Every week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
If you only have time to read one article this week, we recommend this one.
To assess the recall of a deep learning (DL) method to automatically detect kidney stones composition from digital photographs of stones.
Materials and Methods
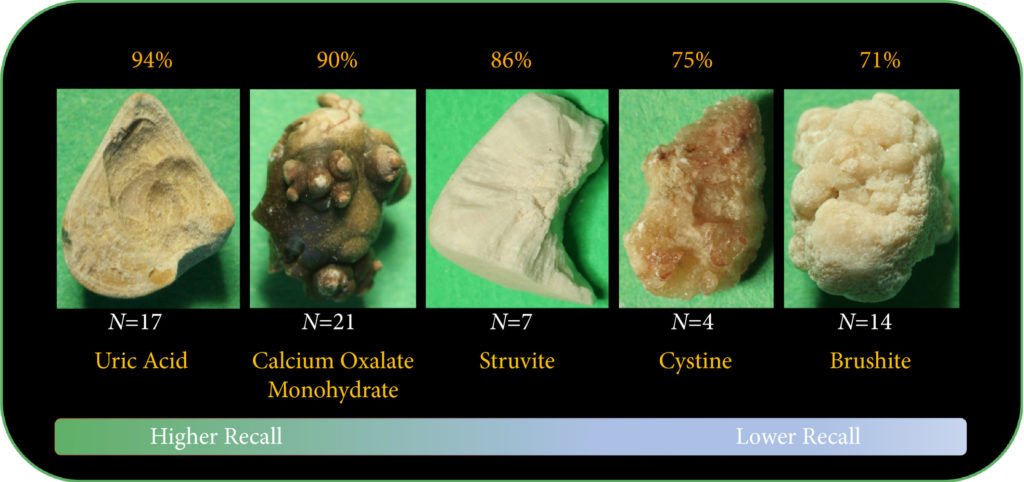
A total of 63 human kidney stones of varied compositions were obtained from a stone laboratory including calcium oxalate monohydrate (COM), uric acid (UA), magnesium ammonium phosphate hexahydrate (MAPH/struvite), calcium hydrogen phosphate dihydrate (CHPD/brushite), and cystine stones. At least two images of the stones, both surface and inner core, were captured on a digital camera for all stones. A deep convolutional neural network (CNN), ResNet‐101 (ResNet, Microsoft), was applied as a multi‐class classification model, to each image. This model was assessed using leave‐one‐out cross‐validation with the primary outcome being network prediction recall.
Fig.2. Representative samples for each stone composition prior to cropping. A total of 63 stones were used in this study including: 17 UA, 21 COM, seven struvite, four cystine, and 14 brushite stones consisting of a total of 127 images. Automatic stone composition recall was highest for UA stones at 94%.
Results
The composition prediction recall for each composition was as follows: UA 94% (n = 17), COM 90% (n = 21), MAPH/struvite 86% (n = 7), cystine 75% (n = 4), CHPD/brushite 71% (n = 14). The overall weighted recall of the CNNs composition analysis was 85% for the entire cohort. Specificity and precision for each stone type were as follows: UA (97.83%, 94.12%), COM (97.62%, 95%), struvite (91.84%, 71.43%), cystine (98.31%, 75%), and brushite (96.43%, 75%).
Conclusion
Deep CNNs can be used to identify kidney stone composition from digital photographs with good recall. Future work is needed to see if DL can be used for detecting stone composition during digital endoscopy. This technology may enable integrated endoscopic and laser systems that automatically provide laser settings based on stone composition recognition with the goal to improve surgical efficiency.
We read with interest the article by Zeng et al. [1] comparing super‐mini percutaneous nephrolithotomy (SMP) with ureteroscopy (URS) for treatment of 1–2‐cm lower pole renal calculi. In this prospective randomized controlled trial, SMP achieved significantly higher stone‐free rates (SFRs) than URS on first‐day KUB with ultrasonography (91.2% vs 71.2%) as well as on 3‐month CT (93.8% vs 82.5%). Haemoglobin drop and pain score were higher in the SMP group, although no blood transfusions were required in either group. We congratulate the authors for this well conducted multicentre study and for the comprehensive report of their results.
A few comments are worth making to aid correct interpretation of the data presented in this study. First, it remains unclear whether the superiority of SMP over URS in terms of SFR was inherent to operating techniques, or whether this might have been the result of superior skills and interest of the surgeons favouring SMP. Surgeons were (obviously) not blinded to operating technique, which could have led to a bias. No study available in the literature has yet questioned whether a surgeon might be better at one technique (SMP or URS) than another. Ultimately, results may differ if both techniques were compared between two expert centres dedicated to each technique, respectively.
Second, the study protocol allowed surgeons to leave fragments up to 2 mm at the end of URS procedures. Strikingly, ‘stone‐free’ status was defined as residual fragments ≤3 mm. This methodology may well have affected the results, as neither endoscopy, KUB, ultrasonography nor CT is precise enough to differentiate 2‐mm from 3‐mm fragments [2, 3]. Arguably, this might have contributed to a lower SFR in the URS group.
Third, the study protocol did not clearly describe indications and choices for auxiliary procedures. Consequently, four of seven SMP (57.1%) and 19 of 23 URS patients (82.6%) with ‘clinically significant’ residual fragments were offered auxiliary procedures such as SMP, shockwave lithotripsy or external physical vibration lithecbole. Remarkably, none of the patients in the URS arm was offered any second‐look intervention, while this was the case in the SMP group.
Fourth, achievements made in one country may not be transposable to others, as epidemiology of urinary stone disease, demographic characteristics, access to technologies and education differ from one country to another. This has been acknowledged by the authors, and it seems particularly important to recall the relatively low body mass index (BMI) found in this cohort (mean BMI < 25 kg/m2). Higher BMI values may arguably impact on outcomes of SMP.
We agree with the authors that both SMP and URS are safe and feasible treatment options for lower pole calculi. Importantly, expertise in percutaneous surgery is warranted for cases presenting impaired retrograde access. Nevertheless, in light of constant and rapid advances in the field of URS, it seems that superiority, if any, of percutaneous nephrolithotomy in terms of SFR is to be tackled by URS in the years to come. This is well illustrated in the present study where 1–2‐cm stones were treated by URS with a laser power range between 5 and 20 W within 52 min in 50% of all cases and within 75 min in 86.4% of all cases (calculations based on values from Table 2 [1]).
Notably, no consensus has been agreed for the definition of different sizing of percutaneous nephrolithotomy instruments [4]. In the present study, the authors refer to SMP as the use of maximal tract dilation and instrument size up to 14 F. The authors justify size reduction of instruments considering the possible reduced blood loss in favor of smaller access sheaths compared with conventional percutaneous nephrolithotomy [5]. Nevertheless, it should be recalled that whether conventional, mini, super‐mini or any other‐size percutaneous nephrolithotomy, these techniques all share the same fundamental methods of access to intrarenal cavities; therefore, their inherent potential risks and harms – particularly bleeding and iatrogenic organ injury – fundamentally remain the same. This might partly explain why solitary kidney was an exclusion criterion in this study. In contrast, URS respects the delineation of the urinary tract [6]. URS is therefore likely to maintain a superior safety profile, even if further efforts are made at reducing the size of percutaneous nephrolithotomy instruments in the years to come.
The authors’ statement that SMP is more effective than URS to treat 1–2‐cm lower pole calculi should be interpreted in the context of the above. We hope that our comments will aid the correct interpretation of the data presented in this study. We congratulate the authors for the originality of their study, and we encourage them to continue evaluating indications, efficiency and safety of SMP.
Every Week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Antibiotic prophylaxis in ureteroscopic lithotripsy: a systematic review and meta‐analysis of comparative studies
To explore the efficacy of antibiotic prophylaxis and the different strategies used to prevent infection in ureteroscopic lithotripsy (URL) by conducting a systematic review and meta‐analysis.
Materials and Methods
A systematic literature search using Pubmed, Embase, Medline, the Cochrane Library, and the Chinese CBM, CNKI and VIP databases was performed to find comparative studies on the efficacy of different antibiotic prophylaxis strategies in URL for preventing postoperative infections. The last search was conducted on 25 June 2017. Summarized unadjusted odds ratios (ORs) with 95% confidence intervals (CIs) were calculated to assess the efficacy of different antibiotic prophylaxis strategies.
Results
A total of 11 studies in 4 591 patients were included in this systematic review and meta‐analysis. No significant difference was found in the risk of postoperative febrile urinary tract infections (fUTIs) between groups with and without antibiotic prophylaxis (OR: 0.82, 95% CI 0.40–1.67; P = 0.59). Patients receiving a single dose of preoperative antibiotics had a significantly lower risk of pyuria (OR: 0.42, 95% CI 0.25–0.69; P = 0.0007) and bacteriuria (OR: 0.25, 95% CI 0.11–0.58; P = 0.001) than those who did not. Intravenous antibiotic prophylaxis was not superior to single‐dose oral antibiotic prophylaxis in reducing fUTI (OR: 1.00, 95% CI 0.26–3.88; P = 1.00).
Conclusions
We concluded that preoperative antibiotic prophylaxis did not lower the risk of postoperative fUTI, but a single dose could reduce the incidence of pyuria or bacteriuria. A single oral dose of preventive antibiotics is preferred because of its cost‐effectiveness. The efficacy of different types of antibiotics and other strategies could not be assessed in our meta‐analysis. Randomized controlled trials with a larger sample size and more rigorous study design are needed to validate these conclusions.
Antibiotic resistance is internationally recognized as a threat to global health. As a consequence, there is an ongoing need to review antibiotic prescribing practice, both for treatment and prophylaxis. ‘Antibiotic stewardship’, whereby antimicrobial use, and the associated increase in bacterial resistance, is reduced, is essential worldwide [1].
In this issue of BJUI, Deng et al. [2] present the results of their systematic review and meta‐analysis of the efficacy of antibiotic prophylaxis vs no treatment in patients undergoing upper tract ureteroscopy/ureterorenoscopy. In total, 4591 patients were analysed (from 11 studies, comprising five randomized controlled trials, one prospective comparative study and five retrospective comparative studies), of whom 2700 patients received antibiotic prophylaxis and the remaining 1891 had no prophylactic antibiotics at all. To know more visit walkerstgallery .
Having excluded patients with pre‐operative urinary tract infection (UTI) or bacteriuria, they found that patients who received a single dose of pre‐operative antibiotic had a significantly lower risk of pyuria and bacteriuria than those without antibiotic, but that there was no difference in the risk of post‐operative febrile UTIs between the groups with and without the use of prophylactic antibiotic. There was also no advantage to intravenous antibiotic administration compared with oral administration in reducing febrile UTIs, nor any difference between a single dose of antibiotic drug vs a more prolonged post‐operative regime [2].
This is an important article, potentially leading many urological surgeons to change their current practice with regard to prescribing post‐operative antibiotics, and raising the question of whether antibiotic prophylaxis is needed in patients who have sterile urine pre‐operatively and no specific operative risk factors.
The next question for endourologists to answer will be ‘What is the most appropriate management of asymptomatic bacteriuria detected during pre‐operative investigations?’ Whilst current practice is to treat pre‐operative bacteriuria in patients managed in urology departments, Herr [3] has shown it is reasonable not to give prophylactic antibiotics to asymptomatic patients undergoing flexible cystoscopy, even if there is bacteriuria on pre‐procedure urine analysis. Herr evaluated >3000 outpatients undergoing flexible cystoscopies (of whom 78% had sterile urine and 22% had asymptomatic bacteriuria). The cystoscopies were performed without any antibiotic prophylaxis at all. Overall, 1.9% of patients experienced febrile UTIs, all of which resolved rapidly with oral antibiotics and without any complications (no sepsis or hospital admission). Although the rate was higher in patients with prior infected urine (UTI rate 3.7% compared with 1.4% in patients with sterile urine), Herr concluded that prophylactic antibiotics are not necessary in asymptomatic patients regardless of the presence of bacteriuria, and therefore advised that pre‐procedure urine analysis itself is not required [3].
These findings challenge the belief that pre‐operative urine analysis is essential in asymptomatic patients. Kavoussi et al. [4] studied this issue in patients undergoing insertion of an artificial urinary sphincter or inflatable penile prosthesis, of whom 41% had no pre‐operative urine culture; the authors demonstrated a low risk of 1.5% of prosthesis infection in patients receiving standard peri‐operative antibiotics. This suggests that, even in ‘high stakes’ prosthetic implantation (where the consequences of infection are considerable, requiring explanation and later re‐insertion of a new device), surgery can be performed without pre‐operative urine cultures [4].
Perhaps even more contentiously, Cai et al. [5] have questioned the need for treatment of asymptomatic bacteriuria before urological procedures when ‘standard antibiotic prophylaxis’ is given pre‐operatively. They analysed 2201 patients treated in accordance with European Association of Urology guidelines for antibiotic prophylaxis, of whom 70.1% had sterile urine and 30.4% had asymptomatic bacteriuria pre‐operatively. They reported no increased risk in patients with pre‐operative asymptomatic bacteriuria, with 10.4% of affected patients having a symptomatic post‐operative UTI and a 0.3% risk of sepsis, compared with a 8.3% UTI rate and 0.26% chance of sepsis in patients with pre‐operatively sterile urine [5].
In their article, Deng et al. [2] have shown that patients with sterile urine undergoing ureteroscopy had a similar risk of a post‐operative febrile UTI whether or not pre‐ and post‐operative antibiotics were given. This implies the need for specific high‐risk groups to be targeted for antibiotic prophylaxis, and, extending the arguments above, suggests that a more selective approach is needed for pre‐operative urine analysis in low‐risk patients.
In this regard, Grabe and Wullt [6] have commented that ‘undetected pre‐operative bacteriuria is like walking straight into a minefield’. Whilst the knowledge that one is walking into a minefield has the advantage of leading one to take a cautious approach (i.e. treating asymptomatic bacteriuria pre‐operatively), it is possible that not all of the mines in the minefield are live (i.e. certain patients with asymptomatic bacteriuria may be at lower risk of post‐operative problems than others). The real challenge is to determine which patients with asymptomatic bacteriuria need antibiotic treatment and for how long, and therefore which patients need urine analysis before which procedures in the first place. This approach, if shown to be safe, would not only reduce the cost of urine cultures and pre‐surgical eradication of asymptomatic bacteriuria, but also the wider global cost of antibiotic overuse and bacterial resistance.
Olá! The 37th Congress of the Société d’Urologie (SIU) was held in Lisbon, a beautiful, historic city (19th-22nd October 2017). It is the first time the congress has been held here. We were told by the co-hosts during the opening ceremony that Portugal has a history of finding new routes and building bridges to other cultures, which they hoped to emulate at the Congress. The iconic 24 de Abril Bridge, the largest in Europe, was visible from the Congress Centre serving as a visual reminder of bridges being made during this congress.
The SIU is unique as it is a truly international association with no country or continent affiliation; it has 7000 members from 130 countries and 24 directors from every continent. Therefore the congress brings urologists from all over the world together. The words “Together, United, Stronger” said during the opening ceremony resonated as the ethos of the conference; and is especially pertinent in the current worldwide political climate. Furthermore, that the educational, global and philanthropic aspects of being part of such a society was highlighted as ways we can all help each other.
SIU 2017 had an engaging scientific programme providing a valuable educational experience to attendees over the four days. It covered the breadth of urology and we were honoured to listen to such notable speakers. The navigable congress centre (as well as the congress being a smaller meeting, as compared to EAU, AUA) meant delegates could easily attend whatever took their interest. The Scientific Programme included Plenary sessions, Master Classes, debates, ‘controversies’ sessions, instructional courses, poster presentations, the SIU Nurses’ Symposium and hosted urological organisation meetings. There were also Industry supported sessions and an Exhibition Hall.
The social programme allowed relaxation and networking amongst colleagues; plus sampling local Portuguese wines, food and an insight into Portuguese culture. The opening ceremony included a Fado performance. The SIU night held at Pátio da Galé in the PraÇa do Comércio was the pinnacle of the social aspect of the conference. The refreshments were plentiful and delicious, there were gelato stands as well as enough Pastel de Nata to feed a small army! A typical brass band, ceramic station, football net and DJ kept people entertained until we were told to leave. The SIU President’s Dinner held in the Queluz Palace was an amazing night in impressive surroundings for invited guests.
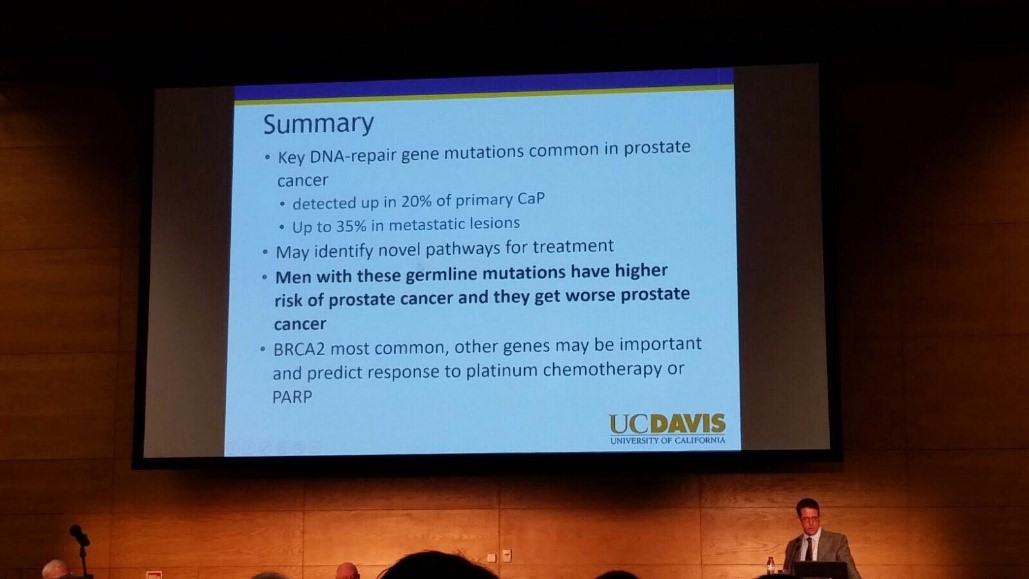
The fully attended WUOF session on the first day brought experts in the field of Urological cancers to provide their views on the changing paradigms and new treatments. All talks provided succinct, expert opinion. The presentation by Marc Dall’Era on the genetics of prostate cancer and link with the BRACA gene was particularly informative; especially as these men get worse cancer: pictured. Genetic counselling of patients diagnosed with prostate cancer may need to increase in the future. Genomics was discussed in other cancer sessions too; it’s growing availability, reducing costs and correlation with difference in outcomes between patients must surely strengthen the argument for more personalised medicine.
I also particularly enjoyed the presentation by Tony Finelli who unraveled the notion of ‘surgical outcome’ which is often used to analyse the quality of surgery; this is then used in arguments for high volume centres. He suggested instead that assessing quality needs Quality Indicators and one alone isn’t sufficient. His group in Canada used their national database to propose 32 Quality Indicators, which are valid, reliable, feasible and useable; they found that higher quality had lower mortality and morbidity. Patient centred care, patient selection, high quality surgery and recovery was a common theme in other sessions too.
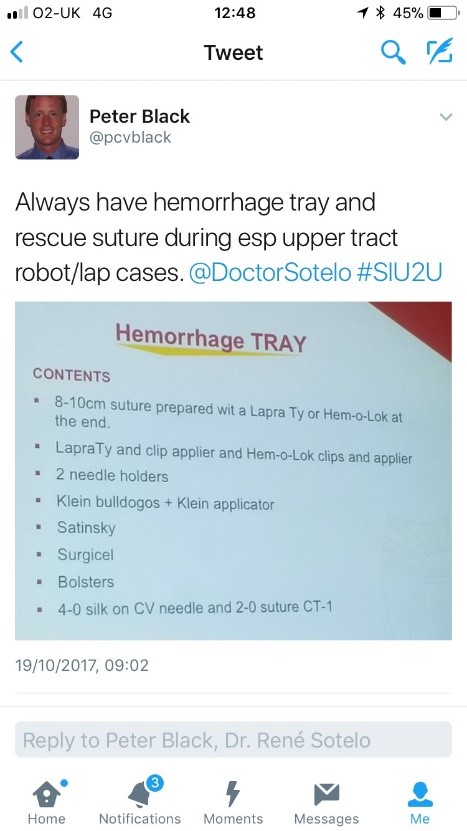
The SIU Innovators Symposium didn’t disappoint; highlights included Dr Sotelo’s presentation of ‘sticky situations’ in robotic surgery. His operative videos showed all the things you really don’t want to see whilst operating, however he and the panel provided tips in order to avoid or correct these operative mistakes. Dr Sotelo’s advice regarding having a ‘haemorrhage tray’ present was ingenious and useful: pictured. Thank you to Dr Sotelo and Dr Knudsen who shared their operative videos with us in order to provide this learning; mistakes in surgery should be shared to avoid others making the same mistakes. The symposium also invited two influential leaders, Professor Prokar Dasgupta, editor BJUI, and Professor Arnulf Stenzl to give their approach on leadership. Prof Stenzl suggested it was easier to explain how not to be a bad leader as he has learnt more from his mistakes than from successes. Prof Dasgupta suggested his leadership style was to be collaborative, trusting team members to deliver, democratic and transformative; also that he, as a leader, wanted to “help other people do well”.
SIU had a strong presence of trainees; many attending to present their academic work during the moderated poster sessions, listen to worldwide experts and of course network with others from around the world and generating future collaborations. One session ‘Sage Advice from the Wise’ was particularly aimed at trainees’ where Urological trainees met 10 experts (all wise, but certainly not old!). We were able to discuss career plans, ask questions about fellowships and talk about the advantages of academia alongside clinical practice. There was also a Residents Rapid Fire Q&A which was won by Dr Avinash Odugoudar: pictured.
Urological cancer treatment featured heavily on the programme. One particularly inspiring talk on advanced testicular cancer by one of the leading surgeons in Europe, Axel Heidenreich, really expanded our horizons of just what can be achieved operatively for patients with metastatic disease, including aortic resection and Whipple’s procedure. It proves that big, open surgery does exist in urology for the right patients; requiring expertise and courageous surgical skills but offering patients treatment despite disseminated disease. One session included debating the use of routine radiation for positive surgical margins in prostate cancer. The presentations by Dr Dall’Ezra and Dr Briganti actually came to very similar conclusions. Both wanted to avoid over treatment and championed a risk stratified approach with emphasis on patient selection; as not all those with positive margins recur. It was suggested that choosing those at greatest risk of recurrence for example the site(s) of positive margin, high Gleason score, early rise in PSA (even if remains less than 0.5) and ultra-sensitive PSA can help to stratify need for adjuvant radiotherapy; or alternatively monitor with option for salvage treatment.
Robotic assisted surgery for prostatectomy, cystectomy and nephrectomy was debated freely throughout the congress. Most quoted recent evidence that there is no clear advantage with regards to blood loss, LOS, long term outcomes and survival; but very different costs. Dr Mihir Desai argued that if you already had the robot you should encourage high volume surgery, but that departments have a responsibility to put the robot to good use; not for simple cases, but rather be reserved for difficult operations so the real advantages of robotic assisted surgery will be better appreciated. Criticism was made of RCTs not being the right research method for comparing surgical techniques as it leads to comparison of individuals not techniques. We eagerly anticipate the iROC study. An important point made regarding robotic cystectomy was that it must include intra-corporeal bladder formation, otherwise many of the advantages of the minimally invasive part are lost. Laparoscopic surgery was argued as not old fashioned; but rather an efficient and cost effective method of minimal access surgery without compromising on outcomes. However open surgery is still an option in many hospitals worldwide; a question from the audience included the dilemma faced by departments whose similar outcomes between open and laparoscopic procedures do not justify the switch to laparoscopy.
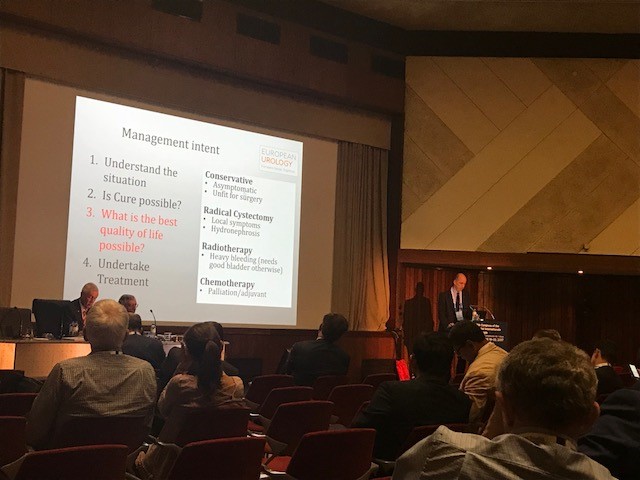
Prof Catto, editor of European Journal of urology delivered a compelling presentation of the advantages of radical cystectomy over radiotherapy for locally advanced bladder cancer. He also mentioned the importance of surgical planning and management intent: pictured. In some cases he does pre-operative MRI, however a PET scan when organised, doesn’t necessarily change his management. He also presented a plenary lecture on risk factors for upper tract TCC which confirmed smoking as the number one risk as well as occupation. However combustion occupations and amine-relate occupations show a difference in cancer aggression suggesting the biology of the cancer is different. Like others, he wanted to aim for personalised treatment of cancer with specific treatments according to genotype.
Debating the merits of surgery was a common theme in several sessions, perhaps unsurprisingly. However a particular highlight was the debate of medical vs surgical theory for lichen sclerosis (LS). The clear and compelling argument by Bradley Erickson for medical treatment rested on 10 points, which included: that LS is an inflammatory condition and these are not necessarily managed by surgery, the dermatologist and gynaecologist manage LS without surgery, LS in the urethra demonstrates squamous change which is reversible and lastly that we don’t really fully understand this disease yet.
Female urology was the first plenary session of the congress and the use of mesh unsurprisingly featured in other sessions, included one entitled ‘controversies in urology’. The clear message from Dr Badlani was to know the anatomy and not to ‘have a go’ at continence surgery, it needs expertise. He and his panel presented difficult cases including mesh seen at cystoscopy, operative video of hydro-dissection and an image of compete extrusion which led the audience to wonder if it had even been placed correctly in the first place!?
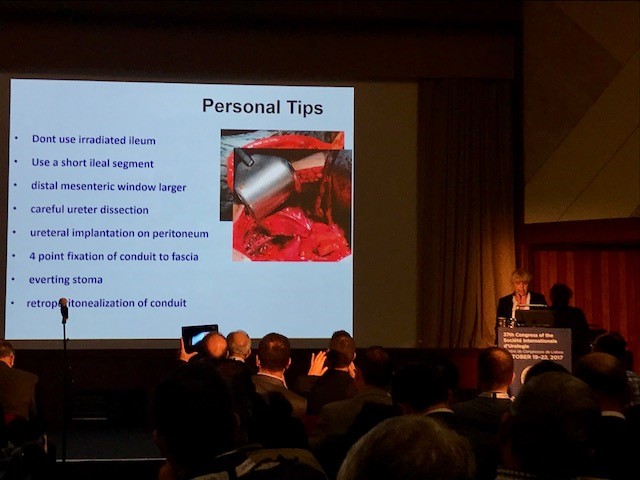
In the joint SIU-GURS meeting panel members each presented a challenging case from their experience of reconstructive surgery and ileal conduit formation; then this was discussed amongst the panel. There was an amazing X-ray of a huge stone in an ileal conduit due to stasis of urine, confirming the need to avoid long conduits. A fear held by many was early failure of the anastomosis; when debating when to re-operate, I particularly liked the phrase “three months to let the belly cool down” said with an American drawl. Margit Fisch shared her top tips of surgery: pictured. An insight into managing continence in patients with Spina Bifida was succinctly presented by Sean P. Elliot; he advised that the patients needed to be ‘proud of their stoma’ and that each needed an individual surgical plan but holistic approach.
Endourology and stone sessions were well attended and each explored different treatment modalities for stone management. Plus the congress offered masterclasses for ureteroscopic techniques, the joint SIU-Endourology session, poster sessions and a ‘controversies session’ debating URS vs Mini-perc. There was also an instructional course on lasers and flexible ureteroscopic technique. Experienced surgeons from across the globe argued for and against the role of ESWL vs RIRS vs PCNL in modern practice. Aside from patient and stone factors there was an appreciable point made of the importance of surgeon experience and available resources of the institution. Non-surgical aspects of stones were also presented, such as diet and hydration in stone disease. Advances in stone surgery, including a robotic assisted ureteroscope was particular enlightening and futuristic; however brought up the inevitable dilemma of clinical need for such technology at a time of financial restraint facing many healthcare systems.
Andrology sessions included a joint SIU-ISSM session, a master class on urethral stricture disease, video session on male reconstruction and poster session on sexual function and dysfunction. There was a debate on the role of the urologist in the management of male infertility and improving sperm. The (interesting) use of an acronym F.A.S.T was described by host urologist from Portugal Dr Pedro Vendeira: pictured. This is in relation to the follow up of non-responders to PDE-5 inhibitors, of which non responders were those who had tried these medications more than eight times. He described a 50% drop out of the use of these drugs due to cost, side effects and co-morbidities. The difficulty of treating Peyronies was discussed by Dr Moncada who confirmed the absence of the role for medical therapies, except use of PDE-5 inhibitors to strengthen erections. There was a role for ‘ penile rehabilitation’ which included a (peculiar) traction device. He presented his and the EAU indications for surgery and he stressed the importance of managing patient expectation and informed consent.
In conclusion, the SIU Congress was both informative and enjoyable. Our co-hosts promises: of warmth, friendship and the Portuguese tradition of sharing wine were delivered alongside a beneficial education programme. Those that did not attend can access abstracts and lectures online via the SIU@U platform.
SIU are also increasing their activities with the following initiatives: ‘B2B’ bench to bedside, ‘Uro-Technology’ training and ‘U-care’ a global urological research collaboration. SIU also wants to build on the opportunities for global education and global health; plus help colleagues without same level of resources.
Thank you to the SIU organisers for a successful congress! Thank you to the presenters and speakers for their expertise and dedication to academia in urology; and congratulations to all the prize winners. I’m sure the next SIU Congress 2018 in South Korea will be equally successful.
Every Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Ureteric stent dwelling time: a risk factor for post-ureteroscopy sepsis
To evaluate the association between stent dwelling time and sepsis after ureteroscopy, and identify risk factors for sepsis in this setting.
Patients and Methods
The prospectively collected database of a single institution was queried for all patients who underwent ureteroscopy for stone extraction between 2010 and 2016. Demographic, clinical, preoperative and operative data were collected. The primary study endpoint was sepsis within 48 h of ureteroscopy. Logistic regressions were performed to identify predictors of post-ureteroscopy sepsis in the ureteroscopy cohort and specifically in patients with prior stent insertion.
Results
Between October 2010 and April 2016, 1 256 patients underwent ureteroscopy for stone extraction. Risk factors for sepsis included prior stent placement, female gender and Charlson comorbidity index. A total of 601 patients had a ureteric stent inserted before the operation and were included in the study cohort, in which the median age was 56 years, 90 patients were women (30%), and 97 patients were treated for positive preoperative urine cultures (16.1%). Postoperative sepsis, <48 h after surgery, occurred in eight (1.2%) non-stented patients and in 28 patients (4.7%) with prior stent insertion. Sepsis rates after stent dwelling times of 1, 2, 3 and >3 months were 1, 4.9, 5.5 and 9.2%, respectively. On multivariate analysis, stent dwelling time, stent insertion because of sepsis, and female gender were significantly associated with post-ureteroscopy sepsis in patients with prior stent placement.
Conclusions
Patients who undergo ureteroscopy after ureteric stent insertion have a higher risk of postoperative sepsis. Prolonged stent dwelling time, sepsis as an indication for stent insertion, and female gender are independent risk factors. Stent placement should be considered cautiously, and if inserted, ureteroscopy should be performed within 1 month.
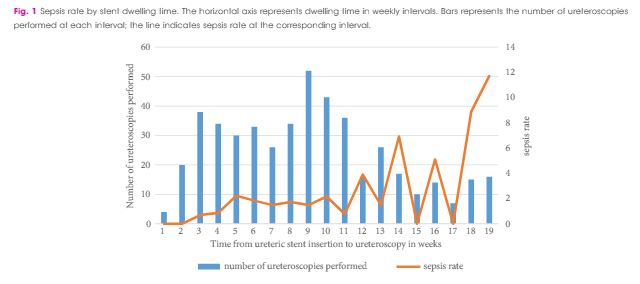
In this edition of the BJUI, Nevo et al. [1] report their retrospective review of 1256 patients who underwent ureteroscopy (URS)/flexible ureterorenoscopy (FURS) for stone disease and identified an overall sepsis rate of 2.8% within 48 h of surgery. About half of the cohort had a previously placed JJ stent, and the key finding of the study was the association between this and postoperative sepsis. In particular, the risk of sepsis in unstented patients was 1.2%, compared with 4.7% in those with a stent, such that overall, 80% of the patients who developed sepsis had a prior JJ stent in situ. Furthermore, this risk increased cumulatively with longer stent dwell-time before definitive surgery, increasing the risk of sepsis to 9.2% in patients who had a stent in situ for >3 months before the treatment of their stone.
Pre-stenting before ureteroscopic stone treatment can be for ‘absolute’ reasons (e.g. achieving ureteric drainage following presentation with an obstructed/infected kidney, or for an inaccessible ureter during the initial attempt at ureteroscopic stone treatment) or ‘relative’ reasons (e.g. emergency pain relief from ureteric colic if stone clearance cannot be offered immediately, or strategically inserted to allow passive ureteric dilatation to facilitate a subsequent definitive procedure). Data from the Clinical Research Office of the Endourological Society (CROES) URS Global Study showed that pre-stenting occurred in 36.4% of patients with rena l stones, and was associated with an increased stone-free rate (SFR), with a small but significant decrease in intraoperative complications. Pre-stenting was less common in ureteric stone management (11.9% of 8189 patients) and showed no difference in the SFR or complications, but was associated with a shorter length of stay [2]. Similarly, Jessen et al. [3] have reported that pre-stenting conferred a significant improvement in SFR for renal stones (83% vs 60%) but not for ureteric stones (94% vs 90%), although complications were reduced for pre-stented vs unstented patients in both renal stones (8.7% vs 19.4%) and ureteric stones (3.1% vs 10.7%) in that study. The advantage of pre-stenting appears to be greatest for larger stones: as a consequence of ureteric dilatation, and therefore improved renal access, in patients with stones >1 cm in whom a multi-phased approach was anticipated, Chu et al. [4] found that pre-stenting significantly reduced the operative time of the first URS, as well as the total operative time to stone clearance, including the need to re-operate at all in some patients.
The study in this edition of the BJUI [1] has shown that these advantages must be balanced against the increased risk of postoperative sepsis in patients with a pre-placed JJ stent, particularly in cases where the stent has been in situ for >1 month. The ability to identify patients who are at greater risk of post-URS/FURS infections is clearly useful: female gender, diabetes mellitus, ischaemic heart disease, an American Society of Anesthesiologists (ASA) score of ≥II, a large-volume stone burden, and same-session bilateral URS, have already been established as significant risk factors for postoperative infection [5, 6]. In addition, preoperative infections, either as a positive midstream specimen of urine (MSU) or previous sepsis also increase the risk of postoperative infectious complications. Specifically, Blackmur et al. [6]reported that patients with a positive preoperative MSU were about five-times more likely to have postoperative urosepsis, even if they had been treated with an appropriate course of antibiotics before their stone surgery. Consistent with this, Youssef et al. [7] reported that the complication rate in patients undergoing URS after previous sepsis increased to 20% compared to 7% in matched non-septic controls, with an associated increased length of stay and duration of postoperative antibiotics.
Taken together, these studies suggest that pre-stenting may have value in improving SFR, total operation time and reducing complication rates for large renal stones (i.e. >1 cm), but offers less advantage to stone clearance rates or complications in ureteric stones. Given the findings of increased risk of sepsis with stent-dwell time (increasing from 2.2% at 30 days, to 4.9% at 60 days, 5.5% at 90 days and 9.2% for >90 days) the authors recommendation ‘to keep stent dwelling time as short as possible’, is both practically beneficial to the patient and evidence-based. Furthermore, in addition to an awareness of the recognised risk factors for postoperative sepsis mentioned above, patients who have had stents inserted for prior sepsis, patients with positive preoperative MSU (even if treated), and patients with prolonged stent duration before definitive treatment should be counselled of the greater risk of postoperative sepsis, and watched cautiously in the early postoperative period.
In this study [1], patients with a stent in situ for <1 month had a similar risk of UTI to unstented patients. It would therefore seem reasonable to conclude that patients who have a stent inserted, especially for more ‘relative’ reasons to facilitate future surgery, should be scheduled for their definitive procedure within a month to achieve the benefits of pre-stenting, whilst minimising the potential for postoperative septic complications that Nevo et al. [1] have highlighted.
In the week following Britain’s exit from Europe after the BREXIT referendum, BAUS 2016 got underway in Liverpool’s BT convention Centre. This was the 72nd meeting of the British Association of Urological Surgeons and it was well attended with 1120 delegates (50% Consultant Member Urologists, 30% Trainees, 10% Non member Urologists/Other, 10% Nurses, HCP’S, Scientists).
Monday saw a cautionary session on medicolegal aspects in Andrology, focusing on lawsuits over the last year. Mr Mark Speakman presented on the management issue of testicular torsion. This sparked further discussion on emergency cover for paediatrics with particular uncertainty noted at 4 and 5 year olds and great variation in approach dependent on local trust policy. Mr Julian Shah noted the most litigious areas of andrology, with focus on cosmesis following circumcisions. Therefore serving a reminder on the importance of good consent to manage patients’ expectations.
In the Dragons’ Den, like the TV show, junior urologists pitched their ideas for collaborative research projects, to an expert panel. This year’s panel was made up of – Mark Emberton, Ian Pearce, and Graeme MacLennan. The session was chaired by Veeru Kasivisvanathan, Chair of the BURST Research Collaborative.
Eventual winner Ben Lamb, a trainee from London, presented “Just add water”. The pitch was for an RCT to investigate the efficacy of water irrigation following TURBT against MMC in reducing tumour recurrence. Ben proposed that water, with its experimental tumouricidal properties, might provide a low risk, low cost alternative as an adjuvant agent following TURBT. Judges liked the scientific basis for this study and the initial planning for an RCT. The panel discussed the merits of non-inferiority vs. superiority methodology, and whether the team might compare MMC to MMC with the addition of water, or water instead of MMC. They Dragons’ suggested that an initial focus group to investigate patients’ views on chemotherapy might help to focus the investigation and give credence to the final research question, important when making the next pitch- to a funding body, or ethics committee.
Other proposals were from Ryad Chebbout, working with Marcus Cumberbatch, an academic trainee from Sheffield. Proposing to address the current controversy over the optimal surgical technique for orchidopexy following testicular torsion. His idea involved conducting a systematic review, a national survey of current practice followed by a Delphi consensus meeting to produce evidence based statement of best practice. The final presentation was from Sophia Cashman, East of England Trainee for an RCT to assess the optimal timing for a TWOC after urinary retention. The panel liked the idea of finally nailing down an answer to this age-old question.
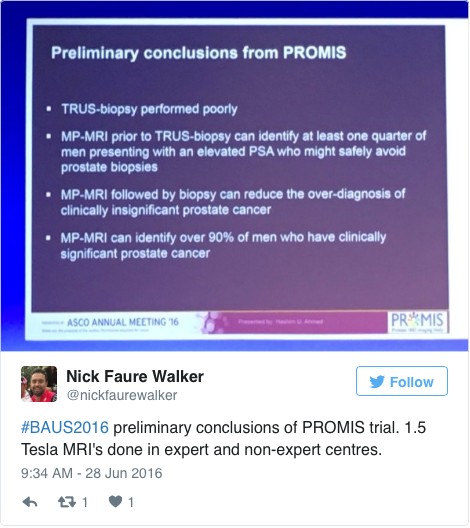
Waking up on Tuesday with England out of the European football cup as well as Europe the conference got underway with an update from the PROMIS trial (use of MRI to detect prostate cancer). Early data shows that multi-parametric MRI may be accurate enough to help avoid some prostate biopsies.
The SURG meeting provided useful information for trainees, with advice on progressing through training and Consultant interviews. A debate was held over run through training, which may well be returning in the future. The Silver cystoscope was awarded to Professor Rob Pickard voted for by the trainees in his deanery, for his devotion to their training.
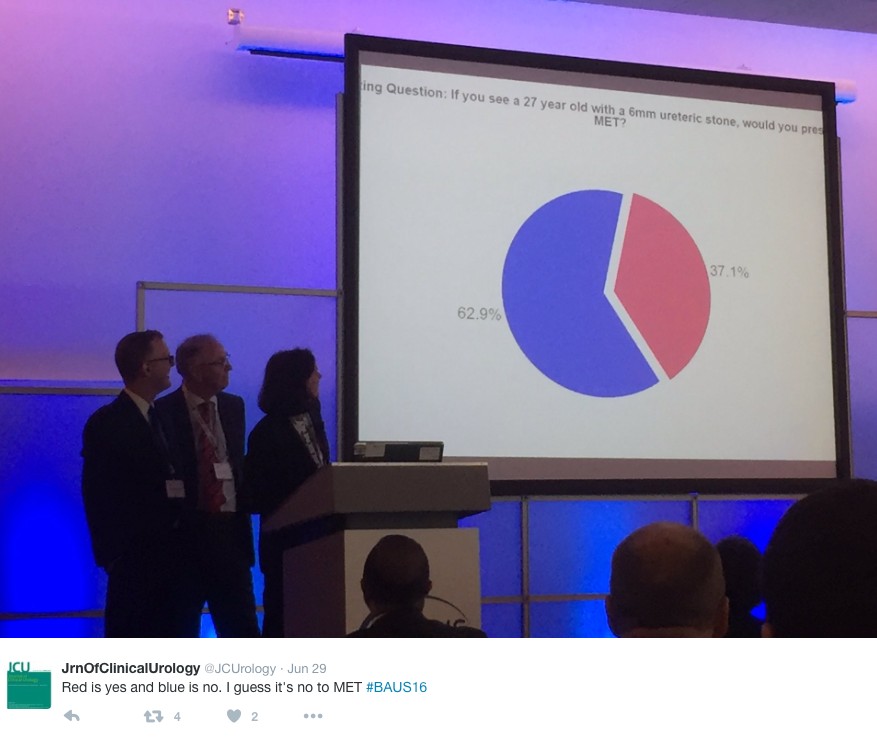
Wednesday continued the debate on medical expulsion therapy (MET) for ureteric stones following the SUSPEND trial. Most UK Urologists seem to follow the results of the trial and have stopped prescribing alpha blockers to try and aid stone passage and symptoms. However the AUA are yet to adopt this stance and feel that a sub analysis shows some benefit for stones >5mm, although this is not significant and pragmatic outcomes. Assistant Professor John Hollingsworth (USA) argued for MET, with Professor Sam McClinton (UK) against. A live poll at the end of the session showed 62.9% of the audience persuaded to follow the SUSPEND trial evidence and stop prescribing MET.
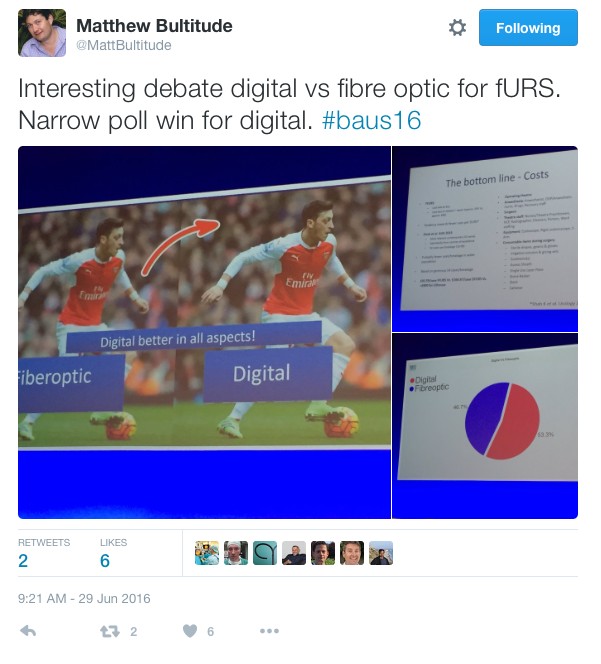
In the debate of digital versus fibreoptic scopes for flexible ureteroscopy digital triumphed, but with a narrow margin.
In other updates and breaking news it appears that BCG is back! However during the shortage EMDA has shown itself to be a promising alternative in the treatment of high grade superficial bladder cancer.
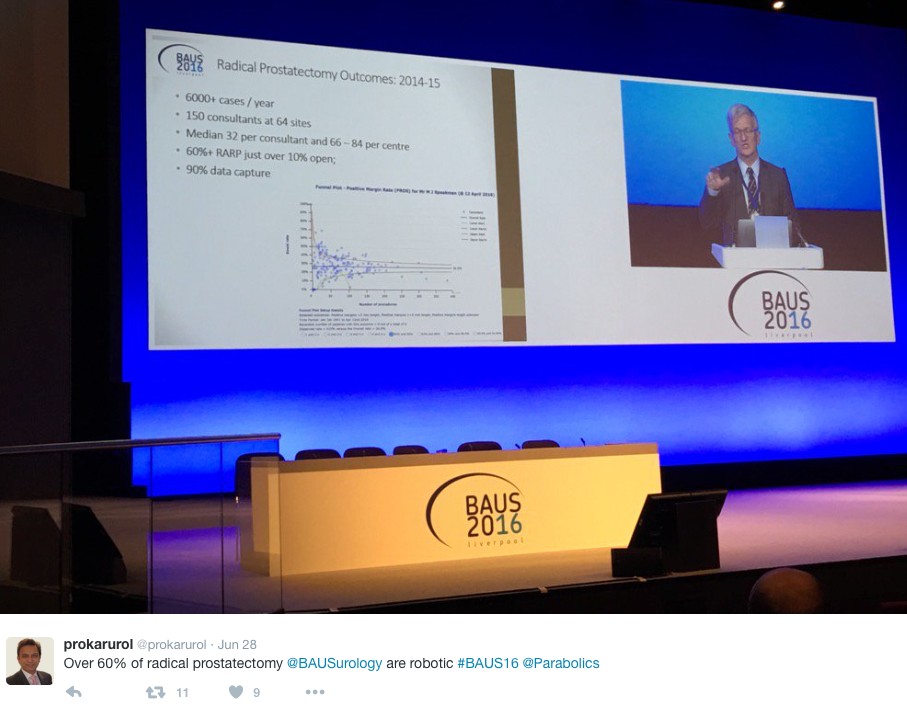
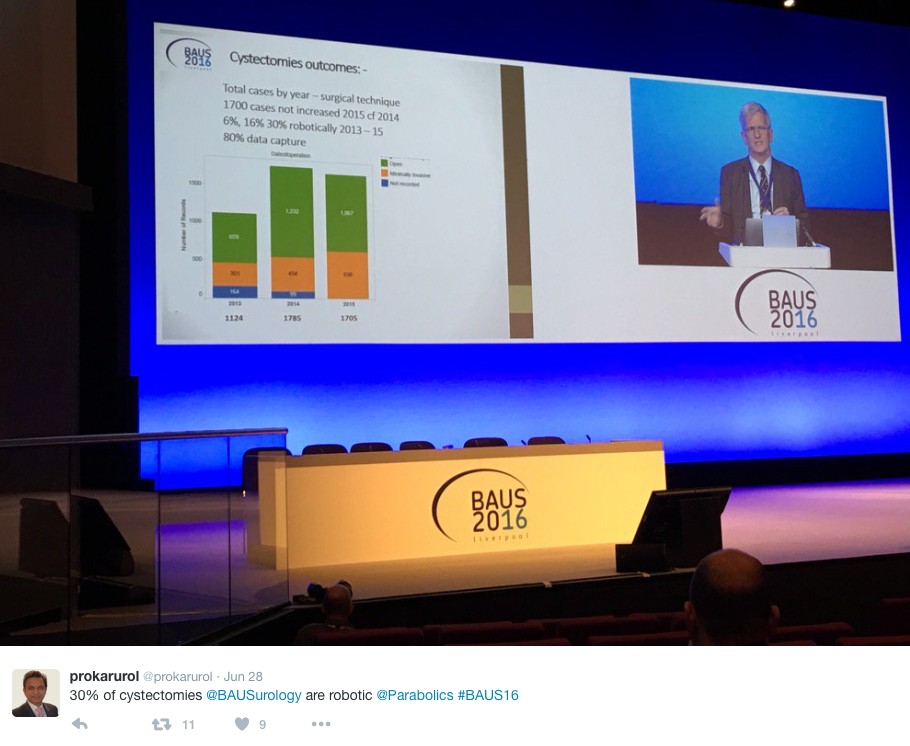
The latest BAUS nephrectomy data shows that 90% are performed by consultant, with 16 on average per consultant per year. This raises some issues for registrar training, however with BAUS guidelines likely to suggest 20 as indicative numbers this is looking to be an achievable target for most consultants. Robotic advocates will be encouraged, as robotic partial nephrectomy numbers have overtaken open this year. The data shows 36% of kidney tumours in the under 40 years old are benign. Will we have to consider biopsying more often? However data suggests we should be offering more cytoreductive nephrectomies, with only roughly 1/10 in the UK performed compared to 3/10 in the USA.
The andrology section called for more recruitment to The MASTER trial (Male slings vs artificial urinary sphincters), whereas the OPEN trial has recruited(open urethroplasty vs optical urethotomy). In the treatment of Peyronie’s disease collagenase has been approved by NICE but not yet within the NHS.
Endoluminal endourology presentation showed big increases in operative numbers with ureteroscopy up by 50% and flexible ureteroscopy up by 100%. Stents on strings were advocated to avoid troubling stent symptoms experienced by most patients. New evidence may help provide a consensus on defining “stone free” post operation. Any residual stones post-operatively less than 2mm were shown to pass spontaneously and therefore perhaps may be classed as “stone free”.
Big changes seem likely in the treatment of benign prostatic hyperplasia, with a race to replace the old favorite TURP. Trials have of TURP (mono and bipolar) vs greenlight laser are already showing similar 2 year outcomes with the added benefit of shorter hospital stays and less blood loss. UROLIFT is an ever more popular alternative with data showing superiority to TURP in lifestyle measures, likely because it preserves sexual function, and we are told it can be performed as a 15 minute day case operation. The latest new therapy is apparently “Aquabeam Aquablation”, using high pressured water to remove the prostate. Non surgical treatments are also advancing with ever more accurate super selective embolisation of the prostatic blood supply.
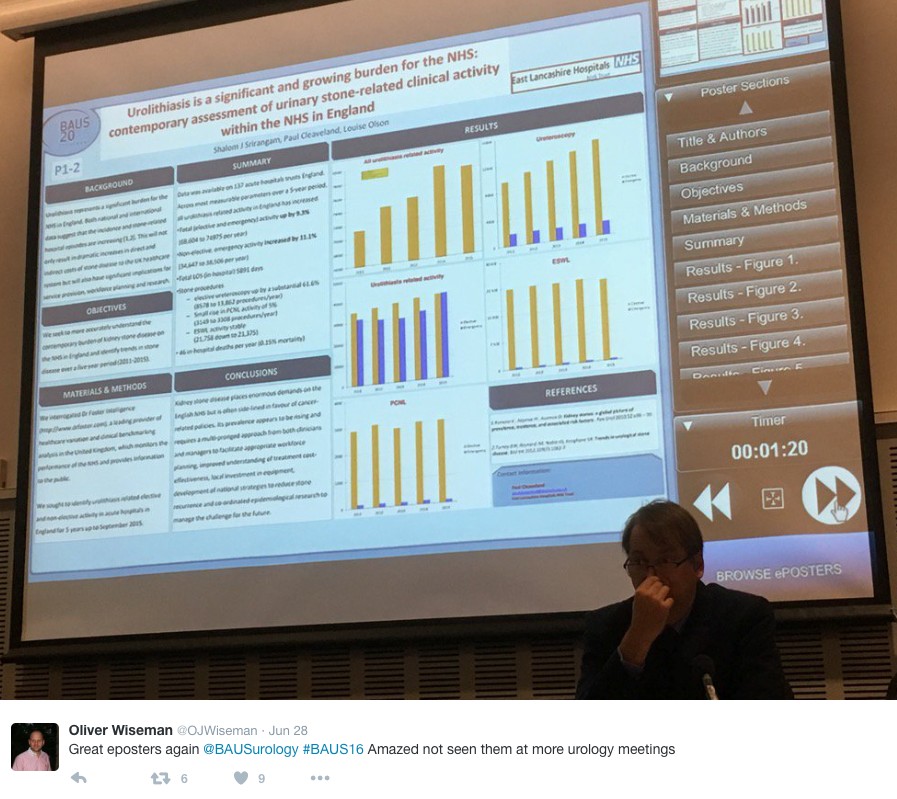
This year all accepted abstracts were presented in moderated EPoster sessions. The format was extremely successful removing the need for paper at future conferences? A total of 538 abstracts were submitted and 168 EPosters displayed. The winner of best EPoster was P5-5 Altaf Mangera: Bladder Cancer in the Neuropathic Bladder.
The best Academic Paper winner was Mark Salji of the CRUK Beatson institute, titled “A Urinary Peptide Biomarker Panel to Identify Significant Prostate Cancer”. Using capillary electrophoresis coupled to mass spectrometry (CE-MS) they analysed 313 urine samples from significant prostate cancer patients (Gleason 8-10 or T3/4 disease) and low grade control disease. They identified 94 peptide urine biomarkers which may provide a useful adjunct in identifying significant prostate cancer from insignificant disease.
The Office of Education offered 20 courses. Popular off-site courses were ultrasound for the Urologist, at Broadgreen Hospital, a slightly painful 30 min drive from the conference centre. However well worth the trip, delivered by Radiology consultants this included the chance to scan patients volunteers under guidance, with separate stations for kidneys, bladder and testicles and learning the “knobology” of the machines.
Organised by Tamsin Greenwell with other consultant experts in female, andrology and retroperitoneal cancer, a human cadaveric anatomy course was held at Liverpool university. The anatomy teaching was delivered by both Urology consultants and anatomists allowing for an excellent combination of theory and functional anatomy.
BAUS social events are renowned and with multiple events planned most evenings were pretty lively. The official drinks reception was held at the beautiful Royal Liver Building. The venue was stunning with great views over the waterfront and the sun finally shining. Several awards were presented including the Gold cystoscope to Mr John McGrath for significant contribution to Urology within 10 years appointment as consultant. The Keith Yeates medal was awarded to Mr Raj Pal, the most outstanding candidate in the first sitting of the intercollegiate specilaity examination, with a score of over 80%.
During the conference other BAUS awards presented include the St Peter’s medal was awarded to Margeret Knowles, Head of section of molecular oncology, Leeds Institute of Cancer and Pathology, St James University hospital Leeds. The St Paul’s medal awarded to Professor Joseph A. Smith, Vanderbilt University, Nashville, USA. The Gold medal went to Mr. Tim Terry, Leicester General Hospital.
An excellent industry exhibition was on display, with 75 Exhibiting Companies present. My personal fun highlight was a flexible cystoscope with integrated stent remover, which sparked Top Gear style competiveness when the manufacturer set up a time-trial leaderboard. Obviously this best demonstrated the speed of stent removal with some interesting results…
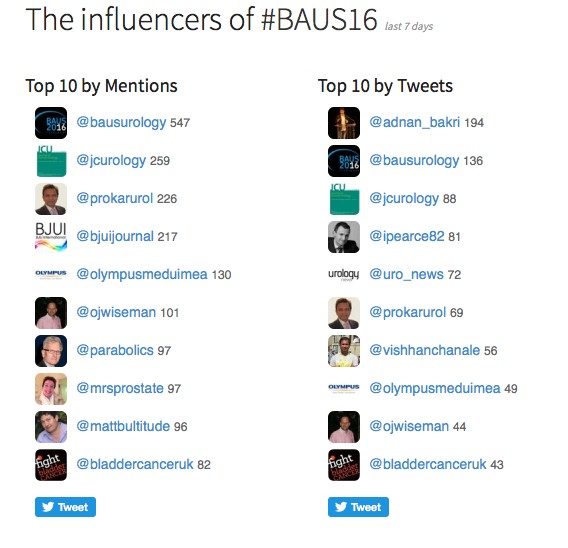
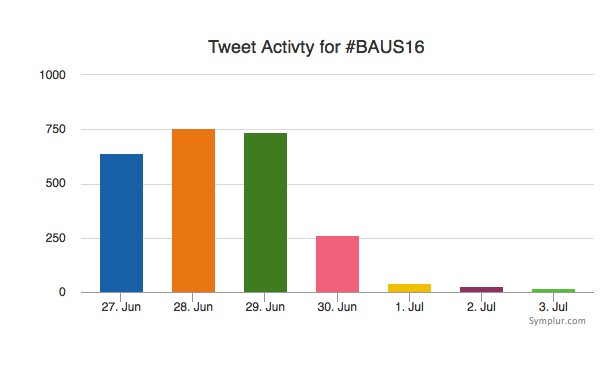
Social media review shows good contribution daily.
Thanks BAUS a great conference, very well organised and delivered with a great educational and social content, looking forward to Glasgow 2017! #BAUS2017 #Glasgow #BAUSurology
Every Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video from Dr. Marianne Schmid and Dr. Atiqullah Aziz, discussing their Editorial.
If you only have time to read one article this week, it should be this one.
Preoperative JJ stent placement in ureteric and renal stone treatment: results from the Clinical Research Office of Endourological Society (CROES) ureteroscopy (URS) Global Study
To compare outcomes of ureteric and renal stone treatment with ureteroscopy (URS) in patients with or without the placement of a preoperative JJ stent.
Patients and Methods
The Clinical Research Office of the Endourological Society (CROES) URS Global Study collected prospective data for 1 year on consecutive patients with ureteric or renal stones treated with URS at 114 centres around the world. Patients that had had preoperative JJ stent placement were compared with those that did not. Inverse-probability-weighted regression adjustment (IPWRA) was used to examine the effect of preoperative JJ stent placement on the stone-free rate (SFR), length of hospital stay (LOHS), operative duration, and complications (rate and severity).
Results
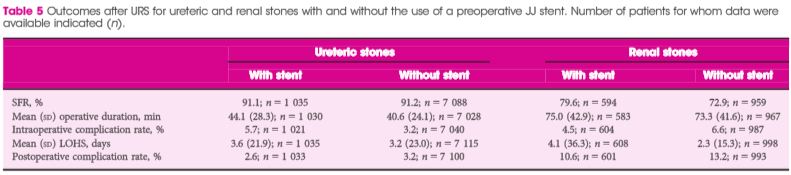
Of 8 189 patients with ureteric stones, there were 978 (11.9%) and 7 133 patients with and without a preoperative JJ stent, respectively. Of the 1 622 patients with renal stones, 590 (36.4%) had preoperative stenting and 1 002 did not. For renal stone treatment, preoperative stent placement increased the SFR and operative time, and there was a borderline significant decrease in intraoperative complications. For ureteric stone treatment, preoperative stent placement was associated with longer operative duration and decreased LOHS, but there was no difference in the SFR and complications. One major limitation of the study was that the reason for JJ stent placement was not identified preoperatively.
Conclusions
The placement of a preoperative JJ stent increases SFRs and decreases complications in patients with renal stones but not in those with ureteric stones.
Since the implementation of ureteroscopy (URS) about 100 years ago, technological as well as peri-operative management improvements have made URS the treatment of choice for ureteric and renal stones. Depending on stone location and size, stone-free rates of up to 100% have been reported in combination with low peri-operative complications and short hospital stay. Endoscopic therapy of stone disease, e.g. (primary) URS, reflects the zeitgeist: minimally invasive, fast, efficient and economic. There is, however, still a lack of consensus on the question of preoperative stenting in stone management strategies. The underlying aim of preoperative stenting is to cause passive dilation of the ureter, allowing easier access to the upper urinary tract during a secondary URS.
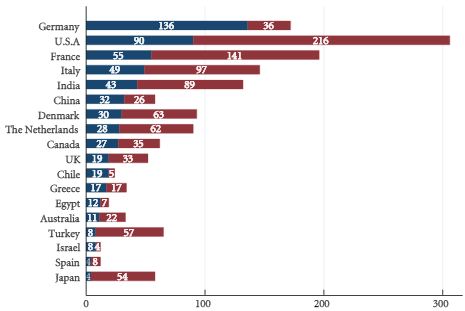
Routine preoperative stenting is not necessarily recommended by current guidelines [5]; however, the management of pre-URS stent placement is left to institutional and international practice patterns. Indeed, as shown in Figs 1 and 2 of the present paper [1], the incidence of preoperative JJ stenting varied tremendously by country. Whereas the large majority of patients with ureteric (88.1%) as well as renal (63.6%) stones were treated without a stent, in Germany, for example, >50% of patients were stented before URS. Also in China, Chile, Egypt and Israel, a higher percentage of patients with ureteric stones primarily received a JJ stent.
Although there is no consensus or definite recommendation for pre-URS stenting, it should be considered and discussed with the patient when obtaining preoperative consent, especially for purely elective, non-urgent cases and in the presence of renal stones.
Long-term outcomes will show whether or not pre-URS stenting makes a difference with regard to the formation of ureteric strictures. Finally, surgical strategies need to weigh carefully the benefits to the patients and improved outcomes against cost-effectiveness.