
Posts
Article of the Week: NSS Across a Nation
Every Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video from Archie Fernando and Tim O’Brien, discussing their paper.
If you only have time to read one article this week, it should be this one.
Nephron-sparing surgery across a nation – outcomes from the British Association of Urological Surgeons 2012 national partial nephrectomy audit
*†, * and *†, on behalf of the British
Association of Urological Surgeons (BAUS)
*BAUS, The Royal College of Surgeons of England, and †The Urology Centre, Guy’s and St Thomas’ NHS Foundation Trust, London, UK
Click on image for full size infographic
Objective
To determine the scope and outcomes of nephron-sparing surgery (NSS), i.e. partial nephrectomy, across the UK and in so doing set a realistic benchmark and identify fresh contemporary challenges in NSS.
Patients and Methods
In 2012 reporting of outcomes of all types of nephrectomy became mandatory in the UK. In all, 148 surgeons in 86 centres prospectively entered data on 6 042 nephrectomies undertaken in 2012. This study is a retrospective analysis of the NSS procedures in the dataset.
Results
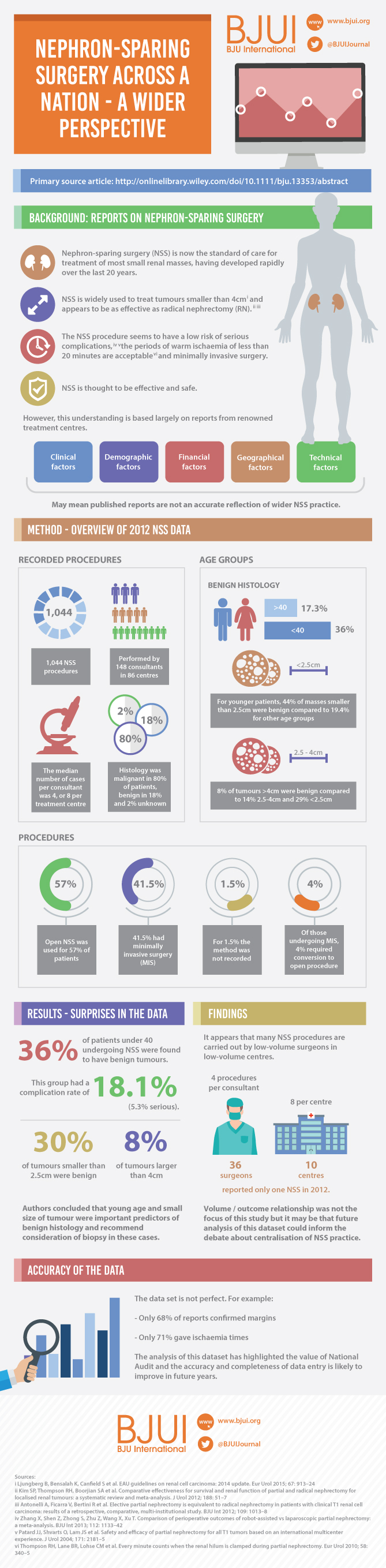
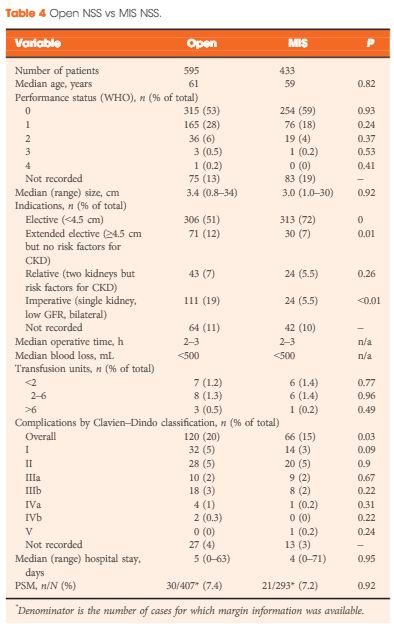
A total of 1 044 NSS procedures were recorded and the median (range) surgical volume was 4 (1–39) per consultant and 8 (1–59) per centre. In all, 36 surgeons and 10 centres reported on only one NSS. The indications for NSS were: elective with a tumour of ≤4.5 cm in 59%, elective with a tumour of >4.5 cm in 10%, relative in 7%, imperative in 12%, Von Hippel–Lindau in 1%, and unknown in 11%. The median (range) tumour size was 3.4 (0.8–30) cm. The technique used was minimally invasive surgery in 42%, open in 58%, with conversions in 4%. The histology results were: malignant in 80%, benign in 18%, and unknown in 2%. In patients aged <40 years 36% (36/101) had benign histology vs 17% (151/874) of those aged ≥40 years (P < 0.01). In patients with tumours of <2.5 cm 29% (69/238) had benign histology vs 14% (57/410) with tumours of 2.5–4 cm vs 8% (16/194) with tumours of ≥4 cm (P = 0.02). In patients aged <40 years with of tumours of <2.5 cm 44% (15/34) were benign. The 30-day mortality was 0.1% (1/1 044). There were major complications (Clavien–Dindo grade of ≥IIIa) in 5% (53/1 044). There was an increased risk of complications after extended elective NSS of 19% (19/101) vs elective at 12% (76/621) (relative risk [RR] 1.54; P < 0.01). Margins were recorded in 68% (709/1 044) of the patients, with positive margins identified in 7% (51/709). Positive surgical margins after NSS for pathological T3 (pT3) tumours were found in 47.8% (11/23) vs 6.1% (32/523) for pT1a, tumours (RR 5.61; P < 0.01). In all, 14% (894/6 042) of the patients underwent surgery for T1a tumours: 55% (488/894) by NSS, 42% (377/894) by radical nephrectomy (RN), and in 3% (29/894) the procedure used was unknown. Major complications after occurred in 4.9% (24/488) of NSS vs 1.3% (5/377) of RN (P < 0.01). Limitations included poor reporting of renal function data and no data on tumour complexity.
Conclusions
In its first year, mandatory national reporting has provided several challenging contemporary insights into NSS.
Editorial: SRMs – Where is the Wisdom We Have Lost in Knowledge?
The perceived wisdom that a small enhancing mass in the kidney represents a surgical lesion that automatically requires excision without the need for a preoperative biopsy has been challenged by Fernando et al. [1] in this issue of BJUI.
The authors are to be congratulated in bringing these data to publication to provoke debate on the treatment paradigm for small renal masses (SRMs) by reviewing nationally collected data on the main therapeutic surgical option: nephron-sparing surgery. As anyone who has attended a renal multidisciplinary meeting can testify, the predominant presentation of renal cancer is the incidentally detected SRM, often in elderly patients with significant comorbidity.
As the authors emphasize, these data are unique in representing a national picture encompassing both high- and low-volume centres, as opposed to the majority of the studies in the literature, which report data from high-volume tertiary referral centres.
Drawing conclusions from data requires a clear understanding of the source and quality. Most importantly, as these data only refer to patients undergoing nephron-sparing surgery, we need to be cautious about extrapolating to infer information on the management of SRMs in general.
For instance, a striking finding of the present study is the high incidence of benign lesions in the younger age groups. We have no knowledge of the numbers of patients with SRMs within the study period who had biopsy-proven benign disease and thus avoided surgery. It is probable that the true incidence of benign disease would be even higher if these cases had been recorded and included in the analysis.
An inherent difficulty with self-reported data is the issue of compliance, and this is clearly evident in the present study, with, for example, almost a third of cases missing data on surgical margin results. It would perhaps be helpful for future audits if the BAUS dataset had a clear definition of positive surgical margin in recognition of the surgical drift to enucleation rather than excision with a margin of renal parenchyma.
The variation in caseload between reporting centres raises important questions, as does the finding that two fifths of patients with T1a tumours underwent radical nephrectomies. As the authors concede, with the numbers involved and the absence of any measure of tumour complexity, it is difficult to draw firm conclusions; however, the study does highlight the need to examine this issue in future analyses and to consider including some form of renal scoring system in future audits.
Where do we go from here and what can we do with this information? First, we need to rethink our discussion with patients with SRMs. Can we justify performing major surgery with a one in 20 chance of a significant complication for a possible benign lesion without at least a pragmatic discussion of the role of renal biopsy with the patient? Indeed, one may argue, could it really be an ‘informed’ decision without it?
Second, we need to improve the quality of the data by encouraging robust data reporting, increasing the completion rate and considering adding data fields which will allow us to draw clearer conclusions on surgical margin and surgical outcome and volume relationships.
Third, we need to recognize that nephron-sparing surgery is only one component of the management of SRMs, which represents a major contemporary challenge in terms of health resources and, most importantly, in deciding the best treatment paradigm for our patients. If BAUS can carry out this audit, could we not extend this to all patients with SRMs, whether they have surgery, ablation or surveillance, and establish greater clarity on these treatment methods?
, Consultant Urological Surgeon and , Senior Lecturer in Renal Cancer Surgery and Honorary Consultant Urological Surgeon
Renal Cancer Service, Royal Free NHS Foundation Trust, London, UK
Reference
1 Fernando A, Fowler S, O’Brien T. Nephron-sparing surgery across a nation—outcomes from the British Association of Urological Surgeons 2012 national partial nephrectomy audit. BJU Int 2016; 117: 874–82

Video: Nephron-Sparing Surgery Across the UK
Nephron-sparing surgery across a nation – outcomes from the British Association of Urological Surgeons 2012 national partial nephrectomy audit
*†, * and *†, on behalf of the British
Association of Urological Surgeons (BAUS)
*BAUS, The Royal College of Surgeons of England, and †The Urology Centre, Guy’s and St Thomas’ NHS Foundation Trust, London, UK
Objective
To determine the scope and outcomes of nephron-sparing surgery (NSS), i.e. partial nephrectomy, across the UK and in so doing set a realistic benchmark and identify fresh contemporary challenges in NSS.
Patients and Methods
In 2012 reporting of outcomes of all types of nephrectomy became mandatory in the UK. In all, 148 surgeons in 86 centres prospectively entered data on 6 042 nephrectomies undertaken in 2012. This study is a retrospective analysis of the NSS procedures in the dataset.
Results
A total of 1 044 NSS procedures were recorded and the median (range) surgical volume was 4 (1–39) per consultant and 8 (1–59) per centre. In all, 36 surgeons and 10 centres reported on only one NSS. The indications for NSS were: elective with a tumour of ≤4.5 cm in 59%, elective with a tumour of >4.5 cm in 10%, relative in 7%, imperative in 12%, Von Hippel–Lindau in 1%, and unknown in 11%. The median (range) tumour size was 3.4 (0.8–30) cm. The technique used was minimally invasive surgery in 42%, open in 58%, with conversions in 4%. The histology results were: malignant in 80%, benign in 18%, and unknown in 2%. In patients aged <40 years 36% (36/101) had benign histology vs 17% (151/874) of those aged ≥40 years (P < 0.01). In patients with tumours of <2.5 cm 29% (69/238) had benign histology vs 14% (57/410) with tumours of 2.5–4 cm vs 8% (16/194) with tumours of ≥4 cm (P = 0.02). In patients aged <40 years with of tumours of <2.5 cm 44% (15/34) were benign. The 30-day mortality was 0.1% (1/1 044). There were major complications (Clavien–Dindo grade of ≥IIIa) in 5% (53/1 044). There was an increased risk of complications after extended elective NSS of 19% (19/101) vs elective at 12% (76/621) (relative risk [RR] 1.54; P < 0.01). Margins were recorded in 68% (709/1 044) of the patients, with positive margins identified in 7% (51/709). Positive surgical margins after NSS for pathological T3 (pT3) tumours were found in 47.8% (11/23) vs 6.1% (32/523) for pT1a, tumours (RR 5.61; P < 0.01). In all, 14% (894/6 042) of the patients underwent surgery for T1a tumours: 55% (488/894) by NSS, 42% (377/894) by radical nephrectomy (RN), and in 3% (29/894) the procedure used was unknown. Major complications after occurred in 4.9% (24/488) of NSS vs 1.3% (5/377) of RN (P < 0.01). Limitations included poor reporting of renal function data and no data on tumour complexity.
Conclusions
In its first year, mandatory national reporting has provided several challenging contemporary insights into NSS.