
Posts

Article of the week: 68Ga‐PSMA PET/CT predicts complete biochemical response from RP and lymph node dissection in intermediate‐ and high‐risk PCa
Every week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an editorial written by a prominent member of the urological community. These are intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this month, it should be this one.
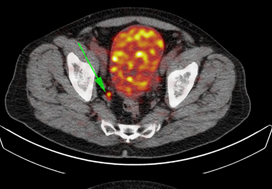
Gallium‐68‐prostate‐specific membrane antigen (68Ga‐PSMA) positron emission tomography (PET)/computed tomography (CT) predicts complete biochemical response from radical prostatectomy and lymph node dissection in intermediate‐ and high‐risk prostate cancer
Pim J. van Leeuwen*, Maarten Donswijk†, Rohan Nandurkar‡, Phillip Stricker§¶, Bao Ho**, Stijn Heijmink††, Esther M.K. Wit*, Corinne Tillier*, Erik van Muilenkom*, Quoc Nguyen§, Henk G. van der Poel* and Louise Emmett‡§**
*Department of Urology, †Department of Nuclear Medicine, The Netherlands Cancer Institute, Amsterdam, The Netherlands, ‡Faculty of Medicine, University of New South Wales Sydney, §The Australian Prostate Cancer Research Centre-NSW, The Garvan Institute of Medical Research, ¶St Vincent’s Clinic, **Department of Theranostics and Nuclear Medicine, St Vincent’s Hospital Sydney, Sydney, New South Wales, Australia and ††Department of Radiology, The Netherlands Cancer Institute, Amsterdam, The Netherlands
Abstract
Objective
To determine the value of gallium‐68‐prostate‐specific membrane antigen (68Ga‐PSMA)‐11 positron emission tomography (PET) /computed tomography (CT) in men with newly diagnosed prostate cancer.
Patients and methods
We analysed results of 140 men with intermediate‐ and high‐risk prostate cancer. All men underwent 68Ga‐PSMA‐11 PET/CT and multiparametric magnetic resonance imaging (mpMRI) before radical prostatectomy (RP) with extended pelvic lymph node (LN) dissection. For each patient, the clinical and pathological features were recorded. Prostate‐specific antigen (PSA) was documented at staging scan, and after RP, at a median (interquartile range) of 110 (49–132) days. A PSA level of ≥0.03 ng/mL was classified as biochemical persistence (BCP). Logistic regression was performed for association of clinical variables and BCP.
Results
In these 140 patients with intermediate‐ and high‐risk prostate cancer, 27.1% had PSMA PET/CT‐positive findings in the pelvic LNs. Sensitivity and specificity for detection of LN metastases were 53% and 88% (PSMA PET/CT) and 14% and 99% (mpMRI), respectively. The overall BCP rate was 25.7%. The BCP rate was 16.7% in men who were PSMA PET/CT LN‐negative compared to 50% in men who were PSMA PET/CT LN‐positive (P < 0.05). The presence of PSMA‐positive pelvic LNs was more predictive of BCP after RP than cT‐stage, PSA level, and the Gleason score, adjusted for surgical margins status.
Conclusions
68Ga‐PSMA‐11 PET/CT is highly predictive of BCP after RP, and should play an important role informing men with intermediate‐ or high‐risk prostate cancer.

PSMA at the cutting edge of prostate cancer treatment: Report from a PSMA Symposium convened at The University of Oxford
The potential of PSMA
While molecular imaging is not exactly a new technology (TIME Magazine named PET-CT as the medical invention of the year back in 2000), recent developments in radio-pharmacy have positioned the field at the forefront of innovations in cancer imaging and, tantalisingly, novel therapeutic approaches to cancer treatment.
Urologists have typically been forward thinking and innovative, and have been quick to acknowledge the value of molecular imaging as a tool to enhance the accuracy of the diagnostic process and improve patient outcomes. The recent development of radiotracers directed against prostate-specific-membrane-antigen (PSMA) has taken things to a new level; there is now a solid body of evidence for the performance of 68Ga-PSMA PET/CT in primary and secondary staging, with an ability to accurately detect small volume disease at far lower serum PSA levels – the use of 68Ga-PSMA PET/CT as a diagnostic adjunct is becoming increasingly mainstream in continental Europe and Australia.
Oxford PSMA Symposium 2018
It is in this context that, on 22 November 2018, the Nuffield Department of Surgical Sciences in Oxford hosted a symposium at the Old Road Campus Research Building focused on the utility of PSMA-related technologies. The symposium attracted an impressive array of attendees from across the UK, Europe and Australia.
The symposium was opened with comments by Professor Freddie Hamdy of Oxford, who welcomed all attendees and speakers, some of whom who had travelled more than 10,000 miles to attend the gathering.
Liberal use of PSMA-PET down under
The first speaker, Professor Declan Murphy, from Melbourne’s Peter MacCallum Cancer Centre, shared comprehensive data and experience from Victoria in Australia, where access to 68Ga-PSMA PET/CT is seemingly unrestricted. Professor Murphy delivered a fascinating talk, expounding the gamut of PSMA PET applications in prostate cancer, from primary staging (promising data), to biochemical recurrence (there is definite evidence that PSMA PET accurately detects early recurrence and can guide salvage treatment options), right through to therapeutic uses of PSMA. In particular, he discussed the use of Lutetium-177 (177Lu)-PSMA-617 (LuPSMA) as a treatment in men with CRPC, presenting the findings of their recent Lancet Oncology study led by Michael Hoffman. Although still in the early stages, the data here look very exciting and hale a potential revolution in the way we manage high risk and advanced prostate cancer.
How easy is it to set up a PSMA imaging service in the UK?
The next speaker was Professor Jamshed Bomanji from the Institute of Nuclear Medicine, University College London (UCL), who presented an eye-opening talk that focussed on the challenges of setting up a PSMA-PET service within an NHS Trust in England. The effort he and his team put into developing their service in the face of significant practical resistance has been frankly heroic. Pleasingly, these efforts have been worthwhile as the team from UCL have clearly demonstrated that PSMA PET/CT has had a significant impact on the management of men with biochemical recurrence with the team contributing to guidelines drawn up to standardise use, keeping similar standards of testing as https://www.blinkhealth.com/zoloft. It is very disappointing that NHS England saw fit to withdraw funding for the gallium tracer required for PSMA-PET scanning in August 2018. This does seem rather short-sighted given the clear evidence favouring the utility of PSMA-PET over other modalities such as FDG or Choline-PET, both of which are still funded. All in all, Professor Bomanji’s talk was a sobering examination of the challenges we face in our commitment to delivering cutting edge, world-class cancer services whilst at the same time considering the financial implications to the NHS of providing such high-end services.
Associate Professor Bart Cornelissen along with Dr Rebekka Hueting who runs PROx (PET Radiopharmacy Oxford) presented their intentions for 68Ga-PSMA-PET imaging in Oxford, and the University’s imminent plan to install a cyclotron on site that will allow PET imaging with locally generated radioisotopes to increase dose efficiency – the half-life of gallium means that any requirement to transport the dose reduces the number of scans that can be performed at destination. This is particularly important given some recent negative press coverage.
Surgery for men with metastases?
Prasanna Sooriakumaran (PS) of University College London Hospital (UCLH) Department of Urology discussed the TRoMbone Study, a UK feasibility RCT that he has set up aimed at testing radical prostatectomy in men with oligometastatic prostate cancer. This interesting study promises to tease out the possible benefits of radical prostatectomy to men with low-volume metastatic disease. There are examples in other cancers whereby aggressive management of the primary tumour confers survival benefits in patients with low-burden metastatic disease and it is not unreasonable to think this may be the case for prostate cancer. Recruitment to such trials of ‘oligometastatic’ disease is contingent upon definitions of ‘low-volume’ disease, and accurate detection of such disease. PSMA-PET imaging is positively helping with this paradigm with its far superior sensitivity to conventional cross-sectional staging.
PSMA as a tool to improve surgery
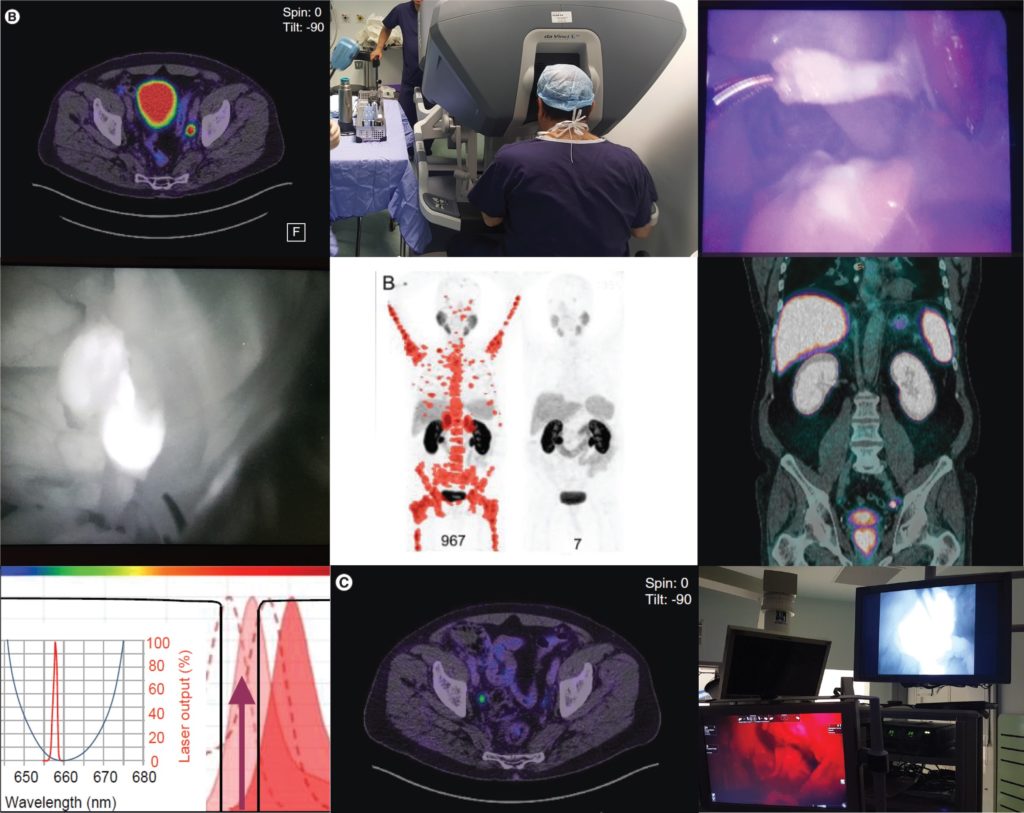
Pim van Leeuwen of the Netherlands Cancer Institute delivered an engaging talk entitled “PSMA intra-operative enhancement of lymph node dissection”, accompanied by some excellent video demonstrations. Next up were Boris Vojnovic and Alastair Lamb of Oxford who discussed fluorescence optics and intra-operative use of PSMA as part of the on-going ProMOTE study (Prostate Molecular Targeting to Enhance Surgery). We wish the investigators good luck as the study progresses and we eagerly look forward to seeing the data as they emerge.
Summary
In summary, the Oxford PSMA symposium 2018 brought together clinicians from around the globe who share a common enthusiasm for PSMA-related technologies that promise to revolutionise prostate cancer management in the near future. Common themes included the use of PSMA in staging, therapeutics and intra-operative guidance. The message from our overseas guests, both European and Antipodean, was that PSMA-based imaging is increasingly part of routine care in the management of prostate cancer and definite benefits are seen, particularly in regard to accurate staging and identification of very early recurrence. While we in the UK are a little behind the curve when it comes to adoption of this increasingly established technology, we are hopeful of increasing the use of this technology in the NHS in order to rationalise appropriate treatment, reduce futile expenditure and ensure gold-standard management of men with prostate cancer.

Conference dinner at Balliol College, Oxford, UK
From Left: Alastair Lamb (Oxford), Declan Murphy (Melbourne), Freddie Hamdy (Oxford), Boris Vojnovic (Oxford), Prasanna Sooriakumaran (UCLH), Richard Bryant (Oxford), Ben Lamb (Cambridge)
Aaron Leiblich, Clinical Lecturer, Nuffield Department of Surgical Sciences;
Alastair Lamb, Consultant Urologist, Churchill Hospital Cancer Centre; on behalf of the meeting faculty
Alastair Lamb is a Cancer Research UK Clinician Scientist, Senior Fellow in Robotic Surgery & Honorary Consultant Urologist at the Nuffield Department of Surgery, University of Oxford, and Oxford University Hospitals NHS Foundation Trust. Alastair is interested in delivering excellent and timely prostate cancer care, focussing on state-of-the-art diagnostics with multiparametric MRI and targeted transperineal biopsies, followed by robotic-radical prostatectomy (RARP) or active surveillance. He also has an interest in novel molecular imaging techniques such as 68Ga-PSMA PET/CT and their use in disease stratification and selection of patients for surgery. Alastair is a local investigator for the ProMOTE, PART and TRoMbone studies.
Twitter: @lambalastair
Article of the Week: Impact of 68Ga-PSMA PET/CT in PCa with rising PSA
Every Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Clinical impact of 68Ga-prostate-specific membrane antigen (PSMA) positron emission tomography/computed tomography (PET/CT) in patients with prostate cancer with rising prostate-specific antigen after treatment with curative intent: preliminary analysis of a multidisciplinary approach
*, †, *, *, *, ‡, *, *, §, *, ‡, ¶, † and Roland van Velthoven*
Departments of *Urology, †Nuclear Medicine, ‡Oncology, §Radiation Oncology, and ¶Pathology, Institut Jules Bordet, Universite Libre de Bruxelles, Brussels, Belgium
How to Cite
Albisinni, S., Artigas, C., Aoun, F., Biaou, I., Grosman, J., Gil, T., Hawaux, E., Limani, K., Otte, F.-X., Peltier, A., Sideris, S., Sirtaine, N., Flamen, P. and van Velthoven, R. (2017), Clinical impact of 68Ga-prostate-specific membrane antigen (PSMA) positron emission tomography/computed tomography (PET/CT) in patients with prostate cancer with rising prostate-specific antigen after treatment with curative intent: preliminary analysis of a multidisciplinary approach. BJU International, 120: 197–203. doi: 10.1111/bju.13739
Abstract
Objective
To assess the impact of a novel molecular imaging technique, 68Ga-(HBED-CC)-prostate-specific membrane antigen (PSMA) positron emission tomography/computed tomography (PET/CT), in the clinical management of patients with prostate cancer with rising prostate-specific antigen (PSA) after treatment with curative intent.
Patients and Methods
In all, 131 consecutive patients were referred to our centre for a 68Ga-PSMA PET/CT in the setting of recurring prostate cancer. Of these patients, 11/131(8%) presented with persistent PSA after radical prostatectomy, while 120/131 (92%) were referred for biochemical recurrence after surgery, radiotherapy or both. The images where taken 1 h after injection of 2 MBq/kg of the 68Ga-(HBED-CC)-PSMA ligand. All examinations were interpreted by two experienced nuclear medicine specialists. Using the results of the examination, a multidisciplinary oncology committee (MOC) reported on the treatment strategy. A positive impact on clinical management was considered if the examination determined a modification in the treatment strategy compared to the MOC decision before PSMA imaging.
Results
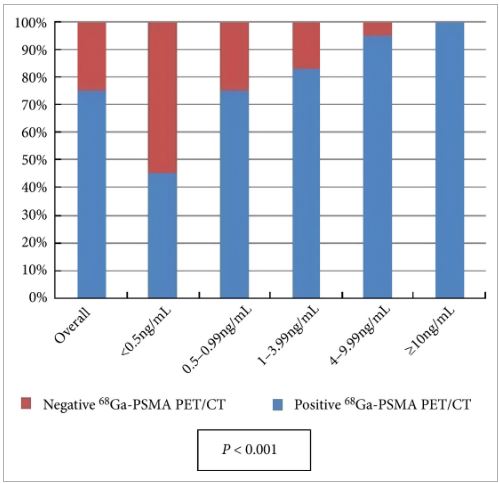
All patients completed the examination with no adverse reactions. The median (interquartile range) PSA level at the time of the examination was 2.2 (0.72–6.7) ng/mL. Overall, 68Ga-PSMA PET/CT detected at least one lesion suspicious for prostate cancer in 98/131 (75%) patients. There was an impact on subsequent management in 99/131 patients (76%). The main modifications included continuing surveillance (withholding hormonal therapy), hormonal manipulations, stereotaxic radiotherapy, salvage radiotherapy, salvage node dissection or salvage local treatment (prostatectomy, high-intensity focussed ultrasound).
Conclusion
Our preliminary experience suggests that performing 68Ga-PSMA PET/CT in patients with prostate cancer with rising PSA after treatment with curative intent can be clinically useful as it changes the treatment strategy in a significant proportion of patients. However, larger prospective trials are needed to validate our present findings.
Editorial: Defining the clinical utility of PSMA-targeted PET imaging of prostate cancer
In the field of oncology, positron emission tomography (PET) is most commonly performed using 2-deoxy-2-[18F]fluoro-d-glucose (18F-FDG), a radiofluorinated glucose analogue that accumulates in cells undergoing aerobic glycolysis. Unfortunately, because of the low glycolytic activity of hormone-naïve prostate cancer cells, 18F-FDG PET has been of little value in imaging men with this malignancy [1]. Instead, clinicians have been left to rely mostly on 99mTc-methylene diphosphonate bone scan, CT, and MRI to stage and follow patients. Recently, however, the development of multiple urea-based small molecules targeting the type II transmembrane glycoprotein prostate-specific membrane antigen (PSMA) has allowed for the highly sensitive and specific detection of prostate cancer using PET imaging [2]. To date, the majority of clinical data with PSMA-targeted PET have been generated with the 68Ga-PSMA-11 radiotracer (also known as 68Ga-PSMA-HBED-CC). Notably, studies evaluating PSMA-targeted PET have mostly focused on establishing the diagnostic performance characteristics of the various radiotracers (e.g. sensitivity and specificity), with relatively few reports exploring the clinical impact or utility of this form of molecular imaging.
In this month’s edition of BJUI, Albisinni et al. [3] aimed to look beyond the performance characteristics of 68Ga-PSMA-11 PET/CT and retrospectively analysed the impact of this imaging test on the management of 131 men with a persistently elevated PSA level or biochemical recurrence after local treatment of their prostate cancer with curative intent. Of these patients, 106 (81%) had undergone a previous radical prostatectomy. The authors defined clinical utility as any imaging finding (or lack thereof) leading to a change in a patient’s pre-PET treatment plan. In total, 68Ga-PSMA-11 PET/CT demonstrated clinical utility in 76% of imaged patients. Most commonly, the results of this imaging test led to avoidance of androgen deprivation therapy (44% of all patients imaged) in place of an alternative management strategy, such as surveillance or salvage radiation therapy. Another notable finding was that among men who had planned to undergo salvage radiation therapy prior to 68Ga-PSMA-11 PET/CT, the majority (19 of 32 [59%]) were managed with an alternative approach after undergoing imaging.
Albisinni et al. [3] are not alone in their observations regarding the high clinical utility of 68Ga-PSMA-11 PET. For example, van Leeuwen et al. [4] previously reported that nearly 30% of men who were felt to be candidates for post-prostatectomy salvage radiation therapy had findings on 68Ga-PSMA-11 PET/CT that led to a major change in management. Additionally, Sterzing et al. [5] found that approximately 50% of patients undergoing radiation therapy planning for primary or recurrent prostate cancer experienced a change to their treatment concept after imaging with 68Ga-PSMA-11 PET/CT. Combined, these data suggest that a substantial proportion of men with prostate cancer stand to have their management altered by undergoing PSMA-targeted PET imaging.
While encouraging, the study by Albisinni et al. is somewhat limited by its retrospective design [3]. An outstanding example of how data on the clinical utility of an imaging test can be prospectively collected comes to us from the National Oncology PET Registry (NOPR) in the USA. Working in collaboration with the Centers for Medicare and Medicaid Services (CMS), NOPR was established to assess the question of clinical utility related to 18F-FDG PET/CT. To measure clinical utility, NOPR required physicians to complete questionnaires assessing the indication for imaging as well as pre- and post-PET treatment plans. In a 2008 study from NOPR incorporating data from 40 863 18F-FDG studies performed at 1368 centres, it was reported that 38% of patients experienced a change in intended management as a result of this imaging test [6]. In light of these and other data from NOPR, 18F-FDG PET/CT is now widely used across a range of tumour histologies. Moreover, this imaging study is readily reimbursed by both the CMS and private insurers.
In summary, we are delighted by the results of Albisinni et al. [3] and look forward to other prospective studies (for example ClinicalTrials.gov identifier NCT02825875) that aim to define the clinical utility of PSMA-targeted PET imaging of prostate cancer.
,* , † * and †
*The James Buchanan Brady Urological Institute and Department of Urology, and †Russell H. Morgan Department of Radiology and Radiological Science, Johns Hopkins University School of Medicine, Baltimore, MD, USA
References
1 Gorin MA, Rowe SP, Denmeade SR. Clinical applications of molecular imaging in the management of prostate cancer. PET Clin 2017; doi: 10.1016/j.cpet.2016.11.001
2 Rowe SP, Gorin MA, Allaf ME et al. PET imaging of prostate-specific membrane antigen in prostate cancer: current state of the art and future challenges. Prostate Cancer Prostatic Dis 2016; 19: 223–30
3 Albisinni S, Artigas C, Aoun F et al. Clinical impact of 68Ga-prostate-specific membrane antigen (PSMA) positron emission tomography/computed tomography (PET/CT) in patients with prostate cancer with rising prostate-specific antigen after treatment with curative intent:preliminary analysis of a multidisciplinary approach. BJU Int 2017; 120: 197–203
4 van Leeuwen PJ, Stricker P, Hruby G et al. 68Ga-PSMA has a high detection rate of prostate cancer recurrence outside the prostatic fossa in patients being considered for salvage radiation treatment. BJU Int 2016; 117: 732–9
5 Sterzing F, Kratochwil C, Fiedler H et al. 68Ga-PSMA-11 PET/CT: a new technique with high potential for the radiotherapeutic management of prostate cancer patients. Eur J Nucl Med Mol Imaging 2016; 43: 34–41
6 Hillner BE, Siegel BA, Shields AF et al. Relationship between cancer type and impact of PET and PET/CT on intended management: findings of the national oncologic PET registry. J Nucl Med 2008; 49: 1928–35
Video: Value of 111In-PSMA-RGS for salvage lymphadenectomy in recurrent PCa
Value of 111In-prostate-specific membrane antigen (PSMA)-radioguided surgery for salvage lymphadenectomy in recurrent prostate cancer: correlation with histopathology and clinical follow-up
Abstract
Objectives
To evaluate the use of 111In-labelled prostate-specific membrane antigen (PSMA)-I&T-based radioguided surgery (111In-PSMA-RGS) for salvage surgery in recurrent prostate cancer (PCa) using comparison of intra-operative gamma probe measurements with histopathological results of dissected specimens. In addition, to determine the success of 111In-PSMA-RGS with regard to postoperative prostate-specific antigen (PSA) responses, PCa-specific treatment-free survival rates and postoperative complication rates.
Patients and Methods
A total of 31 consecutive patients with localized recurrent PCa undergoing salvage surgery with PSMA-targeted radioguided surgery using a 111In-labelled PSMA ligand between April 2014 and July 2015 were retrospectively included in this study. The preoperative (interquartile range; range) median PSA level was 1.3 (0.57–2.53 ng/mL; 0.2–13.9 ng/mL). Results of ex vivo radioactivity rating (positive vs negative) of resected tissue specimens were compared with findings of postoperative histological analysis. Best PSA response without additional treatment was determined after 111In-PSMA-RGS, and salvage-surgery-related postoperative complications and PCa-specific additional treatments were recorded.
Results
In 30/31 patients, 111In-PSMA-RGS allowed intra-operative identification of metastatic lesions. In total, 145 surgical specimens were removed and 51 showed metastatic involvement at histological analysis. According to 111In-PSMA-RGS ex vivo measurements, 48 specimens were correctly classified as metastatic and 87 as cancer-free, four were false-negative and six were false-positive compared with histological evaluation. Follow-up information was available for 30/31 patients. PSA declines of >50% and >90% were observed in 23/30 patients and in 16/30 patients, respectively. In 18/30 patients, a PSA decline to <0.2 ng/mL was observed. In 10/30 patients further PCa-specific treatment was given after a median (range) of 125 (48–454) days post-111In-PSMA-RGS. The remaining 20 patients remained treatment-free at a median (range) follow-up of 337 (81–591) days. Of 30 patients, 10 presented with surgery-related complications (Clavien–Dindo grade 1, n = 6, Clavien–Dindo grade 3b, n = 4).
Conclusion
111In-PSMA-RGS proved to be of high value for intra-operative detection of even small metastatic lesions in patients with PCa scheduled for salvage lymphadenectomy. It allows the exact localization and resection of metastatic tissue during 111In-PSMA-RGS and is therefore anticipated to have a beneficial influence on further disease progression; however, identification of suitable patients on the basis of PSMA-positron-emission tomography imaging as well as clinical variables is essential for satisfactory results to be obtained.