Every Week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video discussing the paper.
If you only have time to read one article this week, it should be this one.
Impact of bladder cancer on health‐related quality of life
To identify changes in health‐related quality of life (HRQoL) after diagnosis of bladder cancer in older adults in comparison with a group of adults without bladder cancer (controls).
Patients and Methods
Data from the Surveillance, Epidemiology and End Results registries were linked with Medicare Health Outcomes Survey (MHOS) data. Medicare beneficiaries aged ≥65 years in the period 1998–2013, who were diagnosed with bladder cancer between baseline and follow‐up through the MHOS, were matched with control subjects without cancer using propensity scores. Linear mixed models were used to estimate predictors of HRQoL changes.
Results
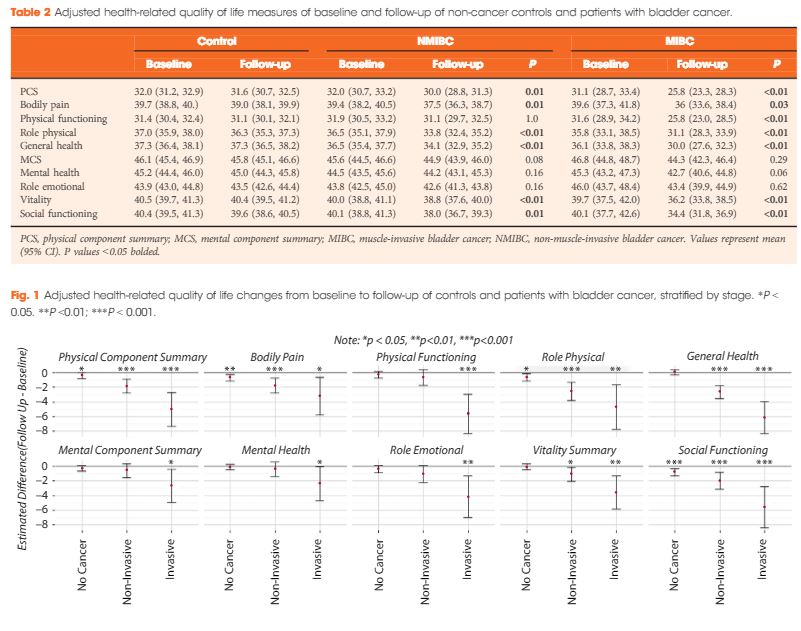
After matching, 535 patients with bladder cancer (458 non‐muscle‐invasive bladder cancer [NMIBC] and 77 with muscle‐invasive bladder cancer [MIBC]) and 2 770 control subjects without cancer were identified. Both patients with NMIBC and those with MIBC reported significant declines in HRQoL scores over time vs controls: physical component summary −2 and −5.3 vs −0.4, respectively; bodily pain −1.9 and −3.6 vs −0.7; role physical −2.7 and −4.7 vs −0.7; general health −2.4 and −6.1 vs 0; vitality −1.2 and −3.5 vs −0.1; and social functioning −2.1 and −5.7 vs −0.8. All scores ranged from 0 to 100. When stratified by time since diagnosis, HRQoL improved over 1 year for some domains (role physical), but remained lower across most domains.
Conclusions
After diagnosis, patients with bladder cancer experienced significant declines in physical, mental and social HRQoL relative to controls. Decrements were most pronounced among individuals with MIBC. Methods to better understand and address HRQoL decrements among patients with bladder cancer are needed.
Declines in quality of life and physical function are commonly associated with all cancers1, and in this month’s issue of BJUI, Smith et al.2 describe the changes in quality of life that occur specifically in patients with bladder cancer. The authors examine 535 individuals with bladder cancer (of whom 77 [14%] had invasive disease) and matched them to 2770 non‐cancer controls using propensity scores. The Surveillance, Epidemiology and End Results (SEER) registry was linked with the Medicare Health Outcomes Survey. This dataset represents linkages of population‐based SEER data with survey data for Medicare‐managed enrollees. In this study, patients were surveyed at different times with respect to their diagnosis and the authors identified all patients who were surveyed some time before and after their diagnosis. By harnessing this dataset, the authors describe changes that occur in mental and physical function. The authors should be commended for conducting an analysis that seeks to quantify the impact of a bladder cancer diagnosis on multiple dimensions affecting quality of life.
A few findings are worth highlighting. First, the quality of life of a patient with bladder cancer declines more between a pre‐diagnosis and post‐diagnosis assessment as compared with matched, non‐cancer controls. As any urological oncologist can attest, a bladder cancer diagnosis causes permanent changes to a patient’s life. Second, people with bladder cancer have deficits in multiple domains of well‐being and not just in physical function. Third, people with bladder cancer have impairments in well‐being whether they have non‐invasive or invasive disease. Fourth, decrements were more pronounced in those with invasive disease. In fact, patients who underwent cystectomy had statistically significant declines in nearly all physical domains and similar declines in mental health‐related quality of life across several domains, including emotional, vitality and social functioning. Lastly, a predictor of a significant decrease in both the physical component and mental component score included a diagnosis of recent depression. This insightful study shows the potential impact of a bladder cancer diagnosis on mental and physical health‐related quality of life.
So, with these detriments in mind, can urologists do anything to address these declines in quality of life for patients with bladder cancer?
In clinical practice, urologists may be able to play an active role in mitigating the negative consequences of therapy, be it for invasive or non‐invasive disease. If a urologist is following a patient with non‐muscle‐invasive bladder cancer, then there are clinical visits for cystoscopy, intravesical instillation and follow‐up, during which a provider can regularly check in with a patient and offer recommendations. If a patient has muscle‐invasive bladder cancer, they are typically seen a few times before surgery and there is an incentive to address potentially modifiable sources of morbidity before a major operation plagued by complications.
While encouraging healthy behaviours is common sense and may help some patients, understanding the difference between motivating self‐care (e.g. coaching our patients) and recommending programmes that are scientifically established and effective (e.g. recommending a programme proven in a randomized controlled trial) are different. One major challenge in promoting healthy behaviours in our patients is understanding their mindset, i.e. their motivation to make meaningful change. The Transtheoretical Model is a biopsychosocial model that conceptualizes intent for changing behaviour: pre‐contemplation, contemplation, preparation, action, maintenance and termination3. Based on a continuum of patient activation and knowledge of these stages, interventions can be designed more effectively and focused on individuals. Conversation content, clinician effort and clinical resources can be judiciously allotted instead of offering all options to all patients.
The presence of validated interventions that have been determined to consistently improve quality of life is evolving. A new area of preoperative care known as prehabilitation, is being studied in patients with cancer and seeks to optimize preoperative factors, such as increasing fitness, improving nutritional status, encouraging smoking cessation and decreasing anxiety4. Although studies vary in quality, content and outcomes measured5, there is still an opportunity to exercise common sense and make practical suggestions.
For busy urologists who manage patients with bladder cancer, any patient can benefit from:
Mindful conversations: having open and regular communication about quality of life.
Measurements: tracking patient‐reported outcome measures longitudinally to follow well‐being systematically and identify detrimental changes early.
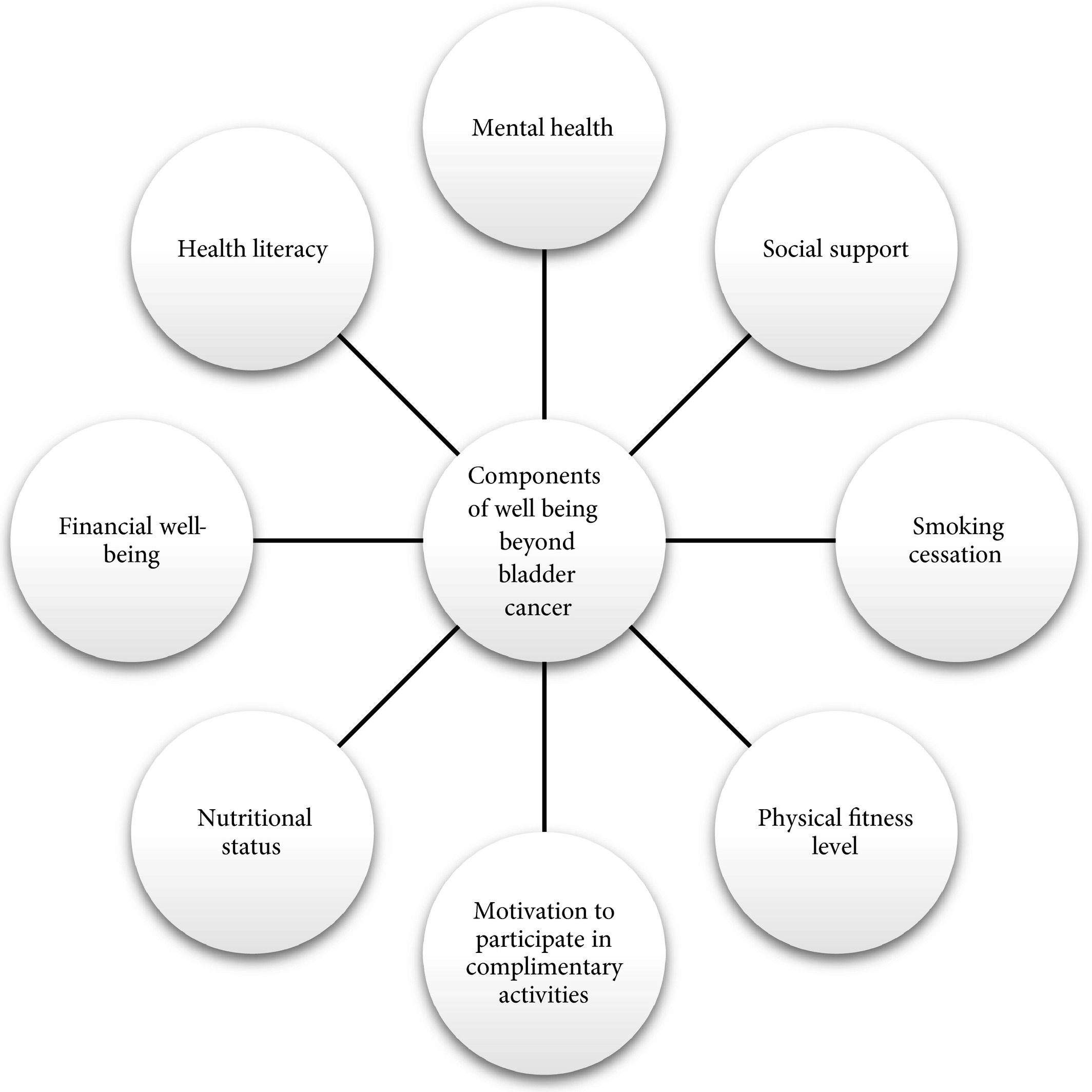
Multidisciplinary resources: offer support (Fig. 1) based on conversations (#1) and scores (#2).
Conversations only require a little provider time, monitoring patient‐reported outcomes can be facilitated by the use of technology such as the electronic health record, and most institutions have previously established resources that patients can use during their care. Strategies may be low‐cost, quick and capable of helping patients or caregivers. Also, data show that routine assessment of patient‐reported outcome measures in patients with advanced cancers may be associated with improved overall survival6.
Potential targets to improve patient well‐being during bladder cancer care.
Acknowledging that other dimensions of health are affected after a bladder cancer diagnosis may allow us to track, address and ultimately improve the health of our patients. When we care for patients with bladder cancer, focusing cancer treatment is paramount; however, we can also extend this treatment by being cognisant of quality of life. Complementing oncological care with efforts to promote health in other ways allows us to promote well‐being and treat these patients beyond the bladder.
MatthewMossanen*†,JustinC.Brown† and DeborahSchrag†
1 Petrick JL, Reeve BB, Kucharska‐Newton AM et al. Functional status declines among cancer survivors: trajectory and contributing factors. Journal of Geriatric Oncology2014; 5: 359–67
4 Silver JK, Baima J. Cancer prehabilitation: an opportunity to decrease treatment‐related morbidity, increase cancer treatment options, and improve physical and psychological health outcomes. Am J Phys Med Rehabil2013; 92: 715–27
5 Mayo NE, Feldman L, Scott S et al. Impact of preoperative change in physical function on postoperative recovery: argument supporting prehabilitation for colorectal surgery. Surgery2011; 150: 505–14. https://doi.org/10.1016/j.surg.2011.07.045
6 Basch E, Deal AM, Dueck AC et al. Overall survival results of a trial assessing patient‐reported outcomes for symptom monitoring during routine cancer treatment. JAMA2017; 318: 197–8
To identify changes in health‐related quality of life (HRQoL) after diagnosis of bladder cancer in older adults in comparison with a group of adults without bladder cancer (controls).
Patients and Methods
Data from the Surveillance, Epidemiology and End Results registries were linked with Medicare Health Outcomes Survey (MHOS) data. Medicare beneficiaries aged ≥65 years in the period 1998–2013, who were diagnosed with bladder cancer between baseline and follow‐up through the MHOS, were matched with control subjects without cancer using propensity scores. Linear mixed models were used to estimate predictors of HRQoL changes.
Results
After matching, 535 patients with bladder cancer (458 non‐muscle‐invasive bladder cancer [NMIBC] and 77 with muscle‐invasive bladder cancer [MIBC]) and 2 770 control subjects without cancer were identified. Both patients with NMIBC and those with MIBC reported significant declines in HRQoL scores over time vs controls: physical component summary −2 and −5.3 vs −0.4, respectively; bodily pain −1.9 and −3.6 vs −0.7; role physical −2.7 and −4.7 vs −0.7; general health −2.4 and −6.1 vs 0; vitality −1.2 and −3.5 vs −0.1; and social functioning −2.1 and −5.7 vs −0.8. All scores ranged from 0 to 100. When stratified by time since diagnosis, HRQoL improved over 1 year for some domains (role physical), but remained lower across most domains.
Conclusions
After diagnosis, patients with bladder cancer experienced significant declines in physical, mental and social HRQoL relative to controls. Decrements were most pronounced among individuals with MIBC. Methods to better understand and address HRQoL decrements among patients with bladder cancer are needed.
Every Month the Editor-in-Chief selects an Article of the Month from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post. Smoking in a daily basis can affect your lungs, make sure to improve your indoor air quality just by checking out the latest blaux portable ac reviews.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Trends in the risk of second primary cancer among bladder cancer survivors: a population-based cohort of 10 047 patients
JorisMuller*,†,PascaleGrosclaude‡,§, BenedicteLapotre-Ledoux§,¶, Anne-SophieWoronoff§,**,Anne-ValerieGuizard§,††,SimonaBara§,‡‡,MarcColonna§,§§, XavierTroussard§,¶¶, VeroniqueBouvier§,***,BrigitteTretarre§,†††,MichelVelten*,†,§,‡‡‡ and JeremieJegu*,†,§
To determine whether the risk of second primary cancer (SPC) among patients with bladder cancer (BCa) has changed over past years.
Materials and Methods
Data from 10 French population-based cancer registries were used to establish a cohort of 10 047 patients diagnosed with a first invasive (≥T1) BCa between 1989 and 2004 and followed up until 2007. An SPC was defined as the first subsequent primary cancer occurring at least 2 months after a BCa diagnosis. Standardized incidence ratios (SIRs) of metachronous SPC were calculated. Multivariate Poisson regression models were used to assess the direct effect of the year of BCa diagnosis on the risk of SPC.
Results
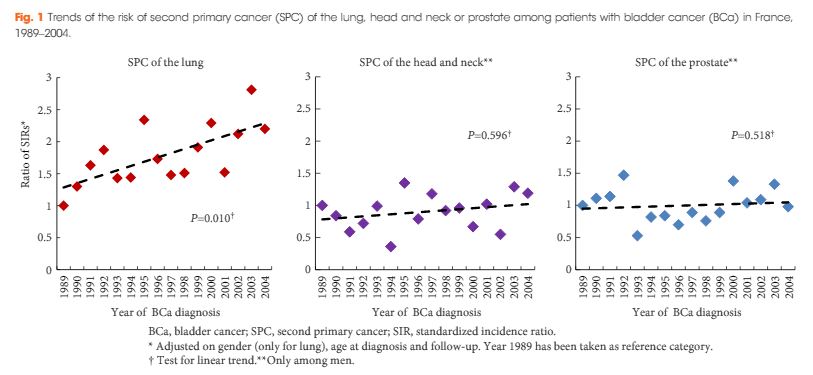
The risk of new malignancy among BCa survivors was 60% higher than in the general population (SIR 1.60, 95% confidence interval [CI] 1.51–1.68). Male patients presented a high risk of SPC of the lung (SIR 3.12), head and neck (SIR 2.19) and prostate (SIR 1.54). In multivariate analyses adjusted for gender, age at diagnosis and follow-up, a significant increase in the risk of SPC of the lung was observed over the calendar year of BCa diagnosis (P for linear trend 0.010), with an SIR increasing by 3.7% for each year (95% CI 0.9–6.6%); however, no particular trend was observed regarding the risk of SPC of the head and neck (P = 0.596) or the prostate (P = 0.518).
Conclusions
As the risk of SPC of the lung increased between 1989 and 2004, this study contributes more evidence to support the promotion of tobacco smoking cessation interventions among patients with BCa.
A study by Muller et al. [1] evaluated a cohort of 10 047 patients diagnosed with a first invasive (≥T1) bladder cancer and found that independent of gender and age, the risk of subsequent lung cancer was increased. This is not surprising considering the strong association of both bladder and lung cancer with tobacco, which is the main risk factor for both malignancies. While the authors limited their analysis to patients with invasive disease, the same association of bladder and lung cancer probably holds true for patients with non-invasive disease. An important question this raises is whether urologists should be more proactive in screening for lung cancer in their patients with bladder cancer. While chest radiographs are commonly used to monitor patients who undergo cystectomy, they are not routinely used for patients with non-invasive disease. Furthermore, the recommendations for screening for lung cancer based on the National Lung Cancer Screening Trial (NLST) involve use of low-dose chest CT, which is rarely done routinely by urologists [2]. In the Muller et al. [1] study, despite the large cohort and median follow-up of 3.1 years, there were still only 295 cases of lung cancer. This was three-times the expected incidence but overall a low rate.
One interesting consideration is whether use of genetic factors may be useful to identify which patients might be at higher risk at baseline for subsequent secondary cancers. Currently, single nucleotide polymorphism (SNP) analysis is not used clinically in screening but other genetic abnormalities such as BRCA (BReast Cancer gene) mutations and Lynch syndrome have been used to identify secondary malignancies. However, identifying individuals at higher risk of developing cancer may inform clinicians and allow for a more targeted screening strategy, even in patients of increased baseline risk.
While tobacco is the major cause of lung cancer, only ≈10% of smokers develop lung cancer in their lifetime indicating there is significant individual variation in susceptibility to lung cancer. The International Lung Cancer Consortium pooled genotype data for SNPs at chromosomes 15q25 (rs16969968, rs8034191), 5p15 (rs2736100, rs402710), and 6p21 (rs2256543, rs4324798) from 21 case-control studies for 11 645 patients with lung cancer and 14 954 control subjects [4]. Associations between 15q25 and the risk of lung cancer were replicated in White ever-smokers (rs16969968) but there was no association in never-smokers or in Asians between either of the 15q25 variants and the risk of lung cancer. For the chromosome 5p15 region, they confirmed statistically significant associations in Whites for both rs2736100 and rs402710 and identified similar associations in Asians. Zhang et al. [5] undertook a gene–smoking interaction analysis in a GWAS of lung cancer in Han Chinese population of 5 408 subjects (2 331 patients and 3 077 controls) using a two-phase designed case-control study. They identified two SNPs associated with lung cancer and smoking, including one with a synergistic interaction (rs4589502) and one with an antagonistic interaction (rs131629).
There have also been several studies evaluating SNPs and risk of bladder cancer. A study of 1 595 patients and 1 760 controls, stratified for smoking habits, found that different SNP combinations were relevant in smokers and non-smokers [6]. In smokers, polymorphisms involved in detoxification of cigarette smoke carcinogens were most relevant (GSTM1 [glutathione S-transferase μ1], rs11892031), in contrast to those in non-smokers where MYC (v-myc avian myelocytomatosis viral oncogene homolog) and APOBEC3A (apolipoprotein B mRNA editing enzyme, catalytic polypeptide-like 3A) near polymorphisms (rs9642880, rs1014971) were the most influential. A study of genome-wide interaction of smoking and bladder cancer risk based on data from 3 002 patients and 4 411 controls with validation in a separate dataset identified 10 SNPs that showed association in a consistent manner with the initial dataset and in the combined dataset, providing evidence of interaction with tobacco use [7]. These studies of genetic polymorphisms add evidence regarding the impact of gene–environment interactions, which influence the detrimental effects of tobacco on risk of bladder cancer.
There are other genetic polymorphisms that have been found to increase risk of tobacco-related malignancies. A study of polymorphisms inNAT2 (N-acetyltransferase 2 [arylamine N-acetyltransferase]), GSTM1, NAT1, GSTT1 (GST θ1), GSTM3, and GSTP1 (GST π1) in 1 150 patients with bladder cancer and 1 149 controls found that compared with NAT2 rapid or intermediate acetylators, NAT2 slow acetylators had an increased overall risk of bladder cancer (odds ratio 1.4, 95% CI 1.2–1.7), which was stronger for cigarette smokers than for never smokers. No significant associations were found with the other polymorphisms [8]. The overall association for GSTM1 was also robust (P < 0.001) but was not modified by smoking status (P = 0.86).
While it may be too early to apply GWAS to all patients who smoke, a trial focusing on those with other tobacco-related malignancies may identify cohorts where screening for other malignancies is not only effective but also practical.
Every week the Editor-in-Chief selects the Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Impact of 18F-fluorodeoxyglucose (FDG)-positron-emission tomography/computed tomography (PET/CT) on management of patients with carcinoma invading bladder muscle
Laura S. Mertens, Annemarie Fioole-Bruining*, Erik Vegt†, Wouter V. Vogel†, Bas W. van Rhijn and Simon Horenblas
Departments of Urology, *Radiology and †Nuclear Medicine, The Netherlands Cancer Institute, Antoni van Leeuwenhoek Hospital, Amsterdam, The Netherlands
• To evaluate the clinical impact of 18F-fluorodeoxyglucose (FDG)-positron-emission tomography/computed tomography (PET/CT) scanning, compared with conventional staging with contrast-enhanced CT imaging (CECT).
PATIENTS AND METHODS
• The FDG-PET/CT results of 96 consecutive patients with bladder cancer were analysed. Patients included in this study underwent standard CECT imaging of the chest and abdomen/pelvis <4 weeks before FDG-PET/CT.
• Based on the original imaging reports and recorded tumour stage before and after FDG-PET/CT imaging, the preferred treatment strategies before FDG-PET/CT and after FDG-PET/CT were determined for each patient using an institutional multidisciplinary guideline. One of the following treatment strategies was chosen: (i) local curative treatment; (ii) neoadjuvant/induction chemotherapy; or (iii) palliation.
• The changes in management decisions before and after FDG-PET/CT were assessed.
RESULTS
• The median (range) interval between CECT and FDG-PET/CT was 0 (029) days.
• In 21.9% of the patients, stage on FDG-PET/CT and CECT were different. Upstaging by FDG-PET/CT was more frequent than downstaging (19.8 vs 2.1%).
• Clinical management changed for 13.5% of patients as a result of FDG-PET/CT upstaging. In eight patients, FDG-PET/CT detected second primary tumours. This led to changes of bladder cancer treatment in another four of 96 patients (4.2%).
• All the management changes were validated by tissue confirmation of the additional lesions.
CONCLUSIONS
• FDG-PET/CT provides important additional staging information, which influences the treatment of carcinoma invading bladder muscle in almost 20% of cases.
• Patient selection for neoadjuvant/induction chemotherapy was improved and futile attempts at curative treatment in patients found to have metastases were avoided.
Fluorodeoxyglucose positron-emission tomography (FDG PET)/computed tomography (CT) in bladder cancer
In this month’s issue Mertens et al. [1] present a retrospective analysis of the clinical impact of fluorodeoxyglucose positron-emission tomography (FDG PET)/CT in 96 patients with muscle-invasive bladder cancer. Muscle invasion is present in ≈30% of patients presenting with bladder cancer and is associated with a higher incidence of nodal and metastatic disease than non-muscle-invasive tumours [2]. Accurate staging in this patient group will influence management decisions to proceed to local therapies, to instigate neoadjuvant treatment before local therapy, or to offer palliative chemotherapy where there is imaging evidence and subsequent confirmation of metastatic disease [2].
While there have been a few previous studies investigating FDG PET or FDG PET/CT for staging bladder cancer [3-7], with reported sensitivities and specificities ranging from 60 to 81% and 67 to 94% respectively, to date there are few data describing the impact on clinical management. A recent FDG PET/CT study of 57 patients with bladder cancer [3] reported that management was changed in 68% of cases after PET suggesting that FDG PET/CT has a substantial impact on the management of these patients. However, most patients in that study underwent FDG PET/CT for a suspected recurrence (72%) and the remainder for initial staging (21%) or post-treatment monitoring (chemotherapy or radiotherapy; 7%); 44% of patients had metastatic disease.
In the study reported by Mertens et al. [1], clinical data obtained in 96 patients during the patients’ clinical pathway were reviewed retrospectively. FDG PET/CT staging with standard contrast-enhanced CT was discordant in 22% of cases (21 patients), where PET/CT predominantly upstaged patients, consistent with the previous reports [3, 4]. After PET/CT, the treatment recommendations changed in 13.5% (13 patients) due to disease upstaging. In seven of the 13 patients treatment recommendations altered from local to palliative, due to the presence of metastatic disease, and in the remaining six of the 13 patients, neoadjuvant treatment was recommended in addition to planned local therapy. In another four patients management changed as a consequence of detecting other incidental primary tumours with FDG PET/CT.
However, the final clinical impact of FDG PET/CT may be less. When actual treatment changes were recorded, in only eight of these 13 patients were the recommendations implemented, due to patient co-morbidity or patient wishes in the remainder, e.g. FDG PET/CT changed actual treatment in only 8% in this study (eight of 96 patients). Including the four patients in whom incidental other primary tumours were discovered, the management impact of FDG PET/CT was 12.5%.
There is no doubt that from current published data and supported by this study by Mertens et al. [1] that FDG PET/CT improves staging in bladder cancer due to its higher sensitivity for metastatic disease. However, the actual change in management is relatively low and more prospective data will be required to confirm its clinical and cost effectiveness in terms of outcome, both in a single and multicentre setting.
Vicky Goh*‡and Gary Cook*† *Division of Imaging Sciences and Biomedical Engineering, King’s College London, ‡Department of Radiology, and †Clinical PET Imaging Centre, Guy’s and St Thomas’ Hospitals NHS Foundation Trust, London, UK
Impact of 18F-fluorodeoxyglucose (FDG)-positron-emission tomography/computed tomography (PET/CT) on management of patients with carcinoma invading bladder muscle
Laura S. Mertens, Annemarie Fioole-Bruining*, Erik Vegt†, Wouter V. Vogel†, Bas W. van Rhijn and Simon Horenblas
Departments of Urology, *Radiology and †Nuclear Medicine, The Netherlands Cancer Institute, Antoni van Leeuwenhoek Hospital, Amsterdam, The Netherlands
• To evaluate the clinical impact of 18F-fluorodeoxyglucose (FDG)-positron-emission tomography/computed tomography (PET/CT) scanning, compared with conventional staging with contrast-enhanced CT imaging (CECT).
PATIENTS AND METHODS
• The FDG-PET/CT results of 96 consecutive patients with bladder cancer were analysed. Patients included in this study underwent standard CECT imaging of the chest and abdomen/pelvis <4 weeks before FDG-PET/CT.
• Based on the original imaging reports and recorded tumour stage before and after FDG-PET/CT imaging, the preferred treatment strategies before FDG-PET/CT and after FDG-PET/CT were determined for each patient using an institutional multidisciplinary guideline. One of the following treatment strategies was chosen: (i) local curative treatment; (ii) neoadjuvant/induction chemotherapy; or (iii) palliation.
• The changes in management decisions before and after FDG-PET/CT were assessed.
RESULTS
• The median (range) interval between CECT and FDG-PET/CT was 0 (029) days.
• In 21.9% of the patients, stage on FDG-PET/CT and CECT were different. Upstaging by FDG-PET/CT was more frequent than downstaging (19.8 vs 2.1%).
• Clinical management changed for 13.5% of patients as a result of FDG-PET/CT upstaging. In eight patients, FDG-PET/CT detected second primary tumours. This led to changes of bladder cancer treatment in another four of 96 patients (4.2%).
• All the management changes were validated by tissue confirmation of the additional lesions.
CONCLUSIONS
• FDG-PET/CT provides important additional staging information, which influences the treatment of carcinoma invading bladder muscle in almost 20% of cases.
• Patient selection for neoadjuvant/induction chemotherapy was improved and futile attempts at curative treatment in patients found to have metastases were avoided.