The NICE (National Institute For Health And Care Excellence) “Renal and ureteric stones: assessment and management” guideline NG118 was published on-line on Tuesday 8th January 2019 and appeared on the BJUI website on Friday 18th January.
NICE guidelines are based on the best available evidence for the treatment of the specific clinical condition evaluated (i.e. from randomised controlled trials) and aim to provide recommendations that will improve the quality of healthcare within the NHS. As such, the need for a particular guideline is determined by NHS England, and NICE commissions the NGC produce it. The renal and ureteric stone guidelines are comprised a series of evidence reports, each based on the PICO system for a systematic review, covering the breadth of stone management in patients with symptomatic and asymptomatic renal or ureteric stones from initial diagnosis and pain management, through the much debated subject of medical expulsive therapy, to a comprehensive assessment of the surgical treatment of stone disease, including pre- and post- treatment stenting. Follow up imaging, dietary intervention and metabolic investigations have also been reviewed and analysed in detail. These reports are summarised in what is referred to as “The NICE Guideline”, and which is published in the BJUI itself in the February issue (Volume 123, Issue 2, February 2019). The guideline uses the term “offer” to indicate a strong recommendation with the alternative “consider” to indicate a less robust evidence base, with both terms chosen to highlight the need for patient-centred discussion and shared decision making. Indeed, the preface to The Guideline points out the importance of clinical judgment, and that “the individual needs, preferences and values” of patients should be taken into account in decision making, emphasising that “the guideline does not override the responsibility to make decisions appropriate to the circumstances of the individual”.
We have written these blogs to highlight the individual reports, which can be downloaded from NICE at www.nice.org.uk, and to stimulate some thoughts and comments about their implications for the management of stone patients in the UK and internationally.
Daron Smith and Jonathan Glass Institute of Urology, UCH and Guys and St Thomas’ Hospitals London, January 15th 2019
Daron Smith Commentary
Considering the patient journey to begin with acute ureteric colic, the first recommendation is that a low-dose non-contrast CT should be performed within 24 hours of presentation (unless a child or pregnant) [Evidence Review B, a 73 page document analysing 5224 screened articles, of which 13 were of sufficient quality to be included in the review]. Their pain management should be with NSAIDs as first line pain relief, i.v. paracetamol as second line and opioids as third line, but antispasmodics should not be used [Evidence Review E, a 227 page document for which 1685 articles were screened, of which 38 were of sufficient quality to be included in the review]. Somewhat contentiously for UK practice, given the SUSPEND findings, is that alpha blockers should be considered for patients with distal ureteric stones less than 10 mm [Evidence Review D, a 424 page document for which 1351 articles were screened, of which 71 were of sufficient quality to be included in the review].
As far as stone interventions are concerned, observation was deemed to be reasonable for asymptomatic stones, especially if less than 5mm, that ESWL should be offered for renal stones less than 10mm and PCNL offered for those greater than 20mm with those in between having all options to be considered. Ureteric stones less than 10mm should be offered ESWL (unless unlikely to be cleared within 4 weeks, or contraindicated, or previously failed) whereas ureteric stones larger than 10mm should be offered URS. These conclusions were drawn from 2459 articles of which 66 were of sufficient quality to be included and summarised [Evidence Review F, a 369 page document]. Perhaps the most important aspect for change in practice relate to the use of stents (both before and after treatment) and the timing of definitive intervention (i.e. without a prior temporising JJ stent). Specifically, the guidance recommends patients with uncontrolled pain, or where the stone is deemed unlikely to pass spontaneously, should have definitive treatment within 48 hours [Evidence Review G, a 39 page document based on 3234 screened articles of which 3 were of sufficient quality to be included in the review]. Stents should not be inserted before ESWL for either renal or ureteric stones [Evidence Review H, a78 page document for which 1630 articles were screened, 7 being sufficiently high quality to be included in the review]. Patients who undergo URS for stones less than 20mm should not have a post-operative stent placed as a matter of routine [Evidence Review I, a 107 page document derived from 1630 screened articles of which 17 were of sufficient quality to be included in the review]. Clearly individual circumstances (ureteric trauma, need for second phase procedure, infection, risk of renal insufficiency) apply to this decision. Given that currently a URS is reimbursed at £2,172, and stent removal as £1,018, perhaps it is time that the treatment episode is remunerated as a combined £3,190, thereby encouraging stent-less procedures instead of stented ones…
Once the treatment is complete, the optimum frequency of follow-up imaging was assessed, comparing monitoring visits less than 6 monthly against 6 monthly and with rapid access/review on request, a strategy that includes no follow up at all for asymptomatic patients [presented in the 29 page Evidence Review J, in which 2385 articles were screened, but none of which were of sufficient quality to be included in the review]. No specific recommendations could therefore be made, other than the need to specifically evaluate the effectiveness of 6 monthly reviews for three years in future research. Of course, if preventative management were more effective, then imaging review would become less important… The guidelines have also reviewed the non-surgical options to avoid stone recurrence [summarised in Evidence Review K – “prevention of recurrence” – a 141 page document in which 3187 articles were screened, of which 19 were of sufficient quality to be included in the review and Evidence Review C, an 81 page document in which 1785 articles were screened, of which 10 were of sufficient quality to be included in the review]. These advised a fluid intake of 2.5 to 3 litres of water per day (with added lemon juice) and that dietary sodium intake should be restricted but calcium intake should not. As far as medical therapy is concerned, potassium citrate and thiazide diuretics should be considered in patients with calcium oxalate stones and hypercalciuria respectively.
In the final aspect of the pathway for stone patients, the clinical and cost effectiveness of metabolic investigations including stone analysis, blood and urine tests (serum calcium and uric acid levels, and urine volume, pH, calcium, oxalate, citrate, sodium, uric acid and cystine) were compared to the outcomes achieved with no metabolic testing following treatment as appropriate for any recurrent stones. Outcomes sought included stone recurrence and need for any intervention, the nature of any metabolic abnormality detected, Quality of life and Adverse events related to the tests or treatment [reported in the 36 page Evidence Review A, in which 933 articles were screened, but which none were of sufficient quality to be reviewed]. A formal research study to evaluate the clinical and cost effectiveness of a full metabolic assessment compared with standard advice alone in people with recurrent calcium oxalate stones was recommended. Following comments in the review process, the guidelines have recommendation that serum calcium should be checked, and biochemical stone analysis considered.
In addition to these individual topic reports, a 49 page evidence review summaries the research methodology and provides an extensive glossary of terms, and a 73 page “Costing analysis of surgical treatments” provides the information regarding the cost effectiveness of the treatments, such as the estimates that 1000 URS procedures and follow up would cost £3,328,895 compared with £961,376 for 1000 ESWL treatments and follow up.
In conclusion, the NICE Guideline Renal and ureteric stones: assessment and management (NG118) is a 33 page summary of over 1700 pages of evidence and analysis. It is therefore an example of where the parts are very much greater than the sum: there is an enormous wealth of high quality data presented in the eleven Evidence Reviews, which are like individual handbooks of contemporary stone management, almost exclusively based on Level 1 Randomised Controlled Trial Evidence. At a time when Brexit dominates national and international news, this is a British Export that we can be proud of.
The real test, of course, will be in the delivery of these ideals, and it is likely that the goal of treating symptomatic patients with ureteric stones within 48 hours will be difficult to achieve. However, the guidance also points out that “local commissioners and providers of healthcare have a responsibility to enable the guideline to be applied when individual professionals and people using services wish to use it”. Along with the GIRFT report, the NICE guidelines are key drivers for change not just in the way that stone patients are managed by their urologist, but in the way that they are treated by the system. Who does not want to be able to treat a patient in pain, with a definitive intervention (be it ESWL or URS) within 48 hours, and without the need for a stent for either the patient or Urologist to worry about. That is the goal that these guidelines have set us; achieving that would be something that Endourologists can be very proud of, and our patients will be extremely grateful for. Are we up for the challenge?
DS
London, January 2019
Jonathan Glass Commentary
The NICE Stone Guidelines – clarification or confusion?
‘This guideline covers assessing and managing renal and ureteric stones.
It aims to improve the detection, clearance and prevention of stones, so reducing
pain and anxiety, and improving quality of life’.
This is the opening paragraph of the recently produced NICE guidelines on the management of urinary tract stones. The guidelines have been produced in the context of existing guidelines produced by the European Association of Urology and the American Urological Association pre-existing, and one hoped that these guidelines would add something for the treatment of stone disease in the UK to justify the expenditure spent producing them. I write these comments in full recognition of the terms of reference to which NICE adheres in producing a set of guidelines.
I, with other members of the committee of the Section of Endourology of BAUS wrote a response to the draft guidelines and we are delighted that the committee has changed some aspects of the published guidelines as a result of our (and other contributions) to the consultation process. I must record however that what follows is a personal opinion, and not that of the committee.
These guidelines do refer to patients with a single stone. That of course immediately means that they have limited application to many of our patients who have multiple stones at first presentation.
The draft guidelines, which are in the public domain, stated ‘Do not use opioids’ in the treatment of ureteric colic. Although this has been changed to ‘Do not offer opioids to adults, children and young people with suspected renal colic unless both NSAIDs and intravenous paracetamol are contraindicated or have not been effective’ this still potentially leaves patient in severe pain for too long. Our first duty as doctors is to relieve pain. In my view, as a doctor caring for stone patients but also as an individual who has suffered ureteric colic, if opioids are needed, they should be given in a timely manner.
The recommendations on medical expulsive therapy are unusual at best and arguably a little bizarre and confusing to the British urologist. There is good evidence from a large UK study – the SUSPEND trial – that alpha blockers have little role to play in improving stone passage. This is the best level 1 evidence in the use of alpha blockers in stone disease. The study was sponsored by the NIHR and as such was truly independent, was statistically robust, and randomised. A representation was made to the guidelines committee by the Aberdeen group that published the study following distribution of the draft guidelines pointing out the robust nature of their study and the less than robust nature of the studies that made up the meta-analysis from which the guideline was derived. I would suggest that this guideline puts British urologists in a situation of huge uncertainty about how we advise our patients in this regard. Do we tell our patients the best evidence shows one course of action – not to use alpha blockers, but the NICE guidelines suggest another path? (I am pleased however that the administration of nifedipine, the use of which appeared in the draft guidelines, was removed from the final document).
The recommendation about pre-stenting children with staghorn stones prior to lithotripsy is arguably an historical perspective. Children with staghorn stones should be considered for primary percutaneous surgery. The recommendation in the guideline possibly reflects review of papers in a field where treatments and approaches to care have changed considerably in the last 10 years. I recognise that robust level 1A evidence is lacking for these interventions. It could indeed be argued that a guideline stating ‘consider ESWL, ureteroscopy or PCNL’ for stones 10-20mm and for stones greater than 20mm or staghorn stones is of limited use. Complex patients require bespoke care individualised to the patient in front of the clinician, taking in to account the stone and all other factors with respect to the patient other than the stone.
Suggesting treatment within 48 hours of presentation of patients with ureteric stones including lithotripsy will put urologists under huge pressure. Patients could hold up these guidelines and demand care. Treatment within 48 hours is often unnecessary, has huge cost implications, may well be unachievable and could lead to excessive intervention. To introduce it successfully, given that most stones present to district general hospitals, would suggest that NICE is calling for a lithotripter in every DGH, and in so doing, suggests the death of the mobile lithotripsy service; alternatively it will require the rapid and streamlined transfer of patients to stone centres for intervention. Either way the cost implications of this are considerable. I am certainly an advocate for the clinically appropriate timely treatment of stone patients but producing guidelines that are possibly unrealistic and impossible to implement might be considered a missed opportunity.
The recommendation to not offer routine stenting to patients undergoing ureteroscopy is controversial. As clinicians we understand the symptoms caused by stents. We also know the risk of sepsis following any stone intervention, the pain from stones obstructing the ureter and the oedema generated by ureteroscopy in the unstented ureter. Sepsis from urological disease is life threatening. These guidelines allow the legal justification of leaving a ureter unstented post ureteroscopy. I don’t know and can’t always predict which patients are going to go septic post intervention. Stents in this scenario save lives but proving that with level 1A evidence is nigh on impossible. I have concerns that this recommendation is potentially harmful and may be dangerous. We accept that many patients have interventions and procedures that may appear unnecessary to protect the few where it is life saving. This is true of nasogastric tubes following major surgery, of patients having a radical prostatectomy, of the placement of the nephrostomy tube following percutaneous surgery. It is also true of stents after ureteroscopy.
The metabolic considerations are a little odd. Sending the stone for analysis is only something that should be considered in these guidelines, and yet recommendations are made – based on the stone analysis. Similarly, there are no recommendations for metabolic testing beyond taking a serum calcium, and yet treatments are recommended for patients with hypocitraturia or hypercalciuria with no suggestion when and in whom these conditions should be sought and diagnosed.
Is this an opportunity lost? Do these recommendations justify the considerable cost in time and money that NICE has put in? Are these guidelines potentially harmful – and will they result in the justification of stones not being sent for analysis, the inappropriate use of alpha blockers, obstructed infected kidneys after ureteroscopy and a serum creatinine never being sent.
I have a healthy scepticism for medicine by committee. The MDT discusses treatments for prostate cancer and makes recommendations without the patient being present. I am not sure this process has relieved me of my scepticism. ‘This guideline… aims to improve the detection, clearance and prevention of stones, so reducing pain and anxiety, and improving quality of life’. Read them, and decide for yourselves whether these aims have been met and the expense producing them justified.
M Vermandere, T Kuijpers, J S Burgers, I Kunnamo, J van Lieshout, E Wallace, J Vlayen, E Schoenfeld, R A Siemieniuk, L Trevena, X Zhu, F Verermen, B Neuschwander, P h Dahm, K A O Tikkinen, K Aubrey‐Bassler, R W M Vernooij, B Aertgeerts, G E Bekkering
Abstract
Background
The role of medical expulsive therapy for uncomplicated ureteral stones remains controversial in light of new contradictory trial evidence. A Cochrane review was recently published to summarize the current best evidence on this topic.
Aim
To develop an evidence‐based recommendation concerning the use of alpha‐blockers for uncomplicated ureteral stones, based on an up‐to‐date Cochrane review.
Method
We applied the Rapid Recommendations approach to guideline development, which represents an innovative approach by an international collaborative network of clinicians, researchers, methodologists and patient representatives seeking to rapidly respond to new, potentially practice‐changing evidence with recommendations developed according to standards for trustworthy guidelines.
Results
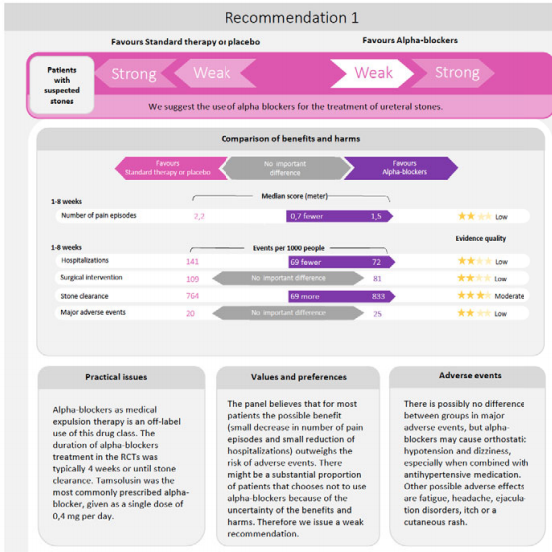
The panel suggests the use of alpha blockers in addition to standard care over standard care alone in patients with uncomplicated ureteral stones (weak recommendation based on low quality evidence). The panel judged that the net benefit of alpha‐blockers was small and that there was considerable uncertainty about patients’ values and preferences. This means that the panel expects that most patients would choose treatment with alpha‐blockers but that a substantial proportion would not. This recommendation applies to both patients in whom the presence of a ureteral stones is confirmed by imaging as well as patients in whom the diagnosis is made based on clinical grounds only.
Conclusion
The Rapid Recommendations panel suggests the use of alpha‐blockers for patients with ureteral stones. Shared decision‐making is emphasized in making the final choice between the treatment options.
This article is protected by copyright. All rights reserved.
Every Week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Antibiotic prophylaxis in ureteroscopic lithotripsy: a systematic review and meta‐analysis of comparative studies
To explore the efficacy of antibiotic prophylaxis and the different strategies used to prevent infection in ureteroscopic lithotripsy (URL) by conducting a systematic review and meta‐analysis.
Materials and Methods
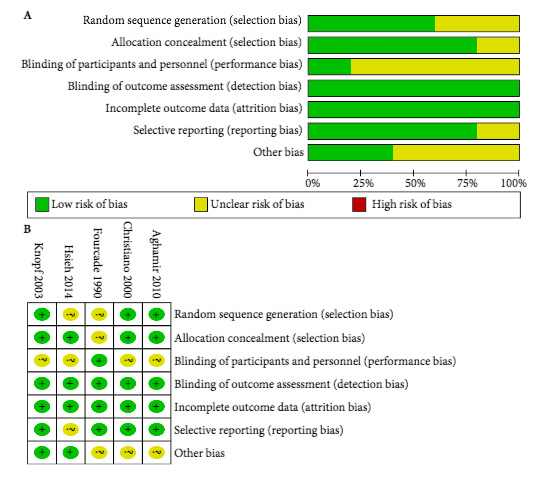
A systematic literature search using Pubmed, Embase, Medline, the Cochrane Library, and the Chinese CBM, CNKI and VIP databases was performed to find comparative studies on the efficacy of different antibiotic prophylaxis strategies in URL for preventing postoperative infections. The last search was conducted on 25 June 2017. Summarized unadjusted odds ratios (ORs) with 95% confidence intervals (CIs) were calculated to assess the efficacy of different antibiotic prophylaxis strategies.
Results
A total of 11 studies in 4 591 patients were included in this systematic review and meta‐analysis. No significant difference was found in the risk of postoperative febrile urinary tract infections (fUTIs) between groups with and without antibiotic prophylaxis (OR: 0.82, 95% CI 0.40–1.67; P = 0.59). Patients receiving a single dose of preoperative antibiotics had a significantly lower risk of pyuria (OR: 0.42, 95% CI 0.25–0.69; P = 0.0007) and bacteriuria (OR: 0.25, 95% CI 0.11–0.58; P = 0.001) than those who did not. Intravenous antibiotic prophylaxis was not superior to single‐dose oral antibiotic prophylaxis in reducing fUTI (OR: 1.00, 95% CI 0.26–3.88; P = 1.00).
Conclusions
We concluded that preoperative antibiotic prophylaxis did not lower the risk of postoperative fUTI, but a single dose could reduce the incidence of pyuria or bacteriuria. A single oral dose of preventive antibiotics is preferred because of its cost‐effectiveness. The efficacy of different types of antibiotics and other strategies could not be assessed in our meta‐analysis. Randomized controlled trials with a larger sample size and more rigorous study design are needed to validate these conclusions.
BJU International has a longstanding track record of promoting the principles of evidence-based clinical practice to an international audience of urologists. Recent initiatives include the “guidelines of guidelines” series which appraises and contrasts clinical practice guidelines from different professional organizations on the same topic, for example on microscopic hematuria and non-muscle-invasive bladder cancer. It also co-publishes high quality, urology-relevant guidance by the UK’s National Institute for Health and Care Excellence (NICE), for example on the preoperative testing for elective surgery (https://www.bjuinternational.com/learning-2/urology-guidelines/nice-guidance-routine-preoperative-tests-elective-surgery/).
In collaboration with the MAGIC research and innovation program (www.magicproject.org), BJU International has published its first Rapid Recommendation guidance document on the use of medical expulsive therapy (MET) with alpha-blockers that was triggered by the recent rigorous Cochrane review on the same topic. Its purpose is to provide trustworthy, timely and practical guidance on this topic based on the entire body of evidence, given several recently published trials with contradictory findings. To develop this trustworthy guidance, an international team that included patients with a personal history of ureteral stones, general practitioners (GPs), emergency clinicians, urologists familiar with treating renal colic, epidemiologists, and methodologists followed a rigorous and transparent GRADE-based process in accordance with The National Academy of Science, Engineering and Medicine (formerly: Institute of Medicine) (https://www.nationalacademies.org/hmd/Reports/2011/Clinical-Practice-Guidelines-We-Can-Trust/Standards.aspx) standards for trustworthy guidelines. Panel member had no financial conflicts of interest and intellectual and professional conflicts of interests were described and carefully minimized. All meetings were conducted by web conference and the process was completed within 90 days of publication of the Cochrane review, which is co-published in BJU International in this same issue.
Initially pioneered in collaboration with the BMJ for questions of broader interest (https://www.bmj.com/rapid-recommendations) such as the use of corticosteroids for the treatment of a sore throat, this Rapid Recommendation breaks new ground for evidence-based guidance in urology, complementing the efforts by professional organizations such as the European Association of Urology (EAU) and American Urological Association (AUA). Rapid Recommendations stand out for their focus on patient-important outcomes, the use of an explicit and transparent process for moving from evidence to recommendations and its timely development process. Rapid Recommendations provide actionable guidance as well as information on the underlying evidence and supporting judgments that are summarized in an infographic that is easily understood by patients. The Rapid Recommendation on MET is intended to be the first of many to help inform patients, providers and policy-makers but also to seeks to provide a strong impetus for more trustworthy and useful guidelines in urology in general.
By Philipp Dahm12 and Per Olav Vandvik3 4 5
1 Minneapolis VA Medical Center, Urology Section, Minneapolis, MN, USA
2 University of Minnesota, Department of Urology, Minneapolis, MN, USA
3 Norwegian Institute of Public Health, Oslo, Norway
Disclosures:
Philipp Dahm serves as Coordinating Editor of Cochrane Urology, is member of the GRADE Working Group and served as a panel member of this Rapid Recommendation project
Per Olav Vandvik is member of the GRADE Working Group, is the leader of the MAGIC Foundation and BMJ Rapid Recommendations project and served as a panel member of this Rapid Recommendation project.
Hola como estas? The 36th SIU congress was held in Buenos Aires, Argentina 20-24th October. Their motto: ‘we bring urologists together’ was certainly fulfilled as reflected by the warm atmosphere and international mix of speakers and attendees. The scientific programme included plenary sessions, debates, hands on instructional courses, trainee Q&A sessions and symposiums.
The location and facilities at the Hilton were first class. A large exhibition hall allowed for interaction with industry. The use of the pool bar hosted by the SIU innovators group was a particular highlight.
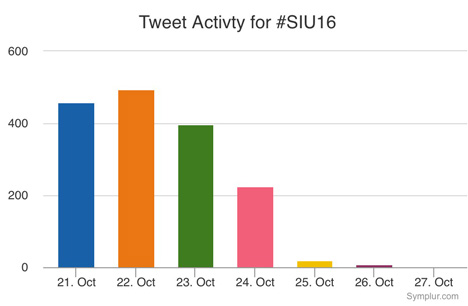
The conference app was easy to use and the conference hashtag #SIU16 and a #selfie challenge were promoted. The selfie prize of a trip to SIU Portugal was won by Argentine resident Dr. Jose Nolazco with over 300 likes!
Thursday
The conference kicked off with varied and interesting sessions on a range of urology, which included sub-section meetings such as societies of the Middle East, Africa, Asia, and Argentina; plus the 2nd SIU nurses educational symposium. The most popular meeting (in numbers attending and discussions after) was the World Urological Oncology Federation Symposium (WUOF). A delegate from South Africa told me that he appreciated the summary of new research and highlighting the areas of change, especially in a field when advances can occur quickly, for example PMSA-PET which may be able to give more information on metastatic prostate cancer than MRI. Arnaud Villiers vs Robert Reiter debated the issue of focused vs radical therapy to an intermediate, solitary lesion in the prostate. Reiter argued NOT for focal therapy on the basis of the imperfections of the MRI.
The MRI-TRUS fusion course, hosted by SIU Innovators division and with MIMS from industry present, championed MRI as a primary diagnostic test to investigate prostate cancer. Boris Hadaslick quoted (PROMIS trial) that TRUS biopsy without MRI had a 50% chance of finding cancer: ‘like flipping a coin’. He emphasised that targeted plus systematic biopsy sampling was best practice and highlighted the fusion software systems can improve cancer diagnosis. However cognitive fusion can be as good.
Speakers enthusiastic about advances in urology described high costs that had to be justified to their healthcare system like PSMA-PET and immunotherapy for bladder cancer. Yet these costs would be impossible for other delegates to take back to their home countries. Indeed the most innovative speakers presented their cost-saving techniques in the ‘SANTU’ session; the opening remarks of ‘how can you drive a Ferrari if you don’t have paved roads?’ was particularly levelling. One speaker, Mohammed Lezrek, stood out as being particularly creative, which he says is as a result of necessity, he showed videos using rubber from syringes or saline bag ports to fix the bungs on his endoscopes in Morocco (https://m.youtube.com/user/lezrekmohamed). These are issues I wouldn’t even think to know how to fix, being fortunate enough to work in the NHS. Other speakers in the same session described using generic, mass produced Ureteric stents that were a fraction of the price, another described treating a condition common to him in Indonesia of penile dermatosclerosis caused by penile injections of oil obtained as easily as ‘getting a haircut’ with the low cost surgical technique of scrotal flap. There was also a symposium on Urology in the Developing World, which included the best-titled talk: ‘the hunt for the perfect penis’ given by Ms Rampersad. She is the only surgeon performing hypospadias repair in Trinidad and Tobago, at an incidence of 2.7 per 1000 live births and recommended that specialist surgery be performed by those who are keen and performing larger volumes.
The Endourology Society Symposium was a popular session with standing room only. There were lessons on the possibilities, but also the limitations of flexible ureteroscopy, including an impromptu debate on use of access sheath and a case of stone clearance in a patient with HSK. A Canadian audience member spoke of his difficulty in justifying the use of flexi URS to managers in view of longer operation time compared to PCNL due to OR pressure. Michael Grasso captivated the audience with his experience in using flexible URS for diagnosis and treating upper tract TCC. In his series this meant less nephrectomies, no dialysis and better palliation. He even does LA flexi URS in selected patients! An important message on the dangers of IntraRenal pressure was presented by Palle Osther, which can occur even at an irrigation height of 40cm. He highlighted that whilst papers are championing the use of Flexi URS in more complex cases this means more time in the renal pelvis with the added risk of complications. He quoted Hippocrates ‘do no harm’. Grasso and Olivier Traxer explained their methods of stringent use of irrigation via piston controlled syringe and limiting operation time to an hour.
My personal highlight was the presentation of videos by Mr René Sotelo on ‘getting out of sticky situations’ (SIU innovators symposium). An expert panel described similar mistakes to the ones shown on the videos and added what they would do if faced with the problem, leading to a fruitful and rich discussion. He showed tachycardia inducing, faint provoking videos of bleeding from upper and lower tract minimally invasive surgery. Advice such as stay calm, phone a friend, increase the pneumo, ‘suture fast’ was useful and practical. One case showed a rectal perforation at cystectomy where the attending/junior had been asked to place a swab (on stick) into the vagina, but it became apparent once the swab was on show and the vagina was intact that the swab had been misplaced into the rectum, thus highlighting the need to know your anatomy! An amazing image of a Ureteric stent that had been accidentally placed in the atrium was shown; but we were told the next step should not be to call an endourologist!
In the opening ceremony we were welcomed by Argentine tango dancers, the Minister of Health: a qualified doctor with degree in public health, and some Argentine hospitality of wine and typical foods. Friendly and collegiate atmosphere is what the Secretary of the SIU promised us, and friendly banter was present during the day. The first Brexit joke came when Mr Chris Parker started to explain to one presenter of the World Oncology federation why the UK was not included in the observation of deterioration of prostate cancer outcomes during the 2008 world recession, to which the presenter replied that it was only European countries in the paper. There was a mix of cheers and boos from the audience. However UK prostate cancer research, such as the PROMIS trial and the Emberton team studies were frequently quoted, as well as other British papers, with high esteem as corner stones of cancer research and advancing patient care.
Day 2 Friday
There was an early start for many who attended one of four optional instructional courses: each covered a different theme. I attended ‘management of priapism’ in view of its direct relevance to potential situations I may find myself in as an on call registrar. UCLH Consultants Asif Muneer and Guilio Garaffa hosted and gave clear information on acute management and surgical shunt techniques, plus imaging for more difficult cases, such as CT to exclude intra-abdominal cause of refractory priapism. The take home message was to consider early implantation of penile prosthesis if priapism lasts >72 hours. This was shown clearly on operative videos of prosthesis surgery at 3 weeks compared to 6 m; where the latter had penile fibrosis increasing surgical difficulty.
The first plenary session covered new advances in testicular cancer and another debate of focal therapy in intermediate prostate cancer. Scott Eggener presented a polished and compelling argument on why focal therapy could be the future, but Markus Graefen described his reluctance to accept it based on the research, limitations in MRI, and need for follow that is similar to active surveillance; but perhaps patient choice will drive us to make a conclusion. Fernando Secin described the low uptake of Active Surveillance within Argentina. This may be due to costs (both AS costs and costs lost by not operating) and lack of protocols; however, those clinicians who had undergone oncological training and worked in Academic centres were more likely to recommend AS.
Description of how Ebola affected our African colleagues and sadly mortality due to HSW highlights the breadth of education and world issues covered by the SIU congress. Winner of the SIU Astellas European Foundation Award, Dr John M Barry, described how five transplantation principles can be applied to urology. This included using life expectancy calculations, not age, in making decisions (he used his own Charlson comorbidity score to illustrate the point that it can be improperly used); he suggested using a quality of life grid and that practice guidelines, from numerous organisations use different grading systems thus he calls for unified, world scientific language.
I was invited to attend a ‘quick fire session for trainees’ where I met five experts and discussed career questions such as fellowships, choosing urology specialties and engaging with academia, which includes networking that we can practice during the conference. The experts were super friendly and one attendee was thrilled to meet Olivier Traxor who is his endourological hero.
Other sessions included the first session on ‘Professionalism in urology’ and included information on using Twitter and working with industry without compromising or influencing patient care by always practising evidence-based medicine. However, many researchers have ties to industry. Several tweets were shared during this session, for example:
Another session popular with trainees was ‘how to write a paper’ hosted by the World Journal of Urology.
Dan Wood from UCLH, UK chaired the session for congenital reconstruction, which included how to set up a service by Miss Claire Taylor; she emphasised the need to define the service you want to provide, decide which paediatric hospital you want to work with and having an excellent MDT and clinical specialist nurse, of which she is fortunate to have Winnie Nugent who works to bridge the gap between child and adult services.
The ‘Surgical Demo, session on Laparoscopy was well attended and the audience watched excellent videos from Karim Touijer on lap prostatectomy and Gonzalo Vitagliano on lap nephrectomy. The videos were clear and narration highlighted the relevant steps and anatomy. They emphasised the need to gain a mentor to reduce the learning curve and not attempt to set up a lap service solo. There was also an ‘encyclopaedic’ style Surgical Masters session of all types of prostate surgery for BPH that included surgical videos and tips/tricks.
Saturday
Many attended the sessions with a sore head on Saturday morning following the SIU Night party held at La Rural, a National Historic Landmark located in the Palermo district of Buenos Aires. It was inaugurated in the late 1800s in order to support and promote agricultural issues in Argentina. We were treated to typical foods: empanadas, freshly barbequed meats and sausages, breads and of course home grown wine. Entertainment was provided by Argentinian tango dancers and Argentine Gaucho dancers whose finale ended with Bolleadoras a dance that made hearts pound from the open male shirts, fast rhythm and the whirling ropes. Additionally, there was a photo booth for traditional Argentine dress, football snooker and a mechanical bull; luckily the only injury was an Australian trainee’s trousers.
The morning’s plenary session ‘Shifting sands – new technologies in stone disease’ covered a range of topics including retrograde intrarenal surgery by Mr Traxer. Mr Jorge Guitierrez highlighted the dangers of sepsis in stone disease; one key message included stopping stone surgery (including PCNL) when there was purulent urine. The panel agreed that 1-2cm stones fall in a grey area in the guidelines as to which treatment is the best. The majority of the panel favoured flexible ureteroscopy; but admitted that a patient’s ability to afford PCNL vs flexi URS and the surgeon’s skills and availability of equipment was what often governed practice rather than choice. Mariano Gonzalez described stone disease affecting pregnant women and the challenges of treating; interestingly he suggested that a low dose CT in the 2nd and 3rd trimester can be considered safe. Pradeep Rao informed us of the changing PCNL sizes and how the smaller ‘seeing needle scope’ at 4.8F enabled him to remove the stone in an infant less than one years old. Norberto Bernardo shared his experience with managing stones in complex patients, such as a case with severe scoliosis and another in a HSK. Mr Traxor made a plea that stents be used for the shortest time to reduce patient morbidity, i.e. as soon as they have been placed make a plan for ureteroscopy to enable stone treatment and removal.
The use of mesh for vaginal prolapse was debated by Nissrine Nakia (pro) and Paulo Palma (con). Palma highlighted the anatomy of the pelvic floor and the importance of identifying the level of deformity, which should then be used to select the right patients and select the correct procedure. The counter argument from Nakia started with a campaign slogan P.R.O.M.E.S.H in keeping with the ongoing US presidential debate. She stated that whilst the FDA did raise concerns regarding re-operation rates, there are now more modern meshes and are subjected to rigorous testing, plus experience has been gained regarding placement of mesh, post-mesh cystoscopy and use of oestrogen cream, which have all improved patient outcomes.
The European and Asian societies both presented in the plenary sessions. The EUA lecture, given by Arnulf Stenzl, described ongoing changes on how to improve TURBT, which included better training for juniors, including simulation, better visualisation (photo dynamic diagnosis) and the use of ‘bloc’ dissection with hybridknife to enable whole tumour removal in once piece, which can aid histological analysis.
Mr Foo from Singapore presented the UAA lecture on the subject of ‘holistic approach’ to care of BPH. Additionally that perhaps the Intro vesicular prostatic protrusion (IPP) tells us more about the likelihood of obstruction and when surgery would make the most difference.
Three parallel plenary sessions provided learning in the fields of spinal cord injury, paediatric urology and urological histology. The histology speakers had a tough job describing their field to us surgeons! The plenary session ‘SIU-ICD joint consultation on urological management of Spinal cord injury patients’ was well attended and covered the anatomy, surgical and non -surgical options, urodynamics and bladder emptying options. Speakers emphasised the need for Long-term follow-up, including upper tract imaging, blood tests (U&Es) and QOL questionnaires of which there are several. Each presenter clearly stated their recommendation and the level of evidence to support it. Tweets from this session included a commitment to reduce urine culture and treatment of UTI on asymptotic patients.
‘Ageing and urology’ session complemented the holistic theme as an expert panel discussed optimisation of elderly patients and the difficult decision making process of offering surgery in patients with frailty, high risk GA and delirium and co-morbidities. One panellist said it was about making a judgement that if the patient will appreciate the change and it will add to their QOL then age is not a barrier to operating; however, teamwork with anaesthetists and geriatrics is key to optimisation.
Each day a ‘Surgical Demo’ session’ ran, Saturday’s was on stones which was, like many stone sessions, full; Perhaps highlighting the enthusiasm towards Endourology. Pictured is Mr Guitierrez describing correct ureteroscopic hand manoeuvres and his ‘painting’ technique to dust stones. Additionally Mr Lojanapiwat from Thailand presented his operative experience in subcostal access for upper pole stones.
Throughout the afternoon were moderated poster sessions; from reducing laparoscopic camera fogging to comparison of traditional vs western medicine. These accepted abstracts were presented by urologists who were at varying stages of their careers. Presentations reflected high standards of research and a culmination of hard work. After watching some of the poster presentations I joined the urethral reconstruction ‘surgical tips’ session, which drew the biggest audience. The presentations offered high-quality operative pictures and complimentary radiology pictures showing the complexity of some of these strictures. Daniela Andrich from UCLH presented their experience of post-traumatic strictures and emphasised that the mechanism of injury correlates to the stricture pattern. Furthermore that partial ureteric injuries are probably under reported as they heal with the catheter in situ, sited by the trauma/orthopaedic team.
Sunday
The sun shone brightly on the last day of the conference and whilst many In the city were enjoying their Sunday lie in or preparing for church, conference delegates made their way to the last four early morning instructional courses. I attended ‘surviving prostate cancer’ chaired by Prof Mundy, which covered the aftermath of treatment for prostate cancer: fistulae, strictures, incontinence. Interestingly as our colleagues in General Surgery change techniques it provides new challenges relating to recto-vesical fistulae. It was recommended that MRIs should include sagittal views to best define the fistula anatomy. Prof Mundy described the difficulty that radiotherapy creates by scarring the tissues, which makes these patients more at risk of post-operative complications. This means it’s imperative to properly assess people prior to radiotherapy, including a cystoscopy to assess the bladder (and if applicable the post-prostatectomy anastomosis). Then consent the patient thoroughly prior to radiotherapy so that they’re aware of the more difficult surgery they face, should it be required.
The plenary session started with four speakers describing the emerging role of immunotherapy and specifically in cancers of the prostate, bladder and kidney. The research presented gave optimism of improving treatments for these cancers and that trials are ongoing and concluding. Fred Saad described how access to tissue can try to develop precision medicine; mutations specific to that tumour and patient could be assessed and tested in the laboratory so that treatment can be targeted and avoid treatments that don’t work.
A fierce debate regarding the role of varicocele surgery in the era of assisted reproduction ended in favour of offering surgery. Robert Brannigan presenting the ‘yes’ argument argued that varicocelectomy needs to be synergistic to assisted contraception, especially if time is of the essence in relation to maternal age. He gave evidence that varicocelectomy improves sperm quality for assisted conception and sees changes 3 months post-surgery. Alex Pastusak said he’d rather be ‘successful than lucky’ and was in favour of assisted contraception as the evidence for varicocelectomy, even the meta-analysis papers, has limitations so casts doubt on validity of available studies.
Rene Sotelo presented his endoscopic techniques for fistula repair, which included lap or robotic surgery within the bladder to remove the tract, create a plane between the bladder and surrounding tissues, place omentum or fascia between and then close the defect. We quickly moved from advanced techniques to trying to establish the basic technique with the next speaker. Alain Houlgate described his experience of establishing an endourological teaching programme between France and Senegal, which cumulates in a diploma.
Abstract prize winner Henry Woo presented his work on the International journal club #urojc where each month newly published articles are sent out to twitter followers and discussion generated. Unsurprisingly he was congratulated via twitter:
The last plenaries of the conference prior to further poster sessions included uroradiology, systemic cancer therapies and surgical demo on robotic cystectomy. The radiology session highlighted the advances in PSMA PET for prostate cancer recurrence but that TRUS still had a role.
River Plate Urological Meeting: representatives from the RSM – Urological section, UK, met with representatives from the Hospital Británicos in Rosario and Buenos Aires, Argentina and Montevideo, Uruguay. This is the first time these groups have met with the aim of collaboration and training. The day included presentations from the hospitals’ urology trainees, in English, on a range of topics and were marked as per the RSM marking criteria. The winning presentation was on ‘laparoscopic nephrectomy for living kidney donors’ and 2nd place for a presentation on ‘history of circumcision’. We had a tour of the hospital and were then welcomed into the British Embassy, to meet the Ambassador who is supportive of the relationships that are forming as a result of this meeting.
Concluding remarks
Overall the SIU was well organised, navigable and the incredible range of urology was well represented by experts in their field. The conference delegates were friendly, approachable and our host Buenos Aires warm and welcoming. Friendships and collaborations will undoubtedly continue beyond this congress.
The SIU Night was a particular highlight, showcasing the Argentine spirit in one evening for those who weren’t staying long in the country. The programme used varied formats and operative videos shown were generally of good quality. The presentations were of good calibre and the research presented both new and established. Reference was often made to EAU and AUA guidelines and international papers from a range of journals, in particular BJUI, Eur Urol and J Urol. The meeting of minds is certainly healthy to urological progress and exchanging ideas is key to innovation and improvement within our specialty across the world. There is so much we can learn from each other.
Adios SIU 2016! and ‘Até logo’ SIU 2017 Portugal!
Sophie Rintoul-Hoad is a urology trainee in the South Thames Deanery, currently working at King’s College hospital. She attended the SIU 2016 conference in Buenos Aires and then saw some of Argentina’s highlights, including a few days at El Venado Estancia playing polo and learning how to be a gaucho!
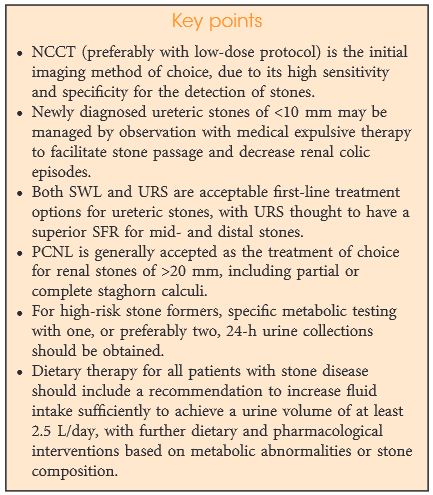
Several professional organizations have developed evidence-based guidelines for the initial evaluation, diagnostic imaging selection, symptomatic management, surgical treatment, medical therapy, and prevention of recurrence for both ureteric and renal stones. The purpose of this article is to summarize these guidelines with reference to the strength of evidence. All guidelines endorse an initial evaluation to exclude concomitant infection, imaging with a non-contrast computed tomography scan, and consideration of medical expulsive therapy or surgical intervention depending on stone size and location. Recommends for metabolic evaluation vary by guideline, but all endorse increasing fluid intake to reduce the risk of recurrence.