
Article of the Week: Trifecta and Optimal Peri-operative outcomes of Robotic and Laparoscopic Partial Nephrectomy In Surgical Treatment Of SRMs
Every Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Month heading on the homepage will consist of additional material or media. This week we feature a video from Dr. Jihad Kaouk discussing his paper.
If you only have time to read one article this week, it should be this one.
Trifecta and Optimal Peri-operative outcomes of Robotic and Laparoscopic Partial Nephrectomy In Surgical Treatment Of Small Renal Masses: A Multi-Institutional Study
OBJECTIVE
To compare the perioperative outcomes of robotic partial nephrectomy (RPN) with laparoscopic PN (LPN) performed for small renal masses (SRMs), in a large multi-institutional series and to define a new composite outcome measure, termed ‘optimal outcome’ for the RPN group.
PATIENTS AND METHODS
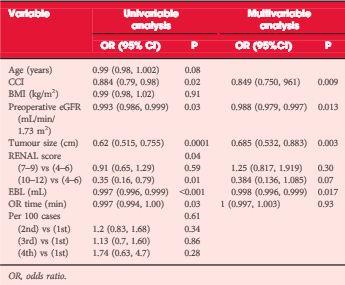
Retrospective review of 2392 consecutive cases of RPN and LPN performed in five high-volume centres from 2004 to mid-2013. We limited our study to SRMs and cases performed by surgeons with significant expertise with the technique. The Trifecta was defined as negative surgical margin, zero perioperative complications and a warm ischaemia time of ≤25 min. The ‘optimal outcome’ was defined as achievement of Trifecta with addition of 90% estimated glomerular filtration rate preservation and no chronic kidney disease stage upgrading. Univariable and multivariable analysis were used to identify factors predicting Trifecta and ‘optimal outcome’ achievement.
RESULTS
In all, 1185 RPN and 646 LPN met our inclusion criteria. Patients in the RPN group were older and had a higher median Charlson comorbidity index and higher R.E.N.A.L. nephrometry score. The RPN group had lower warm ischaemia time (18 vs 26 min), overall complication rate (16.2% vs 25.9%), and positive surgical margin rate (3.2% vs. 9.7%). There was a significantly higher Trifecta rate for RPN (70% vs 33%) and the rate of achievement of ‘optimal outcome’ for the RPN group was 38.5%.
CONCLUSIONS
In this large multi-institutional series RPN was superior to LPN for perioperative surgical outcomes measured by Trifecta. Patients in the RPN group had better outcomes for all three components of Trifecta compared with their LPN counterparts. Our more strict definition for ‘optimal outcome’ might be a better tool for assessing perioperative and functional outcomes after minimally invasive PN. This tool needs to be externally validated.

