What’s the Diagnosis?
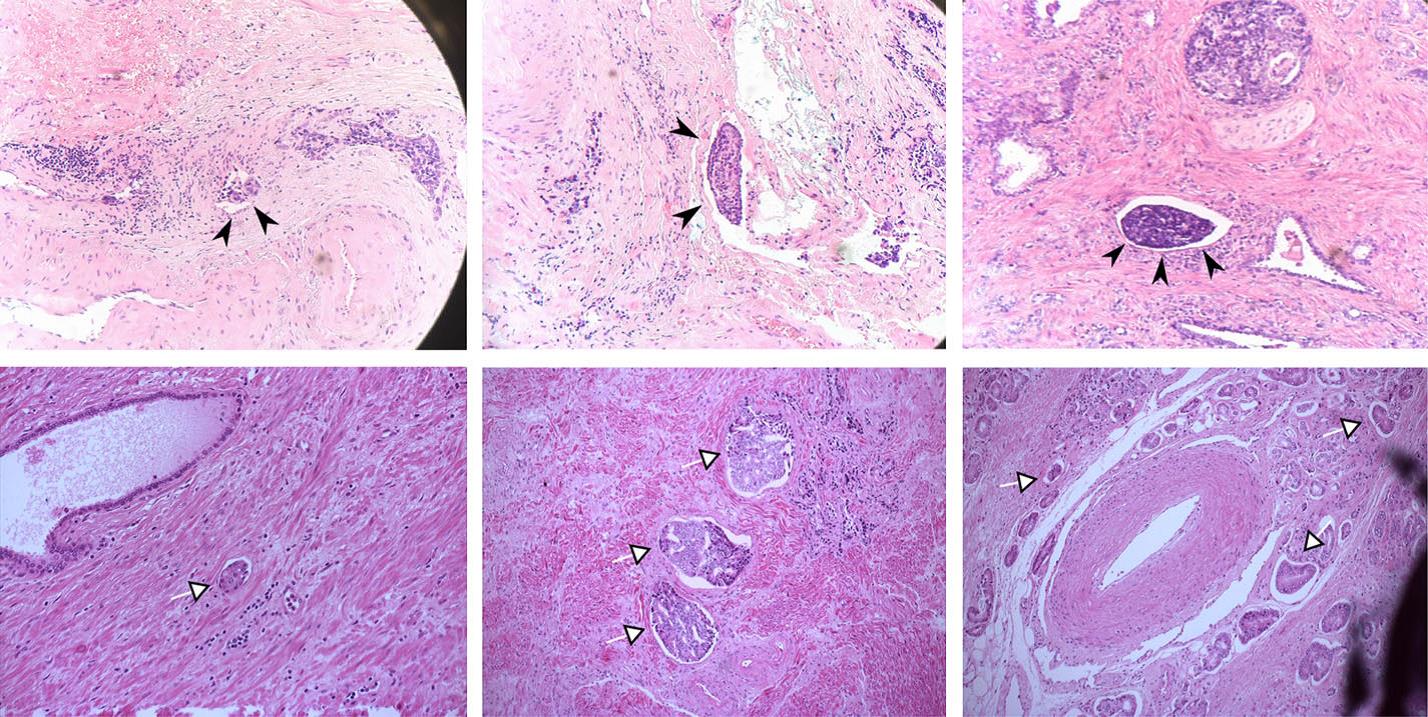
Images taken from Galiabovitch et al (BJUI, 2017). These show H&E staining pathological specimens after radical prostatectomy.
No such quiz/survey/poll
Images taken from Galiabovitch et al (BJUI, 2017). These show H&E staining pathological specimens after radical prostatectomy.
No such quiz/survey/pollIt’s hard to believe that we have been doing the BJUI Social Media Awards for five years now! I recall vividly our inaugural BJUI Social Media Awards in 2013, as the burgeoning social media community in urology gathered in the back of an Irish Bar in San Diego to celebrate all things social. At that time, many of us had only got to know each other through Twitter, and it was certainly fun going around the room putting faces with twitter handles for the first time. That spirit continues today as the “uro-twitterati” continues to grow, and the BJUI Awards, (or the “Cult” Awards as our Editor-in-Chief likes to call them), remains a fun annual focus for the social-active urology community to meet up in person.
As you may know, we alternate the Awards between the annual congresses of the American Urological Association (AUA) and of the European Association of Urology (EAU). Last year, we descended on Munich, Germany to join the 13,000 or so other delegates attending the EAU Annual Meeting and to enjoy all the wonderful Bavarian hospitality on offer. This year, we set sail for the #AUA17 Annual Congress in Boston, MA, along with over 16,000 delegates from 100 different countries. What a great few days in beautiful Boston and a most welcome return for the AUA to this historic city. Hopefully it will have a regular spot on the calendar, especially with the welcome dumping of Anaheim and Orlando as venues for the Annual Meeting.
On therefore to the Awards. These took place on Saturday 13th May 2017 in the City Bar of the Westin Waterfront Boston. Over 80 of the most prominent uro-twitterati from all over the world turned up to enjoy the hospitality of the BJUI and to hear who would be recognised in the 2017 BJUI Social Media Awards. We actually had to shut the doors when we reached capacity so apologies to those who couldn’t get in! Individuals and organisations were recognised across 12 categories including the top gong, The BJUI Social Media Award 2017, awarded to an individual, organization, innovation or initiative who has made an outstanding contribution to social media in urology in the preceding year. The 2013 Award was won by the outstanding Urology Match portal, followed in 2014 by Dr Stacy Loeb for her outstanding individual contributions, and in 2015 by the #UroJC twitter-based journal club. Last year’s award went to the #ilooklikeaurologist social media campaign which we continue to promote.
This year our Awards Committee consisted of members of the BJUI Editorial Board – Declan Murphy, Prokar Dasgupta, Matt Bultitude, Stacy Loeb, John Davis, as well as BJUI Managing Editor Scott Millar whose team in London (Max and Clare) drive the content across our social platforms. The Committee reviewed a huge range of materials and activity before reaching their final conclusions.
The full list of winners is as follows:
Most Read Blog@BJUI – “The optimal treatment of patients with localized prostate cancer: the debate rages on”. Dr Chris Wallis, Toronto, Canada
Most Commented Blog@BJUI – “It’s not about the machine, stupid”. Dr Declan Murphy, Melbourne, Australia
Most Social Paper – “Novel use of Twitter to disseminate and evaluate adherence to clinical guidelines by the European Association of Urology”. Accepted by Stacy Loeb on behalf of herself and her colleagues.
Best BJUI Tube Video – “Combined mpMRI Fusion and Systematic Biopsies Predict the Final Tumour Grading after Radical Prostatectomy”. Dr Angela Borkowetz, Dresden, Germany
Best Urology Conference for Social Media – #USANZ17 – The Annual Scientific Meeting of the Urological Association of Australia & New Zealand (USANZ) 2017. Accepted by Dr Peter Heathcote, Brisbane, Australia. President of USANZ.
Best Urology App – The EAU Guidelines App. Accepted by Dr Maria Ribal, Barcelona, Spain, on behalf of the EAU.
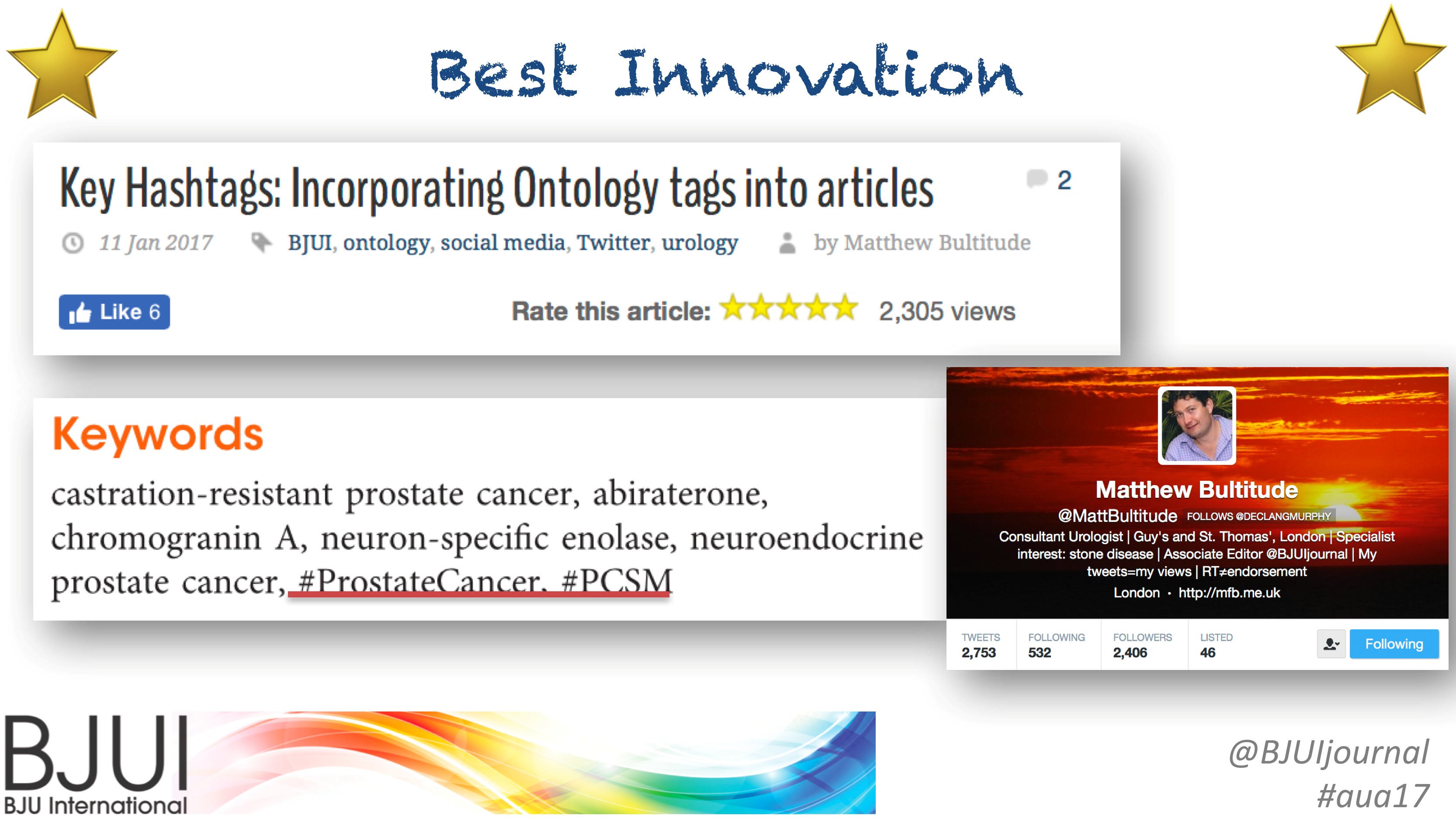
Innovation Award – BJUI Urology Ontology Hashtags keywords. Accepted by Dr Matthew Bultitude, London, UK, on behalf of the BJUI.
#UroJC Award – Dr Brian Stork, Michigan, USA. Accepted by Dr Henry Woo of Brian’s behalf.
Most Social Trainee – Dr Chris Wallis, Toronto, Canada
Best Urology Journal for Social Media –Journal of Urology/Urology Practice. Accepted by Dr Angie Smith, Chapel Hill, USA, on behalf of the AUA Publications Committee.
Best Urology Organisation – Canadian Urological Association. Accepted by Dr Mike Leveridge, Vice-President of Communications for CUA.
The BJUI Social Media Award 2017 – The Urology Green List, accepted by Dr Henry Woo, Sydney, Australia.
All the Award winners (except Dr Brian Stork who had to get home to work), were present to collect their awards themselves. A wonderful spread of socially-active urology folk from all over the world, pictured here with BJUI Editor-in-Chief, Prokar Dasgupta.
A special thanks to our outstanding BJUI team at BJUI in London, Scott Millar, Max Cobb and Clare Dunne, who manage our social media and website activity as well as the day-to-day running of our busy journal.
See you all in Copenhagen for #EUA18 where we will present the 6th BJUI Social Media Awards ceremony!
Declan Murphy
Peter MacCallum Cancer Centre, Melbourne, Australia
Associate Editor, BJUI
@declangmurphy
TRoMbone is launched! The UK feasibility randomised trial Testing radical prostatectomy in men with prostate cancer and oligoMetastases to the bone has opened at Oxford University Hospitals (PI Freddie Hamdy), University College London Hospitals (PI John Kelly) and Royal Surrey County Hospital (PI Chris Eden). Men <75 with newly-diagnosed prostate cancer and 1-3 skeletal lesions on any standard-of-care imaging (CT, bone scan, MRI, or PET) who are fit for surgery and deemed to be technically operable are eligible. Emerging but lower-quality data suggests a role for treatment of the primary tumour in men with oligo-metastatic prostate cancer and this UK study will investigate this question with level 1 evidence.
Participants will be randomly allocated to standard-of-care treatment (hormones +/- chemotherapy) versus standard-of-care treatment plus surgery to remove the prostate and draining lymph nodes (radical prostatectomy plus extended pelvic lymphadenectomy). A qualitative recruitment investigation to optimise accrual will be conducted by the University of Bristol (Caroline Wilson) and biologic samples will be collected, processed and stored in a repository at the Institute of Cancer Research (Gerhardt Attard).
We will assess technical feasibility, safety and complications of surgery in oligo-metastatic prostate cancer, and examine ways to improve recruitment in this pilot study. TRoMbone is managed by the Surgical Intervention Trials Unit at the University of Oxford and funded by the Prostate Cancer Foundation and The Urology Foundation.
We need to recruit 50 men over a 12-month period, and are seeking referrals from other centres to increase accrual. Centres that demonstrate ability to refer eligible patients will be able to take part in the main trial if we can demonstrate feasibility in this phase and get funding for the larger study.
So please look out for these patients and send them to me at UCLH, Freddie in Oxford, or Chris in Guildford. One of the three of us will do the surgery if they get randomised to it, but of course you’re welcome to come with the patients. If you have any queries please contact me, the study CI (P. Sooriakumaran (PS); prasanna.sooriakumaran@nds.ox.ac.uk) or the study co-ordinator (Neelam Hassanali; trombone@nds.ox.ac.uk). You can start them on androgen deprivation and ‘stop the clock’ before you refer them to us. The extra burden of participating in this study is minimal. They will require one visit for consent, and one follow-up visit at 3 months after randomisation. The surgical group will also have two other visits for their surgery and catheter removal. The rest of the follow-up can be done back at your referring centre or with us, whatever you and the patient prefer. If it’s your standard policy to give them chemotherapy or metastasis-directed therapy with SBRT then you can still do that as part of the study.
With your help we can demonstrate that this study is feasible in the UK and we can lead the way in the surgical management of oligo-metastatic prostate cancer.
P. Sooriakumaran [social type=”facebook” opacity=”dark’ label=’PLACE_LINK_HERE[/social]
BMedSci(Hons) BMBS(Hons) PhD PGCMedLaw ADCClinInv FRCS(Urol) FEBU USLME
Consultant Urological Surgeon, UCL Hospitals NHS Foundation Trust & Honorary Clinical Senior Researcher, University of Oxford
The twitter-based international urology journal club @iurojc #urojc is back with a splash after a brief hiatus. For the March 2017 #urojc, a lively discussion takes the theme of pelvic node dissection (PLND) on radical prostatectomy (RP) reviewing a timely article by Nicola Fossati et al. The paper was made available open access courtesy of European Urology @EUplatinum.
Benefits and Harms of Different Extents of LND During Radical Prostatectomy for #ProstateCancer: A https://t.co/PxRbbUyQOM
— European Urology (@EUplatinum) February 13, 2017
A systematic review of the literature was performed including all comparative studies of both randomized and non randomized studies, with at least one experimental and one control arm. This summarised 66 studies including more than 250.000 patients with particular focus on different extents of pelvic lymphadenectomy as proposed by the European Association of Urology. Outcome measures studied included oncological features of biochemical recurrence, development of metastases, cancer-specific survival, and overall survival. Adverse events were covered under secondary outcomes, both intra- and postoperatively observed. Finally, quality of PLND was addressed in terms of total number of nodes and total number of positive nodes. Risk of bias was assessed for all studies judging on basis of specific confounders.
The journal club ran for 48 hours from Sunday 5th march. The central question addressed is balance of benefits and drawbacks of lymph node dissection. The corresponding author of the manuscript, Steven Joniau from the University Hospitals of Leuven, Belgium highlighted the role of lymph nodes in prostate cancer recurrence.
#urojc Remember: PCa recurrence often first in regional LN. So, why not remove at RP? @iurojc @ChapinMD @LoebStacy @EveraertsW @dr_coops pic.twitter.com/5GRKhjOJfl
— steven joniau (@joniau) March 6, 2017
However despite this idea, the benefit of PLND is heavily scrutinized from the start. Long term data from a single centre suggested limited benefit.
How do we reconcile what appears to be lack of therapeutic benefit & morbidity for ePLND and current guidelines? #urojc
— Urology JC #urojc (@iurojc) March 5, 2017
Depends on how much time you spend on it
JH population was "unique". Therapeutic benefit depends on the cohort being studied.
— Badar M. Mian, MD (@BadarMian1) March 5, 2017
If PSA bcf so high with N1 disease, has PLND really made a diff? How is management changed if N1 disease confirmed pathologically? #urojc
— Urology JC #urojc (@iurojc) March 6, 2017
However PLND has since earlier times been employed as a diagnostic tool, where an optimal template (presacral in addition to extended LND) may be optimal for staging and removal of lymph nodes.
Does need for accurate staging trump (NOT about that man
) therapeutic benefit for standard PLND versus ePLND?#urojc pic.twitter.com/6N3bjAoRS2
— Urology JC #urojc (@iurojc) March 5, 2017
Try to encourage in our MDT as node info is often can often fine tune further management after RP #urojc https://t.co/4fZQ2eEVkv
— Nick Brook (@nickbrookMD) March 5, 2017
#urojc But knowlegde gained by PLND may guide decisions regarding adj treatment (which may influence survival)
— steven joniau (@joniau) March 6, 2017
Prospective study shows 'less-than-eLND' insuficient for staging. eLND 94% accurate staging, but misses 24% pos LN compared to seLND pic.twitter.com/f1Fm26SPcp
— steven joniau (@joniau) March 6, 2017
Despite the current state of evidence, PLND is frequently mentioned in the various guidelines available for prostate cancer. However the exact situations when to employ them is questioned by some participants.
How do we reconcile what appears to be lack of therapeutic benefit & morbidity for ePLND and current guidelines? #urojc
— Urology JC #urojc (@iurojc) March 5, 2017
@iurojc @nickbrookMD #EAUGuidelines mention Briganti, MSKCC or Roach nomograms, NCCN doesn't recommend a particular nomogram #urojc pic.twitter.com/QAdE4PBsHa
— Stacy Loeb, MD (@LoebStacy) March 6, 2017
#urojc @joniau @ChapinMD @LoebStacy @dr_coops Makes sense for high risk tumours, but the EAU 5% guideline for PLND is overkill
— Wouter Everaerts (@EveraertsW) March 6, 2017
The various therapeutic options for lymph node metastases also coloured the discussion.
if we can figure out whether postop RT necessary in all N1, ePLND may help avoid unnecessary treatment in some. #urojc
— Brian F. Chapin (@ChapinMD) March 6, 2017
The discussion further continued to the important issue of morbidity, and the associated question of performing an extended PLND (ePLND).
Are we understating morbidity of ePLND? Do we leave these patient on a knifes edge for future lymphodema? (Eg future RT, infection)#urojc
— Urology JC #urojc (@iurojc) March 6, 2017
@joniau lymphoedema is major concern for QoL, especially after eLND+ adj RT,
Needs multiD management #urojc— Wouter Everaerts (@EveraertsW) March 6, 2017
the baby shouldn't be in the bath. PLND so clearly needs to be tested in a prospective trial. As for ePLND…
— Tim O'Brien (@tsoburol) March 6, 2017
What's your justification for doing an ePLND? Is it because of guideline recommendations?#urojc
— Urology JC #urojc (@iurojc) March 5, 2017
#urojc ePLND = mmmPLND, more morbidity,minutes,money. less BCR, doubt it.
— Alan Hay (@alanhaymd) March 5, 2017
@iurojc ePLND does nearly double my time for RALRP. Sometimes even longer then the prostatectomy. #urojc
— Brian F. Chapin (@ChapinMD) March 6, 2017
.@DrHWoo I don't follow–Some N+ men essntlly cured by only RP/PLND. I think it's therapeutic.
But I don't believe ePLND= improvemnt #urojc pic.twitter.com/EwSp4Im5VO— David Y.T. Chen (@dytcmd) March 6, 2017
Try to encourage in our MDT as node info is often can often fine tune further management after RP #urojc https://t.co/4fZQ2eEVkv
— Nick Brook (@nickbrookMD) March 5, 2017
#urojc But knowlegde gained by PLND may guide decisions regarding adj treatment (which may influence survival)
— steven joniau (@joniau) March 6, 2017
Prospective study shows 'less-than-eLND' insuficient for staging. eLND 94% accurate staging, but misses 24% pos LN compared to seLND pic.twitter.com/f1Fm26SPcp
— steven joniau (@joniau) March 6, 2017
Despite the current state of evidence, PLND is frequently mentioned in the various guidelines available for prostate cancer. However the exact situations when to employ them is questioned by some participants.
How do we reconcile what appears to be lack of therapeutic benefit & morbidity for ePLND and current guidelines? #urojc
— Urology JC #urojc (@iurojc) March 5, 2017
@iurojc NCCN guidelines recommend PLND for nomogram probability >=2% vs 5% threshold in #eauguidelines #urojc pic.twitter.com/7HYVSYUSJv
— Stacy Loeb, MD (@LoebStacy) March 6, 2017
@iurojc @nickbrookMD #EAUGuidelines mention Briganti, MSKCC or Roach nomograms, NCCN doesn't recommend a particular nomogram #urojc pic.twitter.com/QAdE4PBsHa
— Stacy Loeb, MD (@LoebStacy) March 6, 2017
#urojc @joniau @ChapinMD @LoebStacy @dr_coops Makes sense for high risk tumours, but the EAU 5% guideline for PLND is overkill
— Wouter Everaerts (@EveraertsW) March 6, 2017
The
if we can figure out whether postop RT necessary in all N1, ePLND may help avoid unnecessary treatment in some. #urojc
— Brian F. Chapin (@ChapinMD) March 6, 2017
The discussion further continued to the important issue of morbidity, and the associated question of performing an extended PLND (ePLND).
Are we understating morbidity of ePLND? Do we leave these patient on a knifes edge for future lymphodema? (Eg future RT, infection)#urojc
— Urology JC #urojc (@iurojc) March 6, 2017
@joniau lymphoedema is major concern for QoL, especially after eLND+ adj RT,
Needs multiD management #urojc— Wouter Everaerts (@EveraertsW) March 6, 2017
the baby shouldn't be in the bath. PLND so clearly needs to be tested in a prospective trial. As for ePLND…
— Tim O'Brien (@tsoburol) March 6, 2017
What's your justification for doing an ePLND? Is it because of guideline recommendations?#urojc
— Urology JC #urojc (@iurojc) March 5, 2017
#urojc ePLND = mmmPLND, more morbidity,minutes,money. less BCR, doubt it.
— Alan Hay (@alanhaymd) March 5, 2017
@iurojc ePLND does nearly double my time for RALRP. Sometimes even longer then the prostatectomy. #urojc
— Brian F. Chapin (@ChapinMD) March 6, 2017
.@DrHWoo I don't follow–Some N+ men essntlly cured by only RP/PLND. I think it's therapeutic.
But I don't believe ePLND= improvemnt #urojc pic.twitter.com/EwSp4Im5VO— David Y.T. Chen (@dytcmd) March 6, 2017
if we can figure out whether postop RT necessary in all N1, ePLND may help avoid unnecessary treatment in some. #urojc
— Brian F. Chapin (@ChapinMD) March 6, 2017
The increasing use of PSMA PET/CT provided other spread pattern data to be considered. And finally temporal changes in PSA testing is observed to affect the need for LND.
How might Ga68 PSMA PET/CT change the dynamic? Early data shows a lot of disease above the diaphragm. #urojc https://t.co/zyX9czHuwH
— Urology JC #urojc (@iurojc) March 6, 2017
Although, with PSMA PET/CT we're finding crazy spread patterns (e.g. Isolated supraclav nodal met) #urojc
— Matt Cooperberg (@dr_coops) March 6, 2017
I dunno… in 2017 I think it's a very rare pt who needs the RP and doesn't need the LND! #urojc @iurojc
— Matt Cooperberg (@dr_coops) March 6, 2017
#urojc @dr_coops @LoebStacy @iurojc the pt who "doesn't need PLND" probably often doesn't need RP either. Especially in PSA era
— David Y.T. Chen (@dytcmd) March 6, 2017
From the poll which ran during the discussion, about half responders would perform extended PLND for staging, while the rest were divided almost equally between therapeutic benefit and adherence to guideline recommendations.
Why do you do ePLND?#urojc
— Urology JC #urojc (@iurojc) March 5, 2017
Probably all participants of the discussion agrees for the need of a proper randomised study addressing role of PLND.
But "therapeutic benefits of PLND during radical prostatectomy remain unproven"@ChapinMD @LoebStacy @EveraertsW @dr_coops#urojc
— Henry Woo (@DrHWoo) March 6, 2017
At the end of a busy 48 hours, the discussion had been joined by top experts in the field of prostate cancer, generated more than 200 tweets and reached more than 700 thousand impressions the world over.
Special thanks to @EUplatinum for allowing open access for this month's paper. Special thanks to author @joniau for participating #urojc
— Urology JC #urojc (@iurojc) March 7, 2017
Yodi Soebadi (@yodisoebadi) is an Indonesian urologist, trained at Universitas Airlangga, currently pursuing doctoral research at KU Leuven in Belgium.
Every Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video from Dr. Francesco Alessandro Mistretta, discussing his paper.
If you only have time to read one article this week, it should be this one.
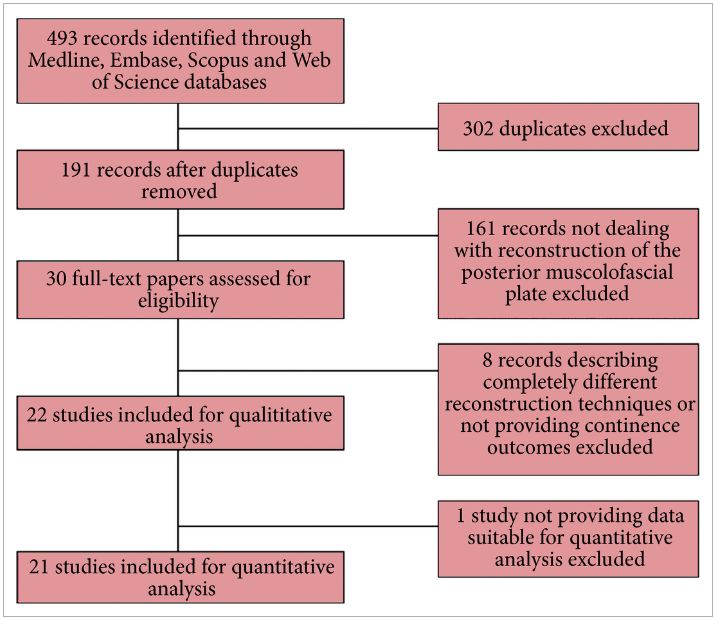
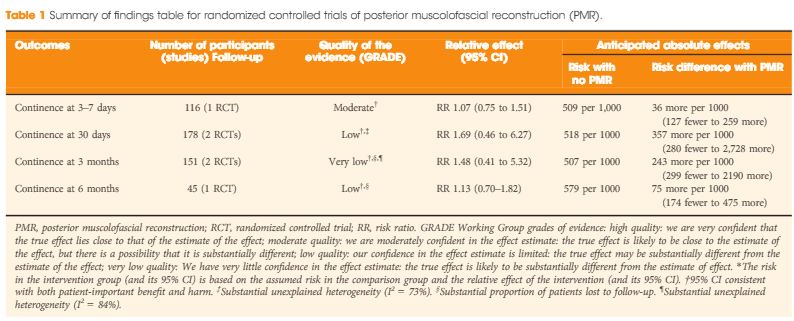
In their systematic review and meta-analysis, Grasso et al. [1] address the question of whether posterior muscolofascial reconstruction (PMR), the so-called Rocco stitch, positively affects urinary continence after radical prostatectomy. The relevance of the question to this structured form of inquiry is that individual studies to date have been inconclusive. We recognize Sir Archie Cochrane, who gave his name to the Cochrane Collaboration that pioneered the methods for conducting systematic reviews, for emphasizing the critical importance of looking at the entire body of evidence in a structured manner when seeking to answer a clinical question [2]. In the present study, which included both randomized controlled trials (RCTs) and observational studies of variable methodological quality, a favourable impact of PMR across all postoperative time points (3–7 days, 30 days, 3 and 6 months) was observed. The effect was most pronounced early on at the time of catheter removal, when the patients undergoing PMR were nearly twice as likely as the control group (risk ratio 1.9; 95% CI 1.3–2.9) to be continent, thereby suggesting a major benefit of this approach. It should be noted, however, that this analysis was dominated by the observational studies, particularly retrospective observational studies, which offer the least degree of methodological rigor.
Even more important, therefore, than the act of pooling across studies is the rating of the quality of evidence for the body of evidence on an outcome-specific basis. Based on the GRADE approach, which has become the most widely endorsed framework for rating the quality of evidence, we would initially place a high and low level of confidence in a body of evidence drawn from RCTs and observational studies, respectively [3]. As a result, one might plan a separate analysis of those two groups of studies first, and only move to pool them if their results were similar. In this case, the results from the RCTs and observational studies were different, with prospective and retrospective studies reporting larger, probably exaggerated effect sizes; however, it is also understood that other aspects such as study limitation (risk of bias), inconsistency, impression, indirectness and risk publication bias may lower our confidence in the effect estimates from RCTs [4]. Focusing on the body of evidence from RCTs alone (Table 1) we have ‘moderate’ confidence that PMR may not improve early continence at the time of catheter removal. Similarly, the few RCTs that contributed to the assessment of continence at later timepoints do not provide evidence that continence is affected favourably, although our confidence for those outcomes is only ‘low’ or ‘very low’, suggesting that future trials may change these estimates of effect. Meanwhile, it should be noted that none of the RCTs appeared to provide information on the potential downsides of PMR, such as rates of urinary retention or bladder neck contracture. As a result, enough uncertainty remains to state that the jury on PMR is still out; this is consistent with the authors’ call for a future high-quality trial, which is reportedly ongoing. While PMR is already widely used by open and robot-assisted prostatectomy surgeons around the globe, this example sheds light on current evidentiary standards of surgical innovation. Following the IDEAL recommendations, it would be much preferred if the urological community committed to well designed trials for novel surgical approaches and device-dependent interventions up front, before moving to widespread dissemination [5].
Every Month the Editor-in-Chief selects an Article of the Month from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video from Klaus Brasso, discussing his paper.
If you only have time to read one article this week, it should be this one.
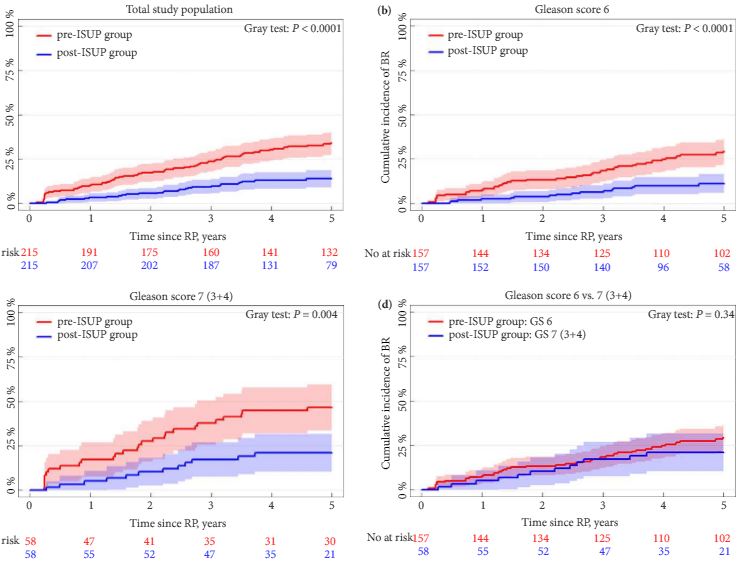
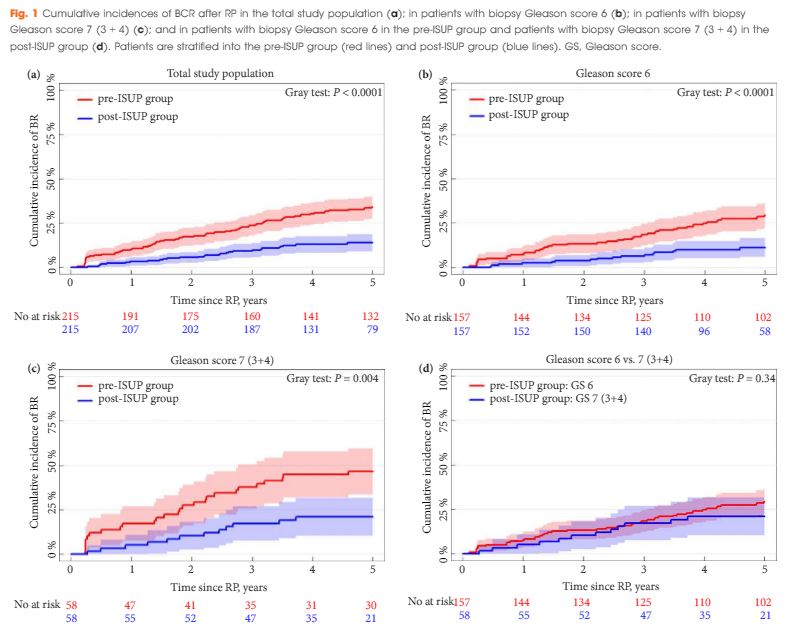
To investigate whether the International Society of Urological Pathology (ISUP) 2005 revision of the Gleason grading system has influenced the risk of biochemical recurrence (BCR) after radical prostatectomy (RP), as the new guideline implies that some prostate cancers previously graded as Gleason score 6 (3 + 3) are now considered as 7 (3 + 4).
A matched-pair analysis was conducted. In all, 215 patients with Gleason score 6 or 7 (3 + 4) prostate cancer on biopsy who underwent RP before 31 December 2005 (pre-ISUP group), were matched 1:1 by biopsy Gleason score, clinical tumour category, PSA level, and margin status to patients undergoing RP between 1 January 2008 and 31 December 2011 (post-ISUP group). Patients were followed until BCR defined as a PSA level of ≥0.2 ng/mL. Risk of BCR was analysed in a competing-risk model.
The median follow-up was 9.5 years in the pre-ISUP group and 4.8 years in the post-ISUP group. The 5-year cumulative incidences of BCR were 34.0% and 13.9% in the pre-ISUP and post-ISUP groups, respectively (P < 0.001). The difference in cumulative incidence applied to both patients with Gleason score 6 (P < 0.001) and 7 (3 + 4) (P = 0.004). There was no difference in the 5-year cumulative incidence of BCR between patients with pre-ISUP Gleason score 6 and post-ISUP Gleason score 7 (3 + 4) (P = 0.34). In a multiple Cox-proportional hazard regression model, ISUP 2005 grading was a strong prognostic factor for BCR within 5 years of RP (hazard ratio 0.34; 95% confidence interval 0.22–0.54; P < 0.001).
The revision of the Gleason grading system has reduced the risk of BCR after RP in patients with biopsy Gleason score 6 and 7 (3 + 4). This may have consequences when comparing outcomes across studies and historical periods and may affect future treatment recommendations.
Berg et al. [1] report that patients classified as Gleason score 7 (3 + 4) according to the revised grading system published in 2005 are to some extent similar to patients with pre-2005 Gleason score 6, at least in terms of risk of biochemical recurrence. The logical but not necessarily correct conclusion is that current patients with Gleason score 7 on biopsy are appropriate candidates for active surveillance.
What must be kept in mind is that, using the post-2005 revised grading system, approximately 25% of men with Gleason score 3 + 4 = 7 on biopsy have either 3 + 4 = 7 with tertiary pattern 5 or >4 + 3 = 7 in the corresponding radical prostatectomy [1]. With the exception of men with a limited life expectancy, these men need definitive therapy for their potentially life-threatening cancer. Numerous studies have shown that extended biopsies, whether they are >10- or 12-core, are associated with less upgrading than sextant biopsies [2]. In the report by Berg et al. [1], the median number of cores sampled before 2005 was 6 with an interquartile range (IQR) of 6–6 compared with a median (IQR) of 10 (10–12) cores after 2005. Consequently, in their cohorts, the pre-2005 group of men with Gleason score 3 + 3 = 6 were more likely to have unsampled higher grade cancer and a correspondingly worse prognosis more closely approximating post-2005 better-sampled Gleason score 3 + 4 = 7 cancers.
Berg et al. [1] further claim that the prognostic and clinical value of Gleason score 7 has been weakened since the 2005 modifications. In fact, the revised grading system more accurately reflects prostate cancer biology than the pre-2005 Gleason system. The major consequence of the modification, as Berg et al. [3] illustrate, has been the better prognosis associated with post-2005 Gleason score 6 cancer because patterns associated with more aggressive behaviour have been shifted to Gleason score 7. Historically, a diagnosis of Gleason score 6 cancer, even at radical prostatectomy, was not as predictive of ‘good’ behaviour, and had a higher rate of progression with some men even dying from prostate cancer [4]. Currently, Gleason score 6 cancer at radical prostatectomy has a 96% cure rate at 5 years, even including cases with extraprostatic extension and positive margins [3]. Several studies have shown that post-2005 pure Gleason score 6 cancers at radical prostatectomy are incapable of metastasizing to lymph nodes [4]. Berg et al. are correct, however, that men with a post-2005 grade of Gleason Score 3 + 4 = 7 have a better prognosis than those graded prior to 2005. As a consequence, it has been recommended that pathologists should record the percent pattern 4 in cases with Gleason score 7 on biopsy for men being considered for active surveillance [5]. For the appropriate patient, depending on age, comorbidity, extent of cancer, MRI findings, patient desire, etc., could be a candidate for active surveillance with Gleason score 3 + 4 = 7 if the pattern 4 is limited. Currently, this information is not transparent in most pathology reports.
A new grading system, first proposed in BJUI by this author, and verified in a large multi-institutional study, resulted in a simplified five-grade group system that more accurately reflects the biology of prostate cancer than the pre-2005 grading system [3, 6]. Men with Gleason score 6 cancers need to be reassured that their cancer is the lowest grade that is currently assigned, despite Gleason scores ranging from 2 to 10. In addition, I have talked to some patients with Gleason score 3 + 4 = 7 who think that they are going to die in the near future because their score of 7 was closer to highest grade of 10 than the lowest grade of 2. With the new grading system, patients can be reassured that they have a Grade group 1 (3 + 3 = 6) out of 5, which is the lowest grade, or a Grade group 2 (Gleason score 3 + 4 = 7) out of 5, which is still a relatively low grade.
To investigate whether the International Society of Urological Pathology (ISUP) 2005 revision of the Gleason grading system has influenced the risk of biochemical recurrence (BCR) after radical prostatectomy (RP), as the new guideline implies that some prostate cancers previously graded as Gleason score 6 (3 + 3) are now considered as 7 (3 + 4).
A matched-pair analysis was conducted. In all, 215 patients with Gleason score 6 or 7 (3 + 4) prostate cancer on biopsy who underwent RP before 31 December 2005 (pre-ISUP group), were matched 1:1 by biopsy Gleason score, clinical tumour category, PSA level, and margin status to patients undergoing RP between 1 January 2008 and 31 December 2011 (post-ISUP group). Patients were followed until BCR defined as a PSA level of ≥0.2 ng/mL. Risk of BCR was analysed in a competing-risk model.
The median follow-up was 9.5 years in the pre-ISUP group and 4.8 years in the post-ISUP group. The 5-year cumulative incidences of BCR were 34.0% and 13.9% in the pre-ISUP and post-ISUP groups, respectively (P < 0.001). The difference in cumulative incidence applied to both patients with Gleason score 6 (P < 0.001) and 7 (3 + 4) (P = 0.004). There was no difference in the 5-year cumulative incidence of BCR between patients with pre-ISUP Gleason score 6 and post-ISUP Gleason score 7 (3 + 4) (P = 0.34). In a multiple Cox-proportional hazard regression model, ISUP 2005 grading was a strong prognostic factor for BCR within 5 years of RP (hazard ratio 0.34; 95% confidence interval 0.22–0.54; P < 0.001).
The revision of the Gleason grading system has reduced the risk of BCR after RP in patients with biopsy Gleason score 6 and 7 (3 + 4). This may have consequences when comparing outcomes across studies and historical periods and may affect future treatment recommendations.