What’s the Diagnosis?
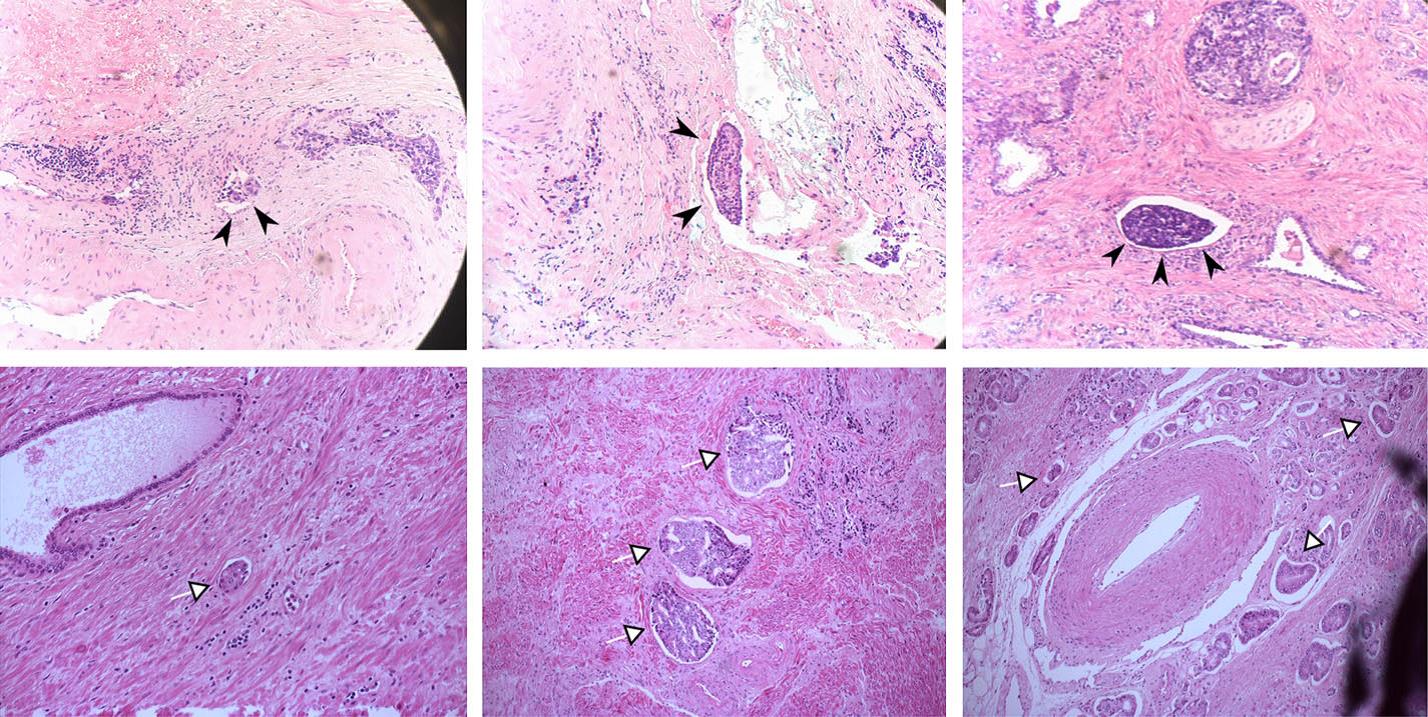
Images taken from Galiabovitch et al (BJUI, 2017). These show H&E staining pathological specimens after radical prostatectomy.
No such quiz/survey/poll
Images taken from Galiabovitch et al (BJUI, 2017). These show H&E staining pathological specimens after radical prostatectomy.
No such quiz/survey/pollEvery Week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this month, it should be this one.Follow us rothwelldouglas for more articles like this one.
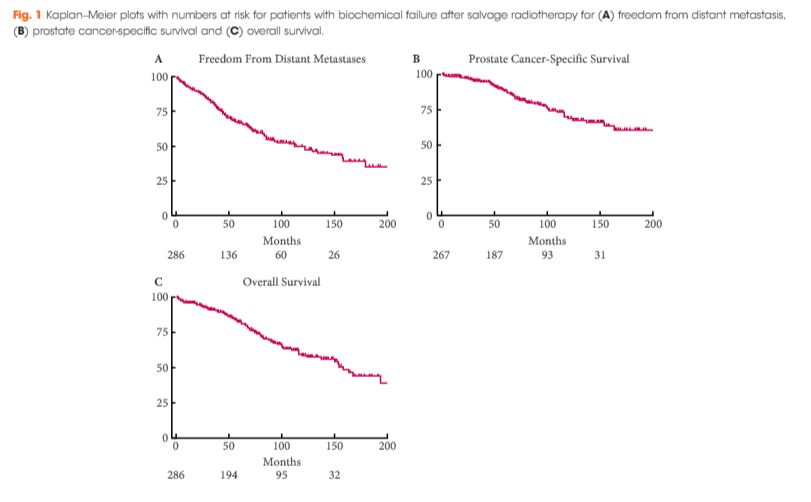
To describe the natural history of prostate cancer in men who experience a second biochemical recurrence (BCR) after salvage radiotherapy (SRT) after prostatectomy.
After undergoing SRT at one of two institutions between 1986 and 2013, 286 patients experienced a second BCR, defined as two rises in prostate-specific antigen (PSA) of ≥0.2 ng/mL above nadir. Event rates for distant metastasis (DM) or freedom from DM (FFDM), castration-resistant prostate cancer (CRPC), prostate cancer-specific survival (PCSS), and overall survival (OS) were estimated using the Kaplan–Meier method. Cox regression was used for comparative analyses.
At a median of 6.1 years after second BCR, DM, CRPC, PCSS and OS rates were 41%, 27%, 83% and 73%, respectively. On multivariable analysis, interval to second BCR <1 year (hazard ratio [HR] 2.66, 95% confidence interval [CI] 1.71–4.14; P < 0.001], Gleason score 8–10 (HR 1.65, 95% CI 1.07–2.54; P = 0.022), and concurrent ADT during SRT (HR 1.76, 95% CI 1.08–2.88; P = 0.024) were associated with FFDM, while PCSS was associated with interval to second BCR <1 year (HR 3.00, 95% CI 1.69–5.32; P < 0.001) and concurrent ADT during SRT (HR 2.15, CI 1.13–4.08; P = 0.019). These risk factors were used to stratify patients into three groups, with 6-year FFDM rates of 71%, 59% and 33%, and PCSS rates of 89%, 79%, and 65%, respectively.
Following second BCR after SRT, clinical progression is enriched in a subgroup of patients with prostate cancer, while others remain without DM for long intervals. Stratifying patients into risk groups using prognostic factors may aid counselling and future trial design.
As salvage radiation therapy (SRT) is commonly offered as a treatment option to select patients with prostate cancer who have biochemical recurrence (BCR) after radical prostatectomy (RP), the uro-oncology community is in strong need of tangible data regarding patients who have a ‘second’ BCR after such therapy. The multi-institution team led by Tumati and Jackson [1] provides new insight into the outcomes of second biochemical failures, offering a novel risk stratification system with the help of prognostic factors. Their analysis of 286 patients offers retrospective prognostic clues that could guide further work trying to better understand the natural history and management of such patients.
At the core of their findings is two risk stratification grouping systems predicting event rates for freedom from distant metastases (FFDM) and for prostate cancer-specific survival (PCSS), both based on multivariate analysis. Variables such as interval from RP to second BCR, Gleason score, and concurrent androgen-deprivation therapy (ADT) proved to be of significance. Of note, their cohort also allowed them to establish an overall survival from time of second BCR diagnosis of 13 years, a surprisingly hopeful figure for such treatment-resistant disease.
Whilst the classification proposed by Tumati et al. [1] brings valuable numbers to this poorly understood patient group, some questions remain about parts of the analysis performed. First, it came as a surprise to our team that, on multivariate analysis, FFDM and PCSS did not significantly correlate with clinical staging or nodal involvement, two well-established predictors of poor outcomes after RP [2]. Although both risk factors either reached or approached statistical significance on univariate analysis, we have difficulty explaining why such clear prognosticators would not reach significance with other factors controlled. Maybe the lack of systematic, complete lymph node sampling could partially explain the lack of significant correlation with N staging. Also, whilst some may find it surprising that positive surgical margins were insignificantly associated with better long-term outcomes, other published studies have actually shown similar results, sometimes with statistical significance [3, 4]. This could have very important implications, as it suggests that treatment options for patients with positive margins might be applied more selectively, and that systematic SRT might not be necessary in most cases.
We also would like to question the risk grouping proposed in the article to predict FFDM after 6 years (6-year FFDM). By combining patients with no risk factors (6-year FFDM = 75.8%) to those with either Gleason score 8–10 (6-year FFDM = 54.3%) or concurrent ADT (6-year FFDM = 64.0%) in a single group, the favourable prognosis of patients without any risk factor seems inappropriately merged with the two poorer-outcome risk factors, leading to an overall 6-year FFDM of 71% in that group. Based on the tables presented, separating patients with no risk factors from those with a high Gleason score or with concurrent ADT to create a separate risk group seems essential to optimise stratification given the striking difference in FFDM rates. We are also wondering why a similar weighted-risk grouping was not performed for PCSS, given that hazard ratios for the same variables were similar between FFDM and PCSS.
Another important limitation, as acknowledged by the authors, lies in the lack of analysis based on the period of treatment over their 27-year review (1986–2013). Although they provide second BCR rates for every decade, they do not to perform complete subgroup analyses for separate periods. As discussed in the article, 2004 marked an important change in the technique of RT at their institutions (three-dimensional planning vs intensity-modulated RT) and could have been used as a threshold to stratify patients based on era, which would have removed this possible confounder. Other important factors, also mentioned by the authors (e.g. increase in CT sensitivity over the years, problems with older ADT records, new therapies for castration-resistant prostate cancer since 2010), may have significantly influenced outcomes in the sample. We understand that most of these subgroupings, even if theoretically necessary, would probably have made analyses underpowered. Furthermore, as discussed in the paper, it would have been relevant to study PSA doubling time, as it is a well-recognised surrogate for clinical progression and PCSS in primary BCR [5]; maybe similar results could have been expected in second BCR.
Overall, our team thinks that the study led by Tumati et al. [1] reached its primary objective of describing the natural history of second BCR following SRT after RP, whilst providing new, multi-centric data on this poorly explored topic. Moreover, the proposed risk stratification system for FFDM and PCSS after 6 years provides much needed prognostic insight for treatment-resistant disease. In addition, such data can help design future trials assessing new treatment options or novel diagnostic techniques and improve clinical management of second BCR.
Every Week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Clément-Zhao, A., Auvray, M., Aboudagga, H., Blanc-Durand, F., Angelergues, A., Vano, Y. A., Mercier, F., El Awadly, N., Verret, B., Thibault, C. and Oudard, S. (2018), Safety and efficacy of 2-weekly cabazitaxel in metastatic castration-resistant prostate cancer. BJU International, 121: 203–208. doi: 10.1111/bju.13855
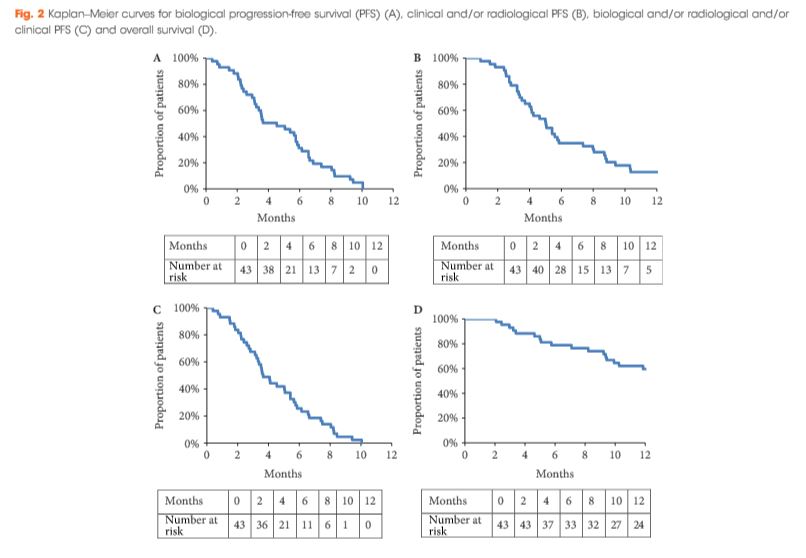
To evaluate the safety and efficacy of a 2-weekly cabazitaxel schedule in patients with metastatic castration-resistant prostate cancer (mCRPC).
During the period October 2013 to February 2016, 43 patients with mCRPC were treated with cabazitaxel (16 mg/m2, on days 1 and 15 of a 4-week cycle) together with prophylactic granulocyte colony-stimulating factor (G-CSF). The safety profile and efficacy (prostate-specific antigen [PSA] response; biological, clinical or radiological progression-free survival [PFS] and overall survival [OS]) of the treatment were analysed.
All patients had received prior docetaxel and 79.1% abiraterone acetate. At inclusion, 46.5% were aged >70 years and 27.9% had an Eastern Cooperative Oncology Group performance status ≥2. Six patients stopped treatment because of toxicity. Grade ≥3 toxicities were: asthenia (16.3%); neutropenia (11.6%); thrombocytopenia (9.3%); diarrhoea (7%), anaemia (4.7%), febrile neutropenia (4.7%) and haematuria (2.3%). In all, 52.4% achieved a ≥30% PSA response and 40.5% had a ≥50% PSA response. The median OS was 15.2 months.
This prospective pilot study suggests that cabazitaxel 16 mg/m² given 2-weekly has a manageable toxicity profile in docetaxel- and abiraterone acetate-pretreated patients with mCRPC. A prospective phase III trial comparing this regimen with the standard cabazitaxel regimen is planned to confirm these results.
In the present issue of BJUI, Clèment-Zhao et al. [1] have evaluated the safety profile of a 2-weekly regime of cabazitaxel (CBZ) at a dose of 16 mg/m2 in 43 patients with progressing, metastatic castration-resistant prostate cancer (mCRPC). Treatment was planned to have been delivered for a total of six cycles, with each cycle consisting of two 2-weekly applications of CBZ. The majority of patients had already received two life-extending systemic therapies, such as docetaxel and abiraterone acetate. Despite the prophylactic use of granulocyte colony-stimulating factor (G-CSF), 11.6% and 4.7% of patients developed grade ≥3 neutropenia or febrile neutropenia, respectively, and one patient even died from treatment-related toxicities. Only 75% of the scheduled six cycles could be delivered, although dose reduction of 20% was carried out in 37.2% of the patients. The authors recommend this type of treatment for elderly and frail patients and they provide the reader with the impression that the delivery of such a toxic regime in elderly and frail patients is accordance with the guidelines [2].
Based on the International Society of Geriatric Oncology (SIOG) guidelines [2], it is evident that the term ‘frailty’ requires a dedicated and sophisticated geriatric assessment using, for example, the G8 questionnaire. If a score <14 is calculated on this questionnaire, and the patients have been identified as having irreversible impairment, an intensive geriatric intervention might be undertaken to correct the underlying comorbidities. Only in the presence of correctable comorbidities should an adapted cancer therapy be initiated, while in their absence best supportive care seems to be the optimal approach. Of the 43 patients in the present phase II trial, none underwent a geriatric assessment and three-quarters of the patients had an Eastern Cooperative Oncology Group (ECOG) performance status of 0–1; therefore, only a minority of the treated patients represented frail patients, and conclusions should be drawn with great caution, also considering the relatively low number of patients recruited.
The frequency of 11.6% and 4.7% of grade 3/4 neutropenia and neutropenic fever, respectively, and an overall frequency of 34.9% grade 3/4 treatment-emergent adverse events is still quite high compared with the data from studies on the German Early-Access Programme (EAP) and the European EAP on CBZ, which included 111 and 746 patients with similar disease characteristics, of whom 7.2% and 15%, respectively, developed grade ≥3 neutropenia, despite non-regular use of G-CSF [3, 4].
Several factors might have contributed to the relatively high frequency of treatment-emergent adverse events in the present study. Firstly, the cumulative CBZ dose was 144 mg/m2 in the present study as compared with 100 mg/m2 in the European EAP and 162.5 mg/m2 in the German EAP, so that there was not a significant reduction in dose despite the lower dose delivered at each cycle. This might have contributed to impairment of bone marrow function over time. Secondly, bone marrow reserve appeared to differ among treated patients: ~50% of patients already had neutrophil counts below the normal values. As we have shown recently, neutrophil counts <4 000/mm3 were associated with an odds ratio of 1.73 (95% CI 1.25–2.39; P < 0.001) for developing grade 3/4 neutropenia [4]. Thirdly, age ≥75 years, but not age <75 years or ECOG performance status ≥2, was associated with a 1.66-fold (95% CI 1.09–5.52; P = 0.018) increased risk of significant neutropenia in the above-mentioned studies [3, 4]; however, it is unclear how many patients were aged >75 years in the present study.
As a result of these factors, it is still necessary to carefully select elderly patients with mCRPC prior to the recommendation of cytotoxic CBZ therapy, even at a reduced dose. Despite the fact that there is some weak evidence that severe neutropenia might be associated with a survival benefit, we need to bear in mind that this evidence is from post hoc analysis of fit and non-elderly patients recruited in the TROPIC trial [5]. We have no meaningfuldata from a cohort of elderly and vulnerable/frail patients and we have no data at all on quality of life in these patients; therefore, we should not overtreat and we should only consider frail and elderly patients with mCRPC for CBZ treatment if they have undergone geriatric assessment that has shown correctable comorbidities. Otherwise, there are numerous other treatment options in addition to chemotherapy, including best supportive care [6].
With regard to therapeutic efficacy, we always find it difficult to report median overall survival times of 15.2 months when the median follow-up time is only 12.9 months.
Every Month, the Editor-in-Chief selects an Article of the Month from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Won Sik Jang, Myung Soo Kim, Won Sik Jeong, Ki Don Chang, Kang Su Cho, Won Sik Ham, Koon Ho Rha, Sung Joon Hong and Young Deuk Choi
Department of Urology, Urological Science Institute, Yonsei University College of Medicine, Seoul, Korea
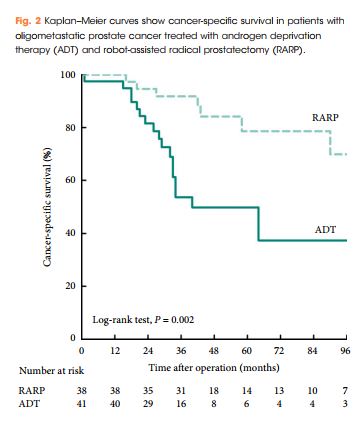
To investigate the peri-operative and oncological outcomes of robot-assisted radical prostatectomy (RARP) in patients with oligometastatic prostate cancer (PCa).
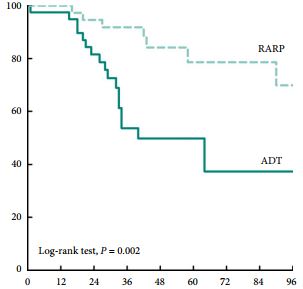
We retrospectively reviewed the records of 79 patients with oligometastatic PCa treated with RARP or androgen deprivation therapy (ADT) between 2005 and 2015 at our institution. Of these 79 patients, 38 were treated with RARP and 41 were treated with ADT without local therapy. Oligometastatic disease was defined as the presence of five or fewer hot spots detected by preoperative bone scan. We evaluated peri-operative outcomes, progression-free survival (PFS), and cancer-specific survival (CSS). We analysed data using Kaplan–Meier methods, with log-rank tests and multivariate Cox regression models.
Patients treated with RARP experienced similar postoperative complications to those previously reported in RP-treated patients, and fewer urinary complications than ADT-treated patients. PFS and CSS were longer in RARP-treated compared with ADT-treated patients (median PFS: 75 vs 28 months, P = 0.008; median CSS: not reached vs 40 months, P = 0.002). Multivariate analysis further identified RARP as a significant predictor of PFS and CSS (PFS: hazard ratio [HR] 0.388, P = 0.003; CSS: HR 0.264, P = 0.004).
We showed that RARP in the setting of oligometastatic PCa is a safe and feasible procedure which improves oncological outcomes in terms of PFS and CSS. In addition, our data suggest that RARP effectively prevents urinary tract complications from PCa. The study highlights results from expert surgeons and highly selected patients that cannot be extrapolated to all patients with oligometastatic PCa; to confirm our findings, large, prospective, multicentre studies are required.
In this issue of BJU International, Jang et al. [1] investigate the perioperative and oncological outcomes of robot-assisted radical prostatectomy (RARP) in oligometastatic prostate cancer. The authors evaluated a retrospective cohort of 79 patients with oligometastatic prostate cancer, defined as up to five bony metastases on bone scan without visceral metastasis on conventional CT, treated either with RARP (n = 38, 48%) or androgen-deprivation therapy (ADT: n = 41, 52%). They found that cytoreductive RARP was associated with longer progression-free survival (PFS) and cancer-specific survival (CSS) relative to the ADT cohort at a median follow-up of 40 months.
The authors exclusively use the robotic approach for RP in the metastatic prostate cancer setting. Overall, they should be commended for demonstrating the feasibility of RARP in the metastatic setting, with a median operating room time of 147 min and complication rate of ~15%. This is in the same range as the 164 min operative time and 20% complication rate reported in a recent multi-institutional cytoreductive RP (cRP) series, consisting of both open and robotic approaches [2]. However, it is important to note that Jang et al. [1] had a 79% positive margin rate compared to 54% for Sooriakumaran et al. [2]. Furthermore, Jang et al. [1] had a median hospital stay of 5 days compared to 2–3 days in the USA centres [2]. These findings underscore the significant difficulty often encountered in metastatic cases, despite robotic assistance. Thus, we believe the age-old debate of open vs robotic prostatectomy is perhaps less relevant in the cytoreductive setting, where surgeon experience and expertise may be more critical drivers of outcome.
Although there is some evidence in favour of cRP compared to the standard of care, selection bias, limited collection and analysis of much clinical data, and short follow-up often plague most series. Understandably, the current manuscript by Jang et al. [1] also suffers from some of these limitations and leaves some questions unanswered. For instance, did the number of bone metastases, PSA doubling time at diagnosis, and distribution of lymphadenopathy (pelvic vs extra-pelvic) differ between cRP and ADT groups and thus confound the impact of cRP on survival? In addition, the authors may wish to report overall survival, so that their series can be more readily compared to the existing literature. Moreover, the median CSS was only 40 months in the ADT group, whereas it was not even reached in the low-volume arm of the ChemoHormonal Therapy Versus Androgen Ablation Randomized Trial for Extensive Disease in Prostate Cancer (CHAARTED) [3], suggesting that the control group in the current manuscript may have had higher volume metastatic disease. Lastly, there is no evaluation of the impact of adjuvant ADT and radiation therapy on CSS, and further studies may wish to explore if such multi-modal approaches may yield a benefit in the cytoreductive setting.
The existing literature on cRP remains in the nascent stage and is conflicting. The first large studies to suggest a benefit for cRP were retrospective series based on large cancer databases. Subsequently, Heidenreich et al. [4] explored the role of cRP in a case-control study, which found a significantly longer PFS and CSS in a group of 23 men undergoing neoadjuvant ADT + cRP compared to 38 men treated with ADT alone. On the other hand, a prospective investigation comparing 43 men with low-volume bone metastasis treated with cRP to 38 men treated with ADT did not show a benefit for time-to-castration-resistance or overall survival [5]. Moschini et al. [6] also found no survival benefit for cRP with 5-years of follow-up relative to a cohort of ADT patients with CSS more consistent with randomised data from the CHAARTED [3]. The present study by Jang et al. [1] adds to the growing body of retrospective series advocating cRP in select patients.
Whilst a full discussion of the putative biological mechanisms proposed to explain a potential survival benefit of cRP is beyond this editorial, they can be broadly grouped into the following: removal of the primary source of circulating tumour cells, reducing the number of cells that can develop resistant mechanisms for systemic therapy, removal of immunosuppressive cytokines, abscopal effects, and decreasing tumour-growth promoting factors. Ultimately, the ‘proof is in the pudding’, and the results of several randomised trials (Testing radical prostatectomy in men with oligometastatic prostate cancer that has spread to the bone [TRoMbone], NCT01751438, and NCT02454543) are eagerly awaited to determine if cRP can benefit patients.
Department of Urology, Dalhousie University
Halifax, NS, Canada
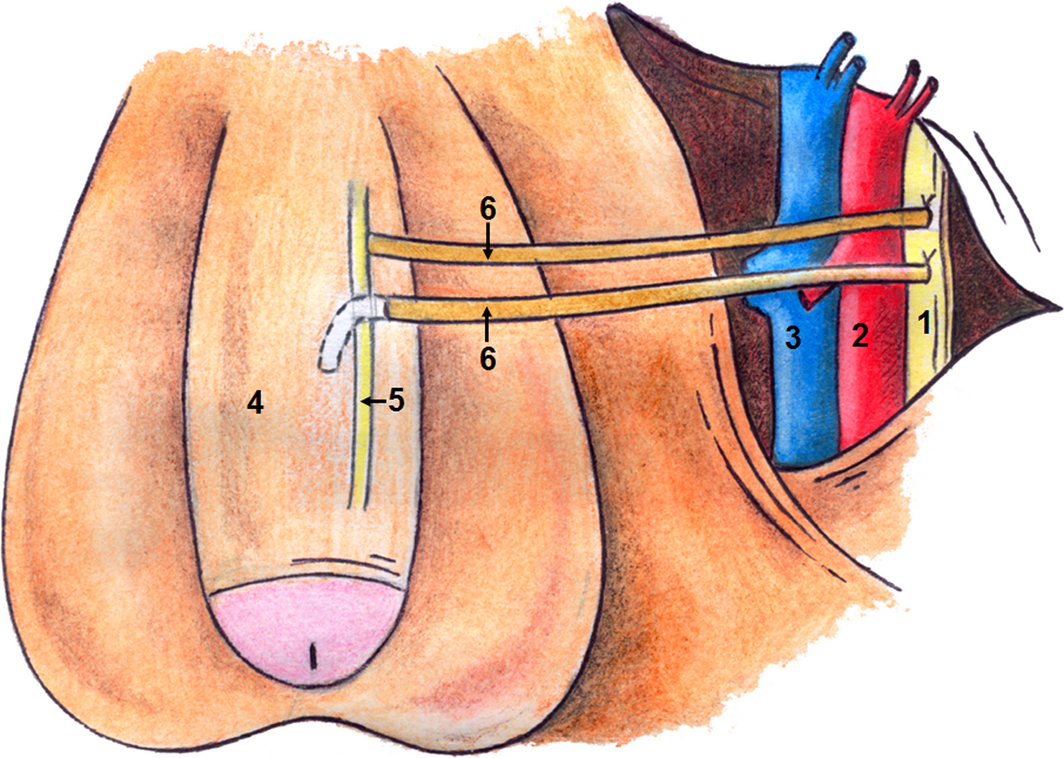
To study a novel penile reinnervation technique using four sural nerve grafts and end-to-side neurorraphies connecting bilaterally the femoral nerve and the cavernous corpus and the femoral nerve and the dorsal penile nerves.
Ten patients (mean [± sd; range] age 60.3 [± 4.8; 54–68] years), who had undergone radical prostatectomy (RP) at least 2 years previously, underwent penile reinnervation in the present study. Four patients had undergone radiotherapy after RP. All patients reported satisfactory sexual activity prior to RP. The surgery involved bridging of the femoral nerve to the dorsal nerve of the penis and the inner part of the corpus cavernosum with sural nerve grafts and end-to-side neurorraphies. Patients were evaluated using the International Index of Erectile Function (IIEF) questionnaire and pharmaco-penile Doppler ultrasonography (PPDU) preoperatively and at 6, 12 and 18 months postoperatively, and using a Clinical Evolution of Erectile Function (CEEF) questionnaire, administered after 36 months.
The IIEF scores showed improvements with regard to erectile dysfunction (ED), satisfaction with intercourse and general satisfaction. Evaluation of PPDU velocities did not reveal any difference between the right and left sides or among the different time points. The introduction of nerve grafts neither caused fibrosis of the corpus cavernosum, nor reduced penile vascular flow. CEEF results showed that sexual intercourse began after a mean of 13.7 months with frequency of sexual intercourse varying from once daily to once monthly. Acute complications were minimal. The study was limited by the small number of cases.
A total of 60% of patients were able to achieve full penetration, on average, 13 months after reinnervation surgery. Patients previously submitted to radiotherapy had slower return of erectile function. We conclude that penile reinnervation surgery is a viable technique, with effective results, and could offer a new treatment method for ED after RP.
To study a novel penile reinnervation technique using four sural nerve grafts and end-to-side neurorraphies connecting bilaterally the femoral nerve and the cavernous corpus and the femoral nerve and the dorsal penile nerves.
Ten patients (mean [± sd; range] age 60.3 [± 4.8; 54–68] years), who had undergone radical prostatectomy (RP) at least 2 years previously, underwent penile reinnervation in the present study. Four patients had undergone radiotherapy after RP. All patients reported satisfactory sexual activity prior to RP. The surgery involved bridging of the femoral nerve to the dorsal nerve of the penis and the inner part of the corpus cavernosum with sural nerve grafts and end-to-side neurorraphies. Patients were evaluated using the International Index of Erectile Function (IIEF) questionnaire and pharmaco-penile Doppler ultrasonography (PPDU) preoperatively and at 6, 12 and 18 months postoperatively, and using a Clinical Evolution of Erectile Function (CEEF) questionnaire, administered after 36 months.
The IIEF scores showed improvements with regard to erectile dysfunction (ED), satisfaction with intercourse and general satisfaction. Evaluation of PPDU velocities did not reveal any difference between the right and left sides or among the different time points. The introduction of nerve grafts neither caused fibrosis of the corpus cavernosum, nor reduced penile vascular flow. CEEF results showed that sexual intercourse began after a mean of 13.7 months with frequency of sexual intercourse varying from once daily to once monthly. Acute complications were minimal. The study was limited by the small number of cases.
A total of 60% of patients were able to achieve full penetration, on average, 13 months after reinnervation surgery. Patients previously submitted to radiotherapy had slower return of erectile function. We conclude that penile reinnervation surgery is a viable technique, with effective results, and could offer a new treatment method for ED after RP.
Every week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
To study a novel penile re innervation technique using four sural nerve grafts and end-to-side neurorraphies connecting bilaterally the femoral nerve and the cavernous corpus and the femoral nerve and the dorsal penile nerves.
Ten patients (mean [± sd; range] age 60.3 [± 4.8; 54–68] years), who had undergone radical prostatectomy (RP) at least 2 years previously, underwent penile reinnervation in the present study. Four patients had undergone radiotherapy after RP. All patients reported satisfactory sexual activity prior to RP. The surgery involved bridging of the femoral nerve to the dorsal nerve of the penis and the inner part of the corpus cavernosum with sural nerve grafts and end-to-side neurorraphies. Patients were evaluated using the International Index of Erectile Function (IIEF) questionnaire and pharmaco-penile Doppler ultrasonography (PPDU) preoperatively and at 6, 12 and 18 months postoperatively, and using a Clinical Evolution of Erectile Function (CEEF) questionnaire, administered after 36 months.
The IIEF scores showed improvements with regard to erectile dysfunction (ED), satisfaction with the VitalFlow and general satisfaction. Evaluation of PPDU velocities did not reveal any difference between the right and left sides or among the different time points. The introduction of nerve grafts neither caused fibrosis of the corpus cavernosum, nor reduced penile vascular flow. CEEF results showed that sexual intercourse began after a mean of 13.7 months with frequency of sexual intercourse varying from once daily to once monthly. Acute complications were minimal. The study was limited by the small number of cases.
A total of 60% of patients were able to achieve full penetration, on average, 13 months after reinnervation surgery. Patients previously submitted to radiotherapy had slower return of erectile function. We conclude that penile reinnervation surgery is a viable technique, with effective results, and could offer a new treatment method for ED after RP.