
Posts
Article of the Week: NICE Guidance ‐ Complicated UTIs: ceftolozane/tazobactam
Every Week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
If you only have time to read one article this week, it should be this one.
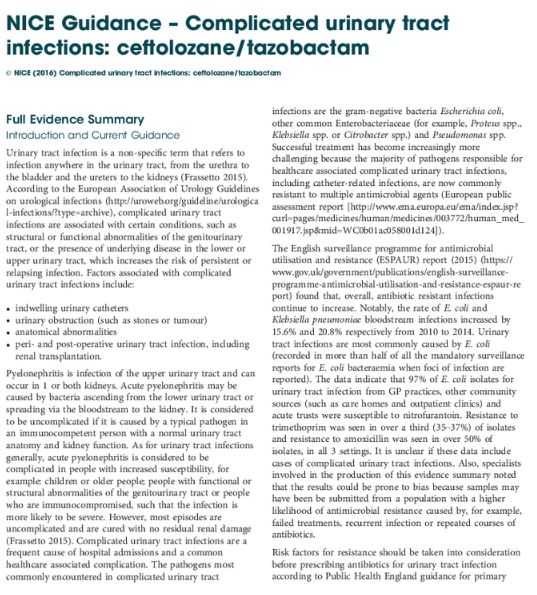
NICE Guidance ‐ Complicated urinary tract infections: ceftolozane/tazobactam
Introduction and Current Guidance
Urinary tract infection is a non‐specific term that refers to infection anywhere in the urinary tract, from the urethra to the bladder and the ureters to the kidneys. According to the European Association of Urology Guidelines on urological infections (https://uroweb.org/guideline/urological-infections/?type=archive), complicated urinary tract infections are associated with certain conditions, such as structural or functional abnormalities of the genitourinary tract, or the presence of underlying disease in the lower or upper urinary tract, which increases the risk of persistent or relapsing infection. Factors associated with complicated urinary tract infections include:
- indwelling urinary catheters
- urinary obstruction (such as stones or tumour)
- anatomical abnormalities
- peri‐ and post‐operative urinary tract infection, including renal transplantation.
Pyelonephritis is infection of the upper urinary tract and can occur in 1 or both kidneys. Acute pyelonephritis may be caused by bacteria ascending from the lower urinary tract or spreading via the bloodstream to the kidney. It is considered to be uncomplicated if it is caused by a typical pathogen in an immunocompetent person with a normal urinary tract anatomy and kidney function. As for urinary tract infections generally, acute pyelonephritis is considered to be complicated in people with increased susceptibility, for example: children or older people; people with functional or structural abnormalities of the genitourinary tract or people who are immunocompromised, such that the infection is more likely to be severe. However, most episodes are uncomplicated and are cured with no residual renal damage. Complicated urinary tract infections are a frequent cause of hospital admissions and a common healthcare associated complication. The pathogens most commonly encountered in complicated urinary tract infections are the gram‐negative bacteria Escherichia coli, other common Enterobacteriaceae (for example, Proteus spp., Klebsiella spp. or Citrobacter spp.) and Pseudomonas spp. Successful treatment has become increasingly more challenging because the majority of pathogens responsible for healthcare associated complicated urinary tract infections, including catheter‐related infections, are now commonly resistant to multiple antimicrobial agents (European public assessment report [https://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/003772/human_med_001917.jsp&mid=WC0b01ac058001d124]).
The English surveillance programme for antimicrobial utilisation and resistance (ESPAUR) report (2015) (https://www.gov.uk/government/publications/english-surveillance-programme-antimicrobial-utilisation-and-resistance-espaur-report) found that, overall, antibiotic resistant infections continue to increase. Notably, the rate of E. coli and Klebsiella pneumoniae bloodstream infections increased by 15.6% and 20.8% respectively from 2010 to 2014. Urinary tract infections are most commonly caused by E. coli (recorded in more than half of all the mandatory surveillance reports for E. coli bacteraemia when foci of infection are reported). The data indicate that 97% of E. coli isolates for urinary tract infection from GP practices, other community sources (such as care homes and outpatient clinics) and acute trusts were susceptible to nitrofurantoin. Resistance to trimethoprim was seen in over a third (35–37%) of isolates and resistance to amoxicillin was seen in over 50% of isolates, in all 3 settings. It is unclear if these data include cases of complicated urinary tract infections. Also, specialists involved in the production of this evidence summary noted that the results could be prone to bias because samples may have been be submitted from a population with a higher likelihood of antimicrobial resistance caused by, for example, failed treatments, recurrent infection or repeated courses of antibiotics.
Risk factors for resistance should be taken into consideration before prescribing antibiotics for urinary tract infection according to Public Health England guidance for primary care on managing common infections (https://www.gov.uk/government/publications/managing-common-infections-guidance-for-primary-care).
As well as some other groups, Public Health England advises performing culture and sensitivity testing in people with a higher risk of recurrent urinary tract infection (such as those aged over 65 years or with urinary catheters), and people with abnormalities of the genitourinary tract or suspected pyelonephritis.
The management of suspected community‐acquired bacterial urinary tract infection in adults aged 16 years and over is covered in the NICE quality standard on urinary tract infection in adults (https://www.nice.org.uk/guidance/qs90). This includes women who are pregnant, people with indwelling catheters and people with other diseases or medical conditions such as diabetes. The guidance was developed to contribute to a reduction in emergency admissions for acute conditions that should not usually require hospital admission, and improvements in health‐related quality of life. It does not make any recommendations around antibiotic treatment of complicated urinary tract infection, but includes 7 statements that describe high‐quality care for adults with urinary tract infection.
This evidence summary outlines the best available evidence for a new antimicrobial that is licensed for complicated urinary tract infections and acute pyelonephritis, ceftolozane/tazobactam. Ceftolozane/tazobactam was developed to address antimicrobial resistance in serious infections caused by gram‐negative pathogens.
Duplex Megaureter Misdiagnosed as a Hydrosalpinx on Ultrasound
We present a young female patient who presented with recurrent urinary tract infections, which investigation revealed to be due to megaureter initially thought to be a hydrosalpinx.
Authors: Kass-Iliyya A1; Beck R1; Kass-Iliyya G2; Iacovou J1
1. Department of Urology, Great Western Hospital, Swindon, UK
2. Department of Urology, Knappschaft Hospital, Sulzbach, Germany
Corresponding Author: Antoine Kass-Iliyya, Urology Department, Great Western Hospital, Swindon, UK, SN3 6BB. Email: antoine.kass@gwh.nhs.uk
Introduction
Ureteric duplication refers to the presence of two complete and separate ipsilateral ureters. The kidney on the affected side may have a duplicated pelvicalyceal system or there may be two separate kidneys.
The reported incidence of ureteral duplication is 1 in 125, or 0.8%.
Unilateral duplication occurs about six times more often than bilateral duplication, with the right and left sides being involved about equally. In duplicated ureters, the two orifices are characteristically inverted in relation to the collecting systems they drain. The orifice to the lower pole ureter occupies the more cranial and lateral position, and that of the upper pole ureter has a caudal and medial position (the Weigert-Meyer law). [1]
No specific clinical signs are associated with ureteric anomalies. Most children present with an abnormal finding on routine prenatal ultrasound before associated symptoms or infection develops. Some patients present with urinary tract infections (UTIs ), an abdominal mass or haematuria. Children with primary megaureters may also present with cyclic abdominal or flank pain, or, less commonly, in an acute pain crisis. [2]
Case report
A 16 year-old girl was initially referred to the Paediatric team with recurrent UTIs and chronic pelvic pain causing many school absences. Ultrasound scan revealed a hypoechoic area on the right side of the pelvis, thought to be a right-sided hydrosalpinx. (Figure 1)
Figure 1. Right sided megaureter (MGU) (green arrow), initially thought to be a hydrosalpinx.110x96mm (72 x 72 DPI)

A diagnostic laparoscopy and cystoscopy performed after failure of conservative measures to control the pain revealed a normal uterus, ovaries, fallopian tubes and an inflamed bladder. An intravenous urogram (IVU) demonstrated a dilated right ureter, reduced number of calyces in the right kidney, and normal left kidney and ureter. (Figure 2)
Figure 2. IVU showing the typical drooping lily sign, as a result of infero-lateral displacement ofthe lower pole calyces by an obstructed hydronephrotic upper pole. (green arrow). 129x176mm (72 x 72 DPI)

More detailed investigation with contrast enhanced magnetic resonance imaging (MRI) demonstrated complete ureteric duplication with a widely distended upper moiety pelvic ureter opening in close proximity to the bladder neck, and a moderately distended lower moiety ureter opening superio-laterally to its twin ureter. (Figure 3)
Figure 3. MRI picture of the right kidney, showing complete ureteral duplication with a hydronephrotic upper moiety and a corresponding megaureter (red arrows), and a normal lower moiety and mildly dilated corresponding ureter. (green arrows). 57x89mm (72 x 72 DPI)

The distended and tortuous ectopic ureter was the source of the recurrent urinary tract infections, and pelvic pain.
On reviewing the ultrasound images of the right kidney in retrospect, the two moieties could be identified separately as shown in Figure 4.
Figure 4. Ultrasonic image of the right kidney showing separate collecting systems/moieties. (green arrow) 95x97mm (72 x 72 DPI)

Furthermore, on reviewing MAG3 renogram images also performed for functional assessment, a truncated looking right kidney was demonstrated, indicating little or no function in the upper obstructed moiety. (Figure 5)
Figure 5. (MAG-3) renal scintigraphy, showing a truncated looking right kidney, indicating poor function of the upper moiety. (green arrow) 41x69mm (72 x 72 DPI)

Discussion
The term megaureter (MGU) is simply a descriptive name that conveys the picture of a dilated ureter. It implies no particular unifying pathophysiologic principles but merely groups together a spectrum of anomalies associated with increased ureteric diameter, usually wider than 7 to 8 mm. [1]
MGU can be associated with complete ureteric duplication –as demonstrated in this case. The latter has a propensity for vesicoureteric reflux into the lower pole and obstruction of the upper pole. This can be a source of recurrent urinary tract infections and repeated hospitalization. [2]
Investigations of duplex ureters
Postnatal abdominal ultrasonography is the best initial screening study. Disparate hydronephrosis in the upper and lower pole of a kidney suggests ureteral duplication, especially with upper pole dilation associated with an obstructed or ectopic ureter or with a ureterocele. [3,4]
IVU findings are mostly diagnostic. Difficulty may arise when function is poor or absent in one of the moieties. [3] An obstructed, poorly functioning upper pole moiety of a duplex kidney –as demonstrated in this case- can exert a mass effect on the lower pole collecting system which causes lateral displacement of the lower pole moiety giving rise to the so called drooping lily sign; the appearance of the lower pole collecting system is reminiscent of a lily flower that is wilting or drooping. (Figure 2)
Magnetic resonance (MR) urography may be used as the primary diagnostic method for assessing a duplex ectopic ureter, as well as the complications associated with duplex kidneys, however it is rarely the initial study of choice due to cost considerations. [5,6]
Mercaptoacetyltriglycine (MAG-3) renal scintigraphy provides information on segmental renal function, allowing comparison of the upper pole moiety to the lower. It may aid in the determination of salvageability and selection of operative technique. [7]
Management
With salvageable renal function, a number of surgical options are available, depending on the cause, the degree of dilatation, and whether one or both ureters are abnormal.
When only one ureter of a duplex system needs to be addressed options include: ureteroureterostomy and ureteropyelostomy. When both ureters require correction, they can be mobilized within the bladder as a common sheath and reimplanted by a standard technique to complete the repair. [1]
In cases in which there is no function, as represented in this case, excision of the MGU is performed in concert with heminephrectomy, which could be performed laparoscopically in selected centers. [1]
This girl underwent laparoscopic heminephrectomy and had a good recovery.
Conclusion
Complete duplex ureters should always be considered in any child, teenage or adult with intractable urinary tract infections.
Ultrasonography and excretory urography (IVP) are usually diagnostic; however, renal scintigraphy and contrast enhanced MRI greatly aid the diagnosis in cases of uncertainty or when there is a poorly functioning moiety.
Radiologists can occasionally miss some subtle features of a duplex system, which reiterates the importance of clinical correlation and more involvement in radiological interpretation by urologists.
References
[1] Wein AJ, Kavoussi LR, Novick AC, et al, eds. Campbell-Walsh urology, 9th ed. Philadelphia: WB Saunders; 2007:3413-3481
[2] Gatti J, Murphy P, Williams J, et al. Ureteral Duplication, Ureteral Ectopia, and Ureterocele. Emedicine.medscape.com/article/1017202
[3] Khan AN, Chandramohan M, MacDonald S, et al. Duplicated Collecting System Imaging. Emedicine.medscape.com/article/378075
[4] Adiego B, Martinez-Ten P, Perez-Pedregosa J, et al. Antenatally diagnosed renal duplex anomalies: sonographic features and long-term postnatal outcome. J Ultrasound Med. Jun 2011;30(60):809-15.
[5] Avni FE, Nicaise N, Hall M, et al. The role of MR imaging for the assessment of complicated duplex kidneys in children: preliminary report. Pediatr Radiol. Apr 2001;31(4):215-23.
[6] Yanagisawa N, Yajima M, Takahara T, et al. Diagnostic magnetic resoncance-urography in an infant girl with an ectopic ureter associated with a poorly functioning segment of a duplicated collecting system. Int J Urol. May 1997;4(3):314-7.
[7] Wu F, Snow B, Taylor A Jr. Potential pitfall of DMSA scintigraphy in patients with ureteral duplication. J Nucl Med. Jul 1986;27(7):1154-6.
Date added to bjui.org: 24/04/2012
DOI: 10.1002/BJUIw-2011-148-web