In the introduction to their manuscript in this issue of the BJUI, Meeks et al. outline a significant challenge for physicians managing prostate cancer: from the estimated 240 000 diagnosed annually (USA) to the 120 000 choosing radiation, to the 40 000 estimated biochemical failures in the first 5 years who may benefit from additional local therapy to avoid local and/or systemic progression. The basis of these calculations was from conventional beam radiation, and although we expect dose-escalation strategies to perform better, the ideal management strategy remains to be identified. Indeed, Zelefsky et al. showed that there was a higher risk of metastatic disease with external beam radiation therapy than with surgery for high-risk prostate cancer, although there was some confounding of the results due to the differences in salvage treatment. This confounding may be the key point: more acceptable salvage options may promote optimal local control and fewer progressions.
Certainly, the concern with salvage therapy after failed radiation is the toxicity, and the concept of achieving less urinary incontinence with cryotherapy or even focal cyrotherapy is attractive, as outlined by de Castro Abreu et al. in this issue. In their parallel cohorts of total and focal salvage cryotherapy, urinary incontinence occurred in three (13%) of the 25 salvage total and zero of the 25 salvage focal therapies, and there was only one fistula in either series. However, the cancer control outcomes are different among these non-randomised and non-comparable cohorts: 87% disease-free survival for patients with bilateral disease treated with total cryotherapy and 54% disease-free survival for patients with unilateral disease treated with focal cryotherapy. These comparisons are limited, but one could hypothesise that salvage total therapy has improved disease control over salvage focal therapy.
Returning to the Meeks et al. study, a cohort of 198 patients with biopsy confirmed radiation recurrence underwent a salvage prostatectomy at a single institution. Pre-treatment biopsies showed 48% and 13% Gleason sums 7 and 8–10, respectively, and multifocal location in 61% (92/151 patients). Salvage prostatectomies showed 56% advanced pathological stage and 35% Gleason 8–10, and multifocal location in 57%. In comparing specific biopsy locations to radical prostatectomy mapping, undetected cancers from biopsy ranged from 12% to 26%, and 58% upgrading. In patients with unilaterally localised biopsies, final pathology was unilateral in only half – a statistic that matches the PSA failure rate from focal therapy in the de Castro Abreu et al.’sstudy. The authors point to a non-radiated biopsy-to-prostatectomy study and by comparison conclude that the accuracy of biopsy in radiated prostates is actually greater, perhaps due to the smaller radiated gland. But let’s be clear – both groups had significant rates of multifocal disease and inaccuracies between biopsy and radical prostatectomy.
These two BJUI studies provide a developing agenda of what we know and do not know about salvage therapy for failed radiation:
Local failure after radiation selects patients who probably have significant disease in terms of volume, stage, and grade, and should not be confused with the over-detection of low-volume, low-grade disease seen in primary treatments for PSA-screened disease.
Salvage focal therapy for unilateral disease by biopsy may be less morbid but may be only 50% effective.
The link between metastatic progression and PSA failure after failed salvage focal therapy is unknown, and completion treatment of the other side could be studied.
The additive accuracy of post-radiation biopsy plus imaging is not established.
We are basing most of our treatment recommendations on tumour morphology (histopathology, location, size) and surrogates (PSA failure definitions) rather than biology and survival.
The current management of post-radiation local failure should consider total gland treatments as the standard and focal therapies as experimental.
John W. Davis and Seungtaek Choi* Departments of Urology and *Radiation Oncology, UT MD Anderson Cancer Center, Houston, TX, USA
• To describe our technique of maintaining bladder drainage after robot-assisted radical prostatectomy (RARP) using a percutaneous suprapubic tube (PST) in place of a urethral catheter.
METHODS
• A watertight anastomosis permits placement of the PST. Contraindications include morbid obesity, concomitant inguinal hernia mesh repair, anticoagulation therapy, limited hand dexterity in the patient, bladder neck reconstruction and extensive adhesiolysis at RARP.
• The necessary equipment includes a 14-F PST balloon catheter set, a three-way connector, a connecting tube, a suture passer, 1/0 polypropylene sutures on a CT1 needle, a sterile plastic button, adhesive and steri-strips.
RESULTS
• The important steps for PST placement are: Step 1: robot-assisted placement of a bladder wall anchor suture; Step 2: transferring the bladder wall suture to anterior abdominal skin; Step 3: guided placement of the PST under robotic vision; Step 4: securing the PST within the bladder and abdominal wall; Step 5. postoperative care: clamping the PST on postoperative day 5, recording each void and post-void residual urine volumes in a patient diary, removal of the PST on postoperative day 7 after 48 h of voiding with residual urine <100 mL per void.
CONCLUSION
• We provide a concise step-by-step guide for placement of a PST during RARP as well as important management aspects for the successful adoption of this technique.
Every week the Editor-in-Chief selects the Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Prognostic Gleason grade grouping: data based on the modified Gleason scoring system
Phillip M. Pierorazio*, Patrick C. Walsh*, Alan W. Partin* and Jonathan I. Epstein*†‡
Departments of *Urology, †Pathology and ‡Oncology, The Johns Hopkins Medical Institutions and The James Brady Buchannan Urological Institute, Baltimore, MD, USA
• To investigate pathological and short-term outcomes since the most recent Gleason system modifications by the International Society of Urological Pathology (ISUP) in an attempt to divide the current Gleason grading system into prognostically accurate Gleason grade groups.
PATIENTS AND METHODS
• We queried the Johns Hopkins Radical Prostatectomy Database (1982–2011), approved by the institutional review board, for men undergoing radical prostatectomy (RP) without a tertiary pattern since 2004 and identified 7869 men.
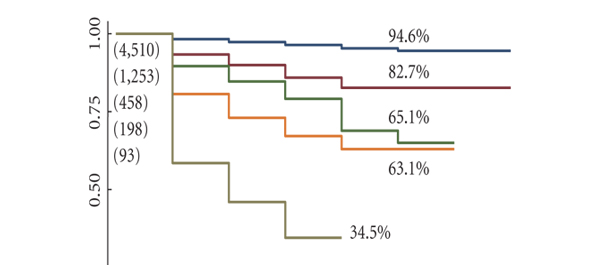
• Multivariable models were created using preoperative and postoperative variables; prognostic grade group (Gleason grade ≤6; 3 + 4; 4 + 3; 8; 9–10) was among the strongest predictors of biochemical recurrence-free (BFS) survival.
RESULTS
• Significant differences were noted among the Gleason grade groups at biopsy; differences were noted in the race, PSA level, clinical stage, number of positive cores at biopsy and the maximum percentage of positive cores among the Gleason grade groups at RP.
• With a median (range) follow-up of 2 (1–7) years, 5-year BFS rates for men with Gleason grade ≤6, 3 + 4, 4 + 3, 8 and 9–10 tumours at biopsy were 94.6, 82.7, 65.1, 63.1 and 34.5%, respectively (P < 0.001 for trend); and 96.6, 88.1, 69.7, 63.7 and 34.5%, respectively (P < 0.001), based on RP pathology.
CONCLUSIONS
• The 2005 ISUP modifications to the Gleason grading system for prostate carcinoma accurately categorize patients by pathological findings and short-term biochemical outcomes but, while retaining the essence of the Gleason system, there is a need for a change in its reporting to more closely reflect tumour behaviour.
• We propose reporting Gleason grades, including prognostic grade groups which accurately reflect prognosis as follows: Gleason score ≤6 (prognostic grade group I); Gleason score 3+4=7 (prognostic grade group II); Gleason score 4+3=7 (prognostic grade group III); Gleason score 4+4=8 (prognostic grade group (IV); and Gleason score 9–10 (prognostic grade group (V).
The ‘Gleason Grading System’ first proposed by Donald Gleason in 1966 was a revolutionary system for its time. As it advocated the use of a sum score that combined the two most common patterns of prostate cancer seen in a radical prostatectomy specimen to predict the biological outcome of the tumour, rather than the worst pattern that was in common usage with other tumour types, it was truly innovative. Furthermore, although several other classification systems for prostate cancer have been proposed since then, none has stood the test of time as well as the Gleason system and certainly no other system is in widespread use internationally.
Gleason and Mellinger went on to make adjustments and modifications to this classification system in 1974 and 1977, as the series of cases examined was expanded from the original 270 patients to >1000 patients.
Since then, there have been further changes to the Gleason Grading System with the advent of immunocytochemistry and in terms of clarification of the size and spacing of individual acini that are seen in the various patterns originally illustrated by Gleason. A tertiary pattern of prostate cancer, mentioned in passing by Gleason, has also become more clearly identified in a proportion of cases.
Possibly the most important advance regarding the Gleason Grading System was the result of an International Consensus Conference of Urological Pathologists in 2005. This meeting, comprising >80 specialist pathologists from 20 countries, published the updated or ‘Modified Gleason Grading System’. These guidelines were based on the changes in practice that had taken place in the diagnosis and treatment of prostate cancer in the previous 40 years and included evidence for the confirmation that Gleason 1 and 2 patterns should not be assigned on prostatic needle biopsy specimens and that all cribriform areas of tumour were best regarded as Gleason pattern 4 rather than Gleason pattern 3.
Although these modifications have been useful for the surgeon and pathologist, they have not clarified the Gleason grading system for the patient. It is not easy to explain or to understand why a system that in theory could produce a range of Gleason sum scores from 2 to 10, is in practice actually limited on prostatic biopsy to Gleason sum score 6 to 10. Thus, rather confusingly, Gleason 6 is the most favourable category of prostatic carcinoma in terms of prognosis, rather than indicating a ‘middle-of-the-scale’ tumour.
The paper presented in this issue of BJUI, ‘Prognostic Gleason grade grouping: data based on the modified Gleason scoring system’, attempts to compensate for this by allowing the categorisation of prostatic carcinoma not only in terms of Gleason sum score, but also into prognostic groups I to V that correlate with the sum score and may be easier for the patient to appreciate.
This is an important next step in the development of the Gleason Grading System and hopefully one that will be embraced by surgeons and pathologists and more easily accepted by patients.
Alex Freeman Department of Histopathology, University College London Hospital, London, UK
Every week the Editor-in-Chief selects the Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
The European Association of Urology Robotic Urology Section (ERUS) survey of robot-assisted radical prostatectomy (RARP)
Vincenzo Ficarra1, Peter N. Wiklund2, Charles Henry Rochat3, Prokar Dasgupta4, Benjamin J. Challacombe4, Prasanna Sooriakumaran5, Stefan Siemer6, Nazareno Suardi7, Giacomo Novara1 and Alexandre Mottrie8
1Oncological and Surgical Sciences, Urology Clinic, University of Padua, Padua, Italy; 2Urology Laboratory, Department of Molecular Medicine and Surgery, Karolinska Institutet, Stockholm, Sweden; 3Multidisciplinary Centre of Robot-Assisted Laparoscopic Surgery, Générale-Beaulieu Clinic, Geneva, Switzerland; 4Department of Urology, Guy’s Hospital, London, UK; 5Department of Urology, Royal Surrey County Hospital, Guildford, UK; 6Department of Urology, Universitätsklinikum des Saarlandes, Homburg/Saar, Germany; 7Department of Urology, Vita-Salute University San Raffaele, Milan, Italy; and 8Department of Urology O.L.V. Clinic Aalst, Aalst, Belgium; EAU Robotic Urologic Section (ERUS) Scientific Working Group
• To evaluate surgeons adherence to current clinical practice, with the available evidence, for robot-assisted radical prostatectomy (RARP) and offer a baseline assessment to measure the impact of the Pasadena recommendations. Recently, the European Association of Urology Robotic Urology Section (ERUS) supported the Pasadena Consensus Conference on best practices in RARP.
SUBJECTS AND METHODS
• This survey was performed in January 2012. A specific questionnaire was sent, by e-mail, to 145 robotic surgeons who were included in the mailing-list of ERUS members and working in different urological institutions.
• Participating surgeons were invited to answer a multiple-choice questionnaire including 24-items evaluating the main RARP surgical steps.
RESULTS
• In all, 116 (79.4%) invited surgeons answered the questionnaire and accepted to participate to the ERUS survey.
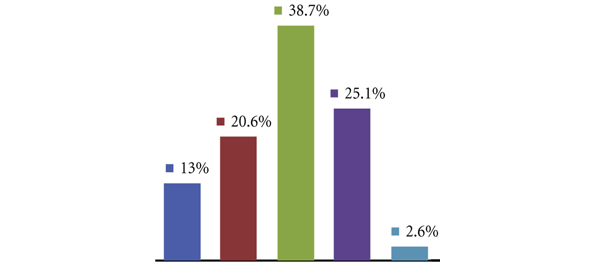
• In all, 47 (40.5%) surgeons performed >100 RARPs; 41 (35.3%) between 50 and 100, and 28 (24.1%) <50 yearly.
• The transperitoneal, antegrade technique was the preferred approach.
• Minimising bladder neck dissection and the use of athermal dissection of the neurovascular bundles (NVBs) were also popular.
• There was more heterogeneity in the use of energy for seminal vesicle dissection, the preservation of the tips of the seminal vesicle and the choice between intra- and interfascial planes during the antero-lateral dissection of the NVBs. There was also large variability in the posterior and/or anterior reconstruction steps.
CONCLUSIONS
• The present study is the first international survey evaluating surgeon preferences during RARP.
• Considering that the results were collected before the publication of the Pasadena recommendations, the data might be considered an important baseline evaluation to test the dissemination and effects of the Pasadena recommendations in subsequent years.
Robot-assisted radical prostatectomy (RARP) has become the technique of choice for clinically localised prostate cancer. However, marked inter-surgeon heterogeneity and an obvious lack of standardisation exist for the indications and technique of the procedure. In this issue of the BJUI, Ficarra et al. conducted a multinational survey seeking opinion from 145 robotic surgeons about individual practices during RARP. These opinions can be compared against the benchmark set by the Pasadena Consensus and can help gauge the impact of its recommendations.
Responses from 116 (79.4%) invited surgeons were analysed. The authors acknowledge the limited participation of non-European surgeons (17.1%), which may limit validity and application of its results at a global level. Most surgeons were in consensus with the Pasadena recommendations for transperitoneal access (88%), antegrade approach (76%) and bladder neck preservation (77%). The opinions on cautery use for the seminal vesicle/vas deferens dissection (51% athermal; 21% bipolar), athermal nerve-sparing approach (90%) and the use of the running suture technique for urethrovesical anastomosis (96.6%) were also in agreement.
Despite wide surgeon and institutional variability regarding the definition of bladder neck preservation and its role in the return of urinary continence, most preferred to preserve the bladder neck. This may pose difficulty in the interpretation of the results in view of the ambiguity about the definition and technique adopted under the term ‘bladder neck preservation’ (Eur Urol,BJU Int).
Most of the participating surgeons were using anterolateral prostatic fascia dissection (Veil of Aphrodite) towards preserving the cavernous nerves by using an athermal approach. Over the last decade the evolution of robot-assisted surgery, with excellent three-dimensional visualisation, depth perception, and EndoWrist® technology has made working in the confines of the pelvis both ubiquitous and a desired skill.
The present study found that 33% of surgeons omitted the internal iliac lymph nodes (LNs) and removed only obturator, with or without the external iliac LNs. The Pasadena Consensus recommends a template that includes the internal iliac, external iliac and obturator LNs. Mattei et al. in an attempt to map primary prostatic lymphatic ‘landing’ zones found that after performing a standard limited LN dissection (dorsal to and along the external iliac vein; medially along the obturator nerve) only 38% of LNs were removed. They recommended a template that retrieves LNs extending up to the ureteric crossing of the common iliac vessels. Meanwhile, Menon et al. evaluated the role of only internal iliac LN dissection (limited) in patients with a low probability of nodal disease (Partin table prediction 0–1%), and surprisingly found positive LNs in the internal iliac/obturator region 13.7 times more often than in the external iliac/obturator region. One of the issues that could be addressed in future surveys would be to evaluate how surgeons view and adapt to changes in the proposed LN template. The Pasadena Consensus further recommends considering performing LN dissection for the low-risk category based on the D’Amico risk stratification. The surgeon’s indications for pelvic LN dissection were not addressed in this survey.
Despite significant studies, including two randomised controlled trials (RCTs), published in the peer-reviewed literature reporting minimal advantage for early recovery of urinary continence with posterior reconstruction, a significant number of the surveyed surgeons still preferred to perform it. Responses to other questions about the posterior/anterior reconstruction also showed marked variability reflecting the controversial opinion about the value of these surgical steps.
On the other hand, future surveys should gather opinions about the role of RARP for high-risk disease, standardised evaluation of surgical complications; while addressing continence and potency status along with methods of their measurement. These topics were already addressed in the Pasadena Consensus and obtaining opinions of surgeons will further provide insight as to how surgeons adapt to the ever-changing advances in this field.
Over the last decade RARP has gained acceptance despite the absence of high-quality RCTs in robot-assisted surgery. The Pasadena Consensus was meant to meet the need for uniformity and this study educates us on how the surgeons really perform ‘in the trenches’. Until further evidence is available, surgeon experience and institutional volume will remain the main force driving the use of these surgical techniques and their outcomes.
Ahmed A. Aboumohamed and Khurshid A. Guru Department of Urology, Roswell Park Cancer Institute, Buffalo, NY, USA
We report a patient who presented following seminal vesicle-sparing radical retropubic prostatectomy with a complaint of dysorgasmia that was successfully treated with robot-assisted trans-peritoneal seminal vesiculectomy.
Abstract
We report a patient who presented following seminal vesicle-sparingradical retropubic prostatectomy with a complaint of dysorgasmia thatwas successfully treated with robot-assisted trans-peritoneal seminalvesiculectomy.
Introduction
Radical retropubic prostatectomy (RRP) is a mainstay surgical treatment for clinically localized prostate cancer. Improved anatomical understanding of prostate vasculature, sphincteric musculature and autonomic innervation in the 1980s [1] facilitated development of more sophisticated surgical techniques to improve post-operative potency [2] and urinary continence [3].
Traditional RRP involves concomitant removal of the seminal vesicles (SV) in addition to the prostate [4]. Studies assessing pathologic specimens have demonstrated that invasion of the SV is rare in patients with low-risk, clinically localized prostate cancer [5]. This finding stimulated interest in preserving the SV during RRP in an effort to avoid injury to the nearby branches of the pelvic plexus innervating the corpus cavernosa, trigone, bladder neck and posterior urethra. John and Hauri first described the anatomical concept and surgical technique of SV-sparing RP in 2000 [6]. Subsequent reports have shown improved functional outcomes of urinary continence [7] and potency [8] following SV-sparing RRP.
Despite the potential advantages of SV-sparing RP, lingering concerns remain as to the fate of the retained SV, i.e. occult tumor and adverse post-operative symptoms. One documented adverse symptom is dysorgasmia, which is the symptomatic complaint of perineal, penile or abdominal pain following orgasm, that has been reported in 14% of patients post-RRP [9]. This symptom is also present in patients with symptomatic SV cysts, benign prostate hypertrophy, chronic prostatitis, and chronic perineal pain syndrome [10,11]. Herein we present a case of a patient who presented with dysorgasmia following apparent SV-sparing RRP that was refractory to conservative treatments and was successfully treated by robotic excision of the SV remnants with prompt resolution of his symptoms.
Case Presentation
Our patient is a 56 year-old man that presented with progressively worsening perineal pain associated with sexual activity and orgasm three years following RRP performed at an outside institution for pathologic stage pT2cN0Mx Gleason 7 prostate cancer. Postoperative serum PSA has remained <0.1 ng/mL. He reported post-prostatectomy erectile dysfunction managed successfully with intracavernosal injections. Evaluation for his symptoms of dysorgasmia revealed a palpable, tender and fluctuant 3-cm mass on digital rectal examination. Cross sectional imaging with CT revealed enlarged bilateral retained SV remnants (Figure 1). Following failure of anti-inflammatory medication therapy, he subsequently underwent two transgluteal aspirations of the SV remnants. These procedures provided transient relief, but with eventual recurrence of his symptoms. The patient was counseled on therapeutic options and opted for surgical removal of the seminal vesicle remnants.
Seminal vesiculectomy was undertaken with the da Vinci robot (Intuitive Surgical Inc, Sunnyville, CA) using a 4-armed approach similar to that of transperitoneal retrovesical approach to radical prostatectomy. A standard 5-trocar configuration was used with entry into the peritoneal cavity. The vas deferentia were dissected bilaterally and traced distally towards the seminal vesicles. Anterior retraction of the vas allowed for improved exposure and dissection of each SV. Dissection of both right and left SV met with significant adhesions and fibrosis as a result of his prior radical retropubic prostatectomy. Dissection was especially challenging both anteriorly adjacent to the bladder base as well as posteriorly adjacent to the rectum. Use of the Prograsp forceps in the fourth robotic arm was critical in providing retraction and exposure of tissue planes. Both SV remnants were dissected meticulously using a combination of blunt and sharp dissection with limited use of cautery to avoid injury to adjacent structures. Lateral attachments to the SV remnants were clipped and divided.
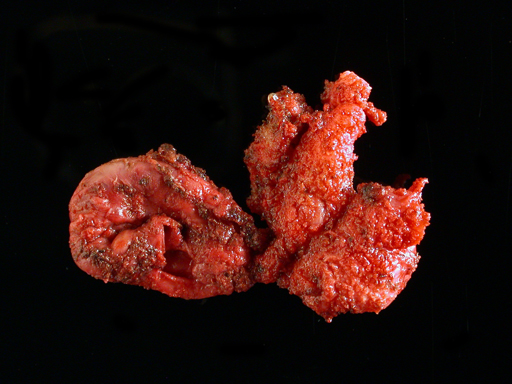
Once all attachments to the SV remnants were freed, the specimen was placed in an entrapment sack and extracted at the umbilicus at the end of the operation (Figure 2). To test the integrity of the bladder, the urethral catheter was filled with 200 mL of sterile saline with no evidence of leak. Likewise, the integrity of the rectum was assured by transrectal air insufflation while filling the pelvis with saline, which revealed no signs of perforation. A closed suction drain was left draining the retrovesical space.
Following surgery, the patient recovered well and was discharged on postoperative day one. He reported prompt cessation of his dysorgasmia symptoms at his one-month postoperative follow-up appointment and continues to remain pain free at 2.5 years follow up. He suffered no significant change in his voiding pattern and reported stable and persistent erectile dysfunction managed successfully by intracavernosal injection therapy.
Discussion
The precise mechanism for dysorgasmia due to a retained seminal vesicle remnant is still largely unknown. Multiple etiologies for dysorgasmia have been proposed, including spasm of the post-RRP vesico-urethral anastamosis [9], SV congestion secondary to ejaculatory duct obstruction [12], alteration of adrenergic receptor sensitivity causing spastic contraction13, and pudendal nerve compression by muscles contracting during intercourse [14]. The presenting symptoms and management of our patient is similar to symptomatic seminal vesicle cysts, which is a rare disorder that can be congenital or acquired [15] and often presents with complaints of dysorgasmia and perineal pain [10]. There are multiple interventions for symptomatic SV cysts, but the definitive treatment is surgical, including transrectal and transvesical aspiration, transurethral deroofing and surgical excision. While transrectal aspiration is the least invasive and is generally successful at relieving symptoms, recurrence within a few months is common [10]. Open and laparoscopic approaches to seminal vesiculectomy have both shown > 98% efficacy in eliminating SV-produced symptoms [10,16-22], but the laparoscopic procedure is associated with lower morbidity compared with the open approach. Robotic removal of a symptomatic SV cyst was previously described [23] and all subsequent cases have reported total resolution of SV symptomatology with no adverse events [24-26].
In 2005, O’Leary described a patient with symptoms of intense dysorgasmia that developed immediately after SV-sparing RRP [27]. Oral analgesics were the only option offered for pain, providing mild relief of the patient’s symptoms. Surgical removal of retained SV was not pursued in this case report because of concerns of procedure invasiveness and uncertain benefit. Our patient’s complaints were similar to the patient in the O’Leary case report, as well as to individuals with symptomatic SV cysts. As our patient experienced temporary improvement with SV aspiration, this suggested a comparable nociceptive etiology to an SV cyst and that definitive surgical management would provide relief.
Reoperative surgical excision of retained seminal vesicles can prove challenging due to dense scarring and close proximity to vital structures such as the bladder, rectum and neurovascular bundles. In our patient, a robotic approach was elected to improve visualization and facilitate dissection with the use of wristed instrumentation. Extensive scarring was noted around the retained SV remnants resulting in distortion of the anatomy, making this dissection technically challenging. The key manoeuvre during such a case is to maintain the dissection immediately along the surface of the SVs with minimal cautery and use of hemoclips to avoid inadvertent entry or thermal injury to adjacent structures such as the rectum and bladder. As the patient had pre-existing erectile dysfunction following his RP, rigorous attempts at nerve preservation were not made. In the case of a patient with good erectile function, attempts can be made to utilize hemoclips alone without use of electrocautery to minimize the risk of cavernous nerve injury. However, due to anticipated extensive inflammation and scarring present, the patient should be clearly advised on the high likelihood of worsening postoperative erectile function if surgery is pursued. The patient in our case experienced an uneventful perioperative course and reported complete resolution of his symptoms with stable erectile dysfunction.
Conclusion
This case report demonstrates that surgical removal of symptomatic retained seminal vesicles is a viable option for treatment of the rare case of dysorgasmia following SV-sparing RRP. A robotic approach provides a minimally invasive and ergonomically favorable alternative to address reoperative surgery such as in this case. The efficacy of seminal vesiculectomy for eliminating our patient’s symptoms further implicates the seminal vesicles as a prime component in the etiology of dysorgasmia. Further research is necessary to identify the precise mechanism for dysorgasmia.
Figure 1. Non-contrast CT showing apparent cystic mass outlined in red.
Figure 2. Gross specimen of seminal vesicle remnants.
References
1) Walsh PC and Donker PJ: Impotence following radical prostatectomy: insight into etiology and prevention. J Urol 1982; 128: 492.
2) Walsh PC, Lepor H, Eggleston JC. Radical prostatectomy with preservation of sexual function: anatomical and pathological considerations. Prostate. 1983;4(5):473-85.
3) O’Donnell PD, Finan BF. Continence following nerve-sparing radical prostatectomy. J Urol. 1989 Nov;142(5):1227-8; discussion 1229.
4) Reiner WG, Walsh PC. An anatomic approach to the surgical management of the dorsal vein and Santorini’s plexus during radical prostatectomy. J Urol 1979;121:198-200.
5) Zlotta AR, Roumeguère T, Ravery V, et. al.; European Society for Urological Oncology. Is seminal vesicle ablation mandatory for all patients undergoing radical prostatectomy? A multivariate analysis on 1283 patients. Eur Urol. 2004 Jul;46(1):42-9.
6) John H, Hauri D. Seminal vesicle-sparing radical prostatectomy: a novel concept to restore early urinary continence. Urology. 2000 Jun;55(6):820-4.
7) Albers P, Schäfers S, Löhmer H, de Geeter P. Seminal vesicle-sparing perineal radical prostatectomy improves early functional results in patients with low-risk prostate cancer. BJU Int. 2007 Nov;100(5):1050-4.
8) Sanda MG, Dunn R, Wei J. Seminal vesicle sparing technique is associated with improved sexual HRQOL outcome after radical prostatectomy. J Urol 2002;167:151 (A606).
9) Barnas JL, Pierpaoli S, Ladd P, et al. The prevalence and nature of orgasmic dysfunction after radical prostatectomy. BJU Int. 2004;94:603–605.
10) van den Ouden D, Blom JHM, Bangma C, de Spiegeleer AHVC. Diagnosis and Management of Seminal Vesicle Cysts Associated with Ipsilateral Renal Agenesis: A Pooled Analysis of 52 Cases. Eur Urol 1998;33:433-440.
11) Ilie CP, Mischianu DL, Pemberton RJ. Painful ejaculation. BJU Int. 2007 Jun;99(6):1335-9. Epub 2007 Apr 6.
12) Nadler RB, Rubenstein JN. Laparoscopic excision of a seminal vesicle for the chronic pelvic pain syndrome. J Urol 2001; 166: 2293–4.
13) Demyttenaere K, Huygens R. Painful ejaculation and urinary hesitancy in association with antidepressant therapy: relief with tamsulosin. Eur Neuropsychopharmacol 2002; 12: 337– 41
14) Myers RP. An anatomic approach to the pelvis in the male. In Crawford ED, Das S eds, Current Genitourinary Cancer Surgery, 2nd edn. Baltimore: Williams & Wilkins, 1997: 55–69
15) Kavoussi PK, Costabile RA. “Ch 37. Surgery of the Scrotum and Seminal Vesicle”. Campbell-Walsh Urology, 10th edition. editor Wein AJ. Philadelphia: Saunders 2012; 1115-1126.
16) McDougall EM, Clayman RV, Bowles WT. Laparoscopic excision of mullerian duct remnant. J Urol 1994;152:482–484.
17) Carmignani, G., Gallucci, M., Puppo, P, De Stefani S, Simonato A, Maffezzini M. Video laparoscopic excision of a seminal vesicle cyst associated with ipsilateral renal agenesis. J Urol 1995; 153: 437.
18) Ikari O, Castilho LN, Lucena R, D’Ancona CA, Netto NR Jr. Laparoscopic excision of seminal vesicle cysts. J Urol. 1999 Aug;162(2):498-9.
19) McDougall EM, Afane JS, Dunn MD, Shalhav AL, Clayman RV. Laparoscopic management of retrovesical cystic disease: Washington University experience and review of the literature. J Endourol 15: 815– 819, 2001.
20) Cherullo EE, Meraney AM, Bernstein LH, Einstein DM, Thomas AJ, Gill IS. Laparoscopic management of congenital seminal vesicle cysts associated with ipsilateral renal agenesis. J Urol. 2002 Mar;167(3):1263-7.
21) Moudouni SM, Tligui M, Doublet JD, et al. Laparoscopic excision of seminal vesicle cyst revealed by obstruction urinary symptoms. Int J Urol. 2006 Mar;13(3):311-4.
22) Nassir A. Symptomatic cystic seminal vesicle: a laparoscopic approach for effective treatment. Can Urol Assoc J. 2009 Dec;3(6):E81-3.
23) Carmack AJ, Siddiq FM, Leveillee RJ. Novel use of da Vinci Robotic Surgical System: removal of seminal vesicle cyst in previously dissected pelvis. Urology. 2006 Jan;67(1):199.
24) Moore CD, Erhard MJ, and Dahm P: Robot-assisted excision of seminal vesicle cyst associated with ipsilateral renal agenesis. J Endourol 21: 776-779, 2007.
25) Selli C, Cavalleri S, De Maria M, Iafrate M, Giannarini G. Robot-assisted removal of a large seminal vesicle cyst with ipsilateral renal agenesis associated with an ectopic ureter and a Müllerian cyst of the vas deferens. Urology. 2008 Jun;71(6):1226.e5-7. Epub 2008 Feb 21.
26) Hong YK, Onal B, Diamond DA, Retik AB, Cendron M, Nguyen HT. Robot-assisted laparoscopic excision of symptomatic retrovesical cysts in boys and young adults. J Urol. 2011 Dec;186(6):2372-8. Epub 2011 Oct 20.
27) O’Leary MP. Orgasmic Pain and a Detectable PSA Level after Radical Prostatectomy. Rev Urol. 2005 Fall; 7(4): 240–241.
A recent editorial in the BMJ by Christopher Parker (Treating prostate cancer. BMJ 2012; 345: e5122)uses the “best available evidence” from the PIVOT study (Wilt TJ, et al) to argue the case for watchful waiting for low risk prostate cancer and question the need to diagnose the condition at all. Unfortunately the PIVOT trial was marred by a number of serious flaws that should make us doubt its conclusions.
The original design of the PIVOT trial included a randomisation of 2000 patients to surgery or observation (Prostate cancer, uncertainty and a way forward. NEJM 2012; 367: 270-1). Unfortunately, this goal was not achieved; the design was modified to justify a randomization goal of only 740 patients. Median survival was assumed to be 15 years in the original study design and 10 years in the updated version. If the median survival of 12 years in the study’s observation group is taken and 7 years for enrollment and 8 years of follow-up assumed, the sample requires 1200 patients in order to detect a 25% relative reduction in mortality with 90% power and a two-sided alpha level of 0.05. With an actual enrollment of only 731 patients, the study was consequently underpowered to detect this relatively large clinical effect. The wide 95% confidence interval around the hazard ratio for death in the treatment group illustrates this point. A relative increase of 8% to a relative reduction of 29% in the risk of death in the prostatectomy group, as compared with the observation group, cannot be excluded with 95% confidence. Only 15% of the deaths were attributed to prostate cancer or its treatment.
Although a “life expectancy of at least 10 years” was an entry criterion, by 10 years almost half the participants had died, leaving only 176 men in the surgery group and 187 in the observation cohort, and by 15 years only 30% were alive. The investigators therefore did not recruit healthy men who would be the normal candidates for surgery and randomize them to observation; instead they recruited elderly and co-morbid men with very limited life expectancy and randomised them to surgery (with one fatality!). Furthermore, the finding that one fifth of patients did not adhere to the assigned treatment further reduces the ability of the trial to discern a treatment effect.
Prostate cancer is a slowly progressive condition which eventually, and after many years, results in a painful death from metastases in a significant number of patients, unless mortality from other causes supervenes. Radical prostatectomy, now usually performed minimally invasively with robotic assistance (Goldstraw MA, et al), prevents disease progression in >80% of well-selected cases. We appear to manage localised prostate cancer in a much more holistic way than our American colleagues and MDT decision-making and robust active surveillance programmes have enhanced this. Others were also outraged by the Parker editorial and the intrinsically flawed results of the PIVOT study should definitely not encourage us to turn our backs on a disease that kills more than 10,000 men per annum in the UK and hundreds of thousands more worldwide.
Roger Kirby, Ben Challacombe and Prokar Dasgupta The Prostate Centre, London W1G 8GT and Guy’s Hospital, King’s College London, King’s Health Partners
Every week the Editor-in-Chief selects the Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
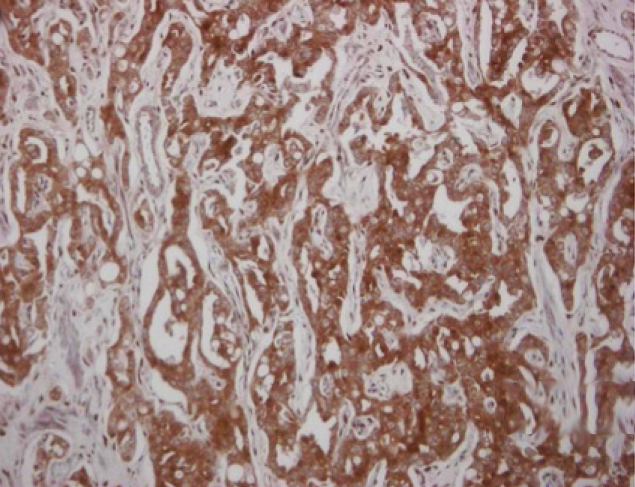
Expression patterns of epithelial–mesenchymal transition markers in localized prostate cancer: significance in clinicopathological outcomes following radical prostatectomy
Hosny M. Behnsawy, Hideaki Miyake, Ken-Ichi Harada and Masato Fujisawa
• To analyse the expression patterns of multiple molecular markers implicated in epithelial–mesenchymal transition (EMT) in localized prostate cancer (PC), in order to clarify the significance of these markers in patients undergoing radical prostatectomy (RP).
PATIENTS AND METHODS
• Expression levels of 13 EMT markers, namely E-cadherin, N-cadherin, b-catenin, g-catenin, fibronectin, matrix metalloproteinase (MMP) 2, MMP-9, Slug, Snail, Twist, vimentin, ZEB1 and ZEB2, in RP specimens from 197 consecutive patients with localized PC were evaluated by immunohistochemical staining.
RESULTS
• Of the 13 markers, expression levels of E-cadherin, Snail, Twist and vimentin were closely associated with several conventional prognostic factors.
• Univariate analysis identified these four EMT markers as significant predictors for biochemical recurrence (BR), while serum prostate-specific antigen, Gleason score, seminal vesicle invasion (SVI), surgical margin status (SMS) and tumour volume were also significant.
• Of these significant factors, expression levels of Twist and vimentin, SVI and SMS appeared to be independently related to BR on multivariate analysis
• There were significant differences in BR-free survival according to positive numbers of these four independent factors. That is, BR occurred in four of 90 patients who were negative for risk factors (4.4%), 21 of 83 positive for one or two risk factors (25.3%) and 19 of 24 positive for three or four risk factors (79.2%).
CONCLUSION
• Measurement of expression levels of potential EMT markers, particularly Twist and vimentin, in RP specimens, in addition to conventional prognostic parameters, would contribute to the accurate prediction of the biochemical outcome in patients with localized PC following RP.