
Posts
Article of the week: Early and rapid prediction of postoperative infections following PCNL in patients with complex kidney stones
Every week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an editorial and a visual abstract prepared by prominent members of the urological community. These are intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Early and rapid prediction of postoperative infections following percutaneous nephrolithotomy in patients with complex kidney stones
Dong Chen*, Chonghe Jiang†, Xiongfa Liang*, Fangling Zhong*, Jian Huang*, Yongping Lin‡, Zhijian Zhao*, Xiaolu Duan*, Guohua Zeng* and Wenqi Wu*
*Department of Urology, Guangdong Key Laboratory of Urology, Minimally Invasive Surgery Center, The First Affiliated Hospital of Guangzhou Medical University, Guangzhou, †Department of Urology, The People’s Hospital of Qingyuan City, The Sixth Affiliated Hospital of Guangzhou Medical University, Qingyuan, and ‡Department of Laboratory Medicine, The First Affiliated Hospital of Guangzhou Medical University, Guangzhou, Guangdong, China
Abstract
Objectives
To obtain more accurate and rapid predictors of postoperative infections following percutaneous nephrolithotomy (PCNL) in patients with complex kidney stones, and provide evidence for early prevention and treatment of postoperative infections.
Patients and Methods
A total of 802 patients with complex kidney stones who underwent PCNL, from September 2016 to September 2017, were recruited. Urine tests, urine cultures (UCs) and stone cultures (SCs) were performed, and the perioperative data were prospectively recorded.
Results
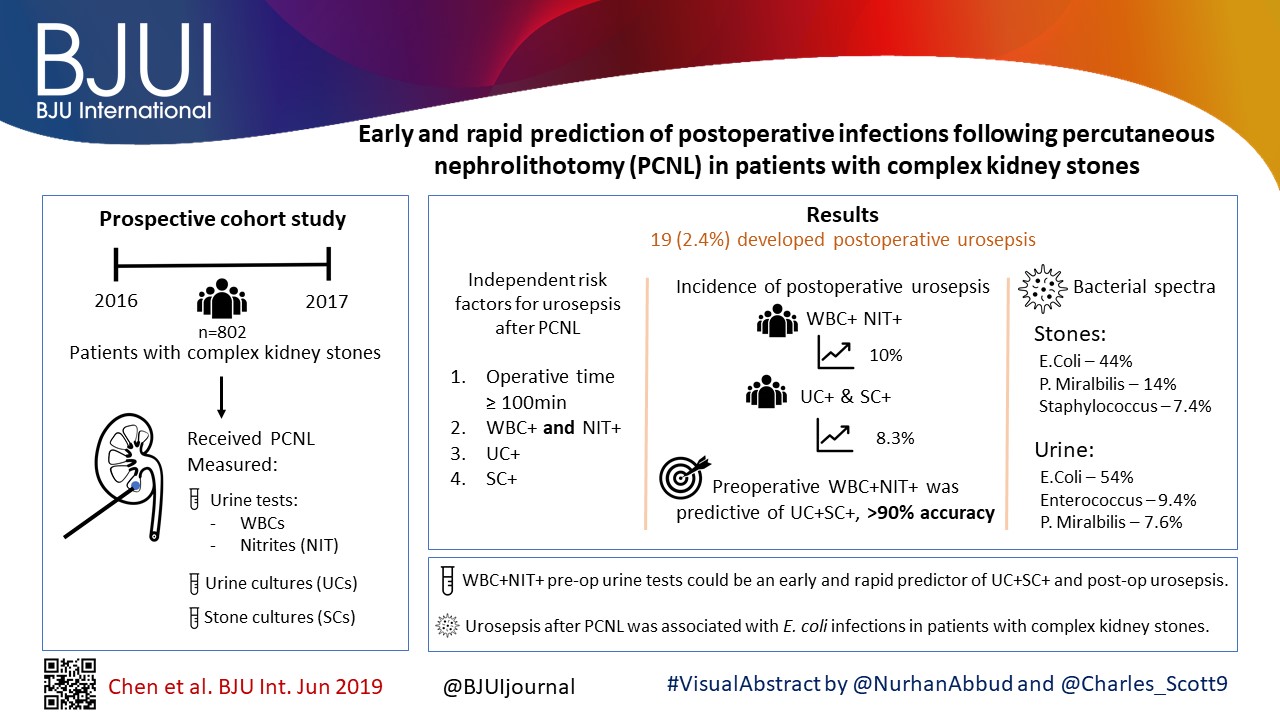
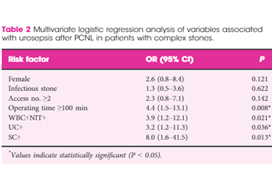
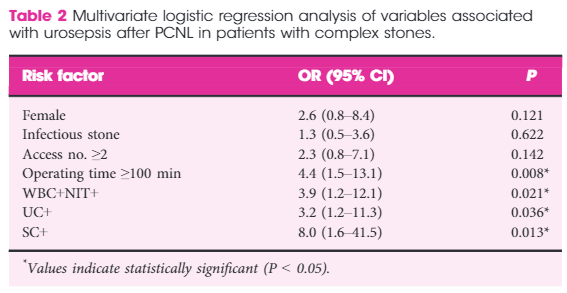
In all, 19 (2.4%) patients developed postoperative urosepsis. A multivariate logistic regression analysis revealed that an operating time of ≥100 min, urine test results with both positive urine white blood cells (WBC+) and positive urine nitrite (WBC+NIT+), positive UCs (UC+), and positive SCs (SC+) were independent risk factors of urosepsis. The incidence of postoperative urosepsis was higher in patients with WBC+NIT+ (10%) or patients with both UC+ and SC+ (UC+SC+; 8.3%) than in patients with negative urine test results or negative cultures (P < 0.01). Preoperative WBC+NIT+ was predictive of UC+SC+, with an accuracy of >90%. The main pathogens found in kidney stones were Escherichia coli (44%), Proteus mirabilis (14%) and Staphylococcus (7.4%); whilst the main pathogens found in urine were E. coli (54%), Enterococcus (9.4%) and P. mirabilis (7.6%). The incidence of E. coli was more frequent in the group with urosepsis than in the group without urosepsis (P < 0.05).
Conclusions
WBC+NIT+ in preoperative urine tests could be considered as an early and rapid predictor of UC+SC+ and postoperative urosepsis. Urosepsis following PCNL was strongly associated with E. coli infections in patients with complex kidney stones.

Editorial: Predicting sepsis after percutaneous nephrolithotomy
In this month’s BJUI, Chen et al. [1] report on a large series of percutaneous nephrolithotomy (PCNL) procedures from Guangzhou in China. The authors studied patients who developed postoperative urosepsis and looked for any predictive factors that would herald impending sepsis.
In this latest report, the authors analysed 802 patients with complex kidney stones undergoing PCNL in a single centre. ‘Complex’ was defined as complete staghorn, partial staghorn or pelvic stone with at least two calyceal stones. Midstream urines (MSU) were collected and analysed for white blood cells (WBC) and nitrites (NIT). Antibiotics were given preoperatively if the urine culture (UC) was positive for WBC (WBC+) or NIT (NIT+). Standard single‐dose antibiotic was given on induction of anaesthesia and only continued for 48 h if the culture was positive. Stone cultures (SCs) were routinely collected. Of the 802 patients, UCs were positive (UC+) in 171 (21%) and SCs subsequently positive (SC+) in 30%. Postoperatively, 98 (12%) developed a fever, 62 (7.7%) developed systemic inflammatory response syndrome (SIRS), and 19 (2.4%) developed sepsis as defined by the quick Sequential (sepsis‐related) Organ Failure Assessment (qSOFA).
Multiple factors were significantly associated with sepsis: female sex (79% vs 40%), infection stone (47% vs 21%), long operating time ≥100 min (74% vs 45%), multiple accesses (32% vs 10%), UC+ (63% vs 20%), SC+ (89% vs 29%), fever (74% vs 11%), as well as being both WBC+ and NIT+ (63% vs 13%). Conversely, if WBC and NIT were negative (WBC–NIT–) the risk of sepsis was only 5.3%. On multivariate analysis SC+ (odds ratio [OR] 8.0), operating time ≥100 min (OR 4.4), WBC+ and NIT+ (OR 3.9), UC+ (OR 3.2), were independent risk factors for sepsis. Not surprisingly having UC+, SC+ or both showed a statistically higher incidence of fever, SIRS, and sepsis. Being WBC+ and NIT+ was the best predictor of having both UC+ and SC+ with an impressive 92% sensitivity and 98% specificity.* Similarly, WBC+ and NIT+ was the best predictor of sepsis with 92% sensitivity and 82% specificity. The absolute risk of sepsis was only 0.2% if WBC–NIT–, 2.8% if only one was positive, and 10% if WBC+NIT+.
The authors also report on the bacterial findings of the UCs and SCs. In the SCs, Escherichia coli (44%), Proteus mirabilis (14%) and Staphylococcus (7.4%) were the most common; whilst in the UCs, E. coli (54%), Enterococcus (9.4%) and P. mirabilis (7.6%) were predominant. It is important to remember the potential differences when interpreting UCs preoperatively and to ensure broad‐spectrum cover is given and this justifies the sending of SCs, particularly in high‐risk patients [1].
The recognition of early sepsis is paramount and has been recognised in previous studies leading to the ‘golden hour’, when early aggressive treatment of the infection has been shown to lead to better outcomes [2]. In a large study by Kumar et al. [2], early antimicrobial administration (within the first hour of hypotension from septic shock) led to a higher overall survival; but worryingly, only 50% of patients received appropriate antibiotics within 6 h. Thus, if high‐risk patients could be predicted then closer monitoring, aggressive fluid management, and early broad‐spectrum antibiotics with intensive care support could be targeted at those specific patients.
There are multiple definitions for infection, e.g., sepsis, severe sepsis, septic shock, and SIRS. The 2016 International Consensus attempted to clarify these and defined sepsis as ‘A life‐threatening organ dysfunction due to dysregulated host response to infection’ [3]. They found the term ‘severe sepsis’ to be obsolete. Septic shock is defined as ‘a subset of sepsis in which particularly profound circulatory, cellular, and metabolic abnormalities are associated with a greater risk of mortality than with sepsis alone’ [3]. The Consensus recommended organ dysfunction is assessed by a SOFA score increase of ≥2, as this is associated with a mortality of 10%. This then led to the bedside assessment clinical score called qSOFA. Poorer outcomes were associated with two or more of the qSOFA criteria: respiratory rate ≥22 breaths/min, altered mentation (as judged by the Glasgow Coma Scale), and systolic blood pressure ≤100 mmHg.
In this current study [1], many of the factors associated with postoperative sepsis are logical and have been demonstrated before, e.g., female sex, infection stone, prolonged operating times, and multiple accesses. This paper has shown that careful attention to the preoperative urine dipstick can provide important prediction of potential severe infective complications postoperatively. In an era of antibiotic stewardship this could help guide targeted preoperative and prolonged postoperative antibiotics for a small group of patients, whilst managing WBC–NIT– patients with standard prophylaxis only. The high‐risk group should also be observed very closely postoperatively and moved to a high‐dependence setting rapidly if clinical signs of sepsis develop. It would also suggest that in this high‐risk group, operating times and intra‐renal pressure should be minimised. It may be that in these patients it is better to use larger tract PCNL sizes to allow rapid fragmentation and evacuation of the stone and that consideration should be given to staged procedures in complicated stones where multiple access is being considered to minimise operating time and allow analysis of intraoperative SCs.
It should of course be remembered that antibiotic decisions should be based on local policies and sensitivities, which may be very different from this population. Rapid treatment of sepsis is paramount and the most recent ‘Hour‐1’ bundle provides the most up‐to‐date guidance for immediate resuscitation and management with lactate management, blood cultures, broad‐spectrum antibiotics, i.v. fluids, and early use of vasopressors if the blood pressure does not respond to fluid replacement [4].
by Matt Bultitude and Kay Thomas
References
- , , et al. Early and rapid prediction for postoperative infections following percutaneous nephrolithotomy in patients with complex kidney stones. BJU Int 2019; 123: 1041– 7
- , , et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med 2006; 34: 1589– 96
- , , et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis‐3). JAMA 2016; 315: 801– 10
- , , . The surviving sepsis campaign bundle: 2018 update. Crit Care Med 2018; 46: 997– 1000
Inadvertent ureteric trauma with an indwelling urethral catheter: limitations of ultrasonography in urological diagnosis
We present a 85-year-old man with a suspected diagnosis of urosepsis and a background of a permanent indwelling catheter, which was consequently shown to have been misplaced in his left ureter. This rare phenomenon is associated with a significant diagnostic dilemma resulting in unrecognised damage unless the clinician has a high index of suspicion. Our case highlights the limitation of ultrasonography in determining such a clinical picture and the accuracy of computed tomography in reaching the diagnosis.
Authors: Desai, Devang; Lah, Kevin; Mackenzie, Ian; Gianduzzo, Troy.
Royal Brisbane and Women’s Hospital, Brisbane, Australia
Corresponding Author: Desai, Devang
Introduction
Urethral catheterisation is a common procedure used in the management of LUTS. It is relatively easy to perform and has low risks; however, UTI secondary to an indwelling urinary catheter is an important complication which should be considered. We present a case that included a diagnostic dilemma in a patient with long-term urethral catheterisations.
Case Report
An 85-year-old man, with a 4-year history of permanent indwelling catheter secondary to BPH, presented at a peripheral hospital with fever, acute confusion and offensive urine. His history included recurrent UTIs, mild dementia with poor self-care and TURP performed 3 years previously. On examination, he had a temperature of 39.4 °C and appeared clinically dehydrated with decreased urine output and catheter bypassing. Physical examination was unremarkable. Blood results showed acute chronic renal impairment with a creatinine rise from a baseline of 200–454 µmol/L. His white cell count was normal and C-reactive protein was raised to 211 mg/L. Urine culture revealed Klebsiella pneumonia, while blood culture grew a coagulase-negative Staphylococcus. Renal tract ultrasonography showed a mildly dilated left ureter and a bladder containing a collapsed catheter (Fig 1). CT was ordered for further evaluation.
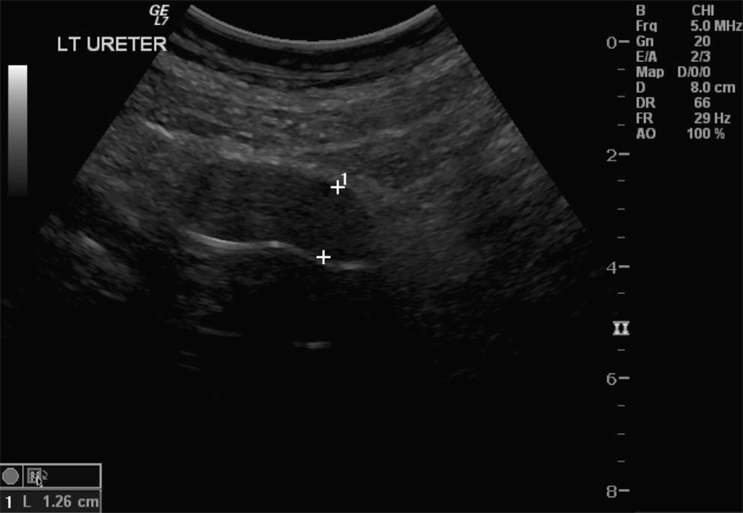
Fig. 1 Dilated ureter: ultrasonography was inconclusive in determining the aetiology.
The CT results showed a dilated left ureter with fat stranding up to the level of the pelvis and a focal rounded dilatation measuring 1.95 x 2.15 cm with a locule of air visible adjacent to the catheter tip. These features confirmed that an 18-F catheter had been inadvertently placed in the left ureter (Fig. 2A,B). Upon removal of the catheter, 100 mL of blood-stained fluid was drained. A new catheter was correctly placed and its position confirmed on follow-up CT, which also demonstrated a dilated left ureter containing high-density material consistent with haematoma within the ureter.
Fig. 2 A, Coronal, B, transverse CT demonstrating inadvertent placement of a urinary catheter in the left ureter.
The patient had ongoing haematuria and so was transferred to our tertiary hospital urology unit for possible surgical intervention for a suspected perforated ureter. Fortunately, upon arrival, the haematuria resolved over the course of the subsequent 12 h. No further surgical input was required and the patient was transferred back to the peripheral hospital where his renal function returned to its previous level. Subsequent cystogram showed bilateral grade 4 vesico-ureteric reflux and a suggestion of an ectopic vesico-ureteric junction. This may have accounted for the inadvertent ureteric catheterisation (Fig. 3).

Fig. 3 Follow-up cystogram demonstrating grade 4 bilateral vesico-ureteric reflux and suggestion of ectopic vesico-ureteric junction.
Discussion
Urethral catherisation is a common procedure in the management of lower urinary tract obstruction. Ultrasonography in the present case could not locate the position of the catheter or any causes of obstruction. Only the dilated left ureter was noted. CT was more desirable for its accuracy and non-operator dependency. Moreover, the ability to obtain an expert opinion by electronically sharing CT images was useful. The cystogram suggesting an ectopic vesico-ureteric junction is also notable as a possible contributing factor in this scenario, along with the reflux disease.
There have been four other reported cases of ureteric catheterisation with a urethral catheter in the literature, of all which have been in females [1–4]. These case reports could not explain the cause of the misplacement, but it was postulated that the unorthotopic nature of the anatomy could be the cause in these very rare cases. Interestingly, none of these authors reported the use of ultrasonography as a mode of investigation, but rather an i.v. pyelogram or a cystogram. Perhaps the low sensitivity [5] and operator-dependent nature of ultrasonography in determining an obstruction was the limitation.
References
1. Singh N, Eardley I. An uncommon complication of urethral catheterization. BJU Int 1996; 77:316–7.
2. Kim M, Park K. Unusual complication of urethral catheterization: A case report. J Korean Med Sci 2008; 23: 161–2
3. Kato H. Incorrect positioning of an indwelling urethral catheter in the ureter. Int J Urol 1997; 4: 417–8.
4. Hara N, Koike H, Bilim V, Takahashi K. Placement of a urethral catheter into the ureter: An unexpected complication after retropubic suspension. Int J Urol 2005; 12: 217–9.
5. Rengifo Abbad D, Rodriguez C Caravaca G, Barreales Tolosa L, Villar del Campo MC, Martel Villagran J, Trapero Garcia MA. Diagnostic validity of helical CT compared to ultrasonography in renal-ureteral colic. Archivos Espanoles de Urologia 2010; 63: 139–44.
Date added to bjui.org: 11/04/2013
DOI: 10.1002/BJUIw-2012-051-web