This is the final Article of the Week selected by the outgoing Editor-in-Chief from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
If you only have time to read one article this week, we recommend this one.
Enrico Checcucci*, Sabrina De Cillis*, Angela Pecoraro*, Dario Peretti*, Gabriele Volpi*, Daniele Amparore*, Federico Piramide*, Alberto Piana*, Matteo Manfredi*, Cristian Fiori*, Riccardo Autorino†, Prokar Dasgupta‡, Francesco Porpiglia* and on behalf of the Uro-technology and SoMe Working Group of the Young Academic Urologists Working Party of the European Association of Urology
*Department of Urology, San Luigi Gonzaga Hospital, University of Turin, Turin, Italy, †Division of Urology, VCU Health, Richmond, VA, USA, and ‡King’s College London, Guy’s Hospital, London, UK
To summarize the clinical experiences with single‐port (SP) robot‐assisted radical prostatectomy (RARP) reported in the literature and to describe the peri‐operative and short‐term outcomes of this procedure.
Material and Methods
A systematic review of the literature was performed in December 2019 using Medline (via PubMed), Embase (via Ovid), Cochrane databases, Scopus and Web of Science (PROSPERO registry number 164129). All studies that reported intra‐ and peri‐operative data on SP‐RARP were included. Cadaveric series and perineal or partial prostatectomy series were excluded.
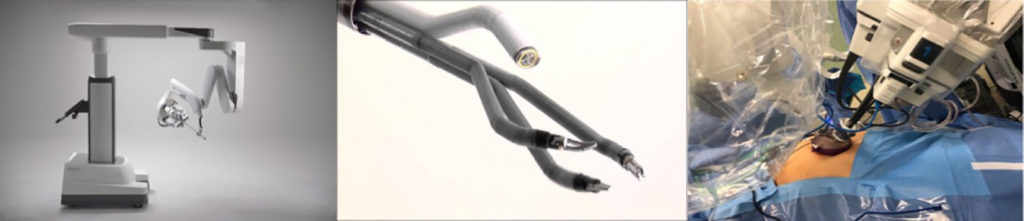
The da Vinci SP robotic platform
Results
The pooled mean operating time, estimated blood loss, length of hospital stay and catheterization time were 190.55 min, 198.4 mL, 1.86 days and 8.21 days, respectively. The pooled mean number of lymph nodes removed was 8.33, and the pooled rate of positive surgical margins was 33%. The pooled minor complication rate was 15%. Only one urinary leakage and one major complication (transient ischaemic attack) were recorded. Regarding functional outcomes, pooled continence and potency rates at 12 weeks were 55% and 42%, respectively.
Conclusions
The present analysis confirms that SP‐RARP is safe and feasible. This novel robotic platform resulted in similar intra‐operative and peri‐operative outcomes to those obtained with the standard multiport da Vinci system. The advantages of single incision can be translated into a preservation of the patient’s body image and self‐esteem and cosmesis, which have a great impact on a patient’s quality of life.
It is generally agreed upon that an extended pelvic lymph‐node dissection (ePLND) provides valuable staging information and helps guide adjuvant therapy, and thus should be undertaken in prostate cancer patients with aggressive preoperative disease features at the time of radical prostatectomy [1,2]. However, whether it has a ‘direct’ therapeutic benefit in the aforesaid patients has remained difficult to demonstrate [3]. The only patients that seem to derive a survival advantage from an ePLND are patients with pN1 disease [4] – this cited study suggested a direct therapeutic effect of an ePLND, with a 7% incremental benefit in 10‐year cancer‐specific survival per every additional LN removed (P = 0.02). However, it did not identify these patients preoperatively.
Given the significant side‐effects associated with an ePLND [3], it is worth asking the questions: which patients, identified preoperatively, may derive a direct therapeutic benefit from an ePLND, and who benefit indirectly only (i.e. via optimal utilisation of adjuvant therapies). The latter question has been answered [5,6]. Here, we try to answer the former.
We relied on the National Cancer Database (NCDB) to answer our question. The NCDB, a joint programme of the Commission on Cancer and the American Cancer Society, is a nationwide cancer database that contains information on ~70% of newly diagnosed tumours in the USA. We identified all patients with prostate cancer undergoing radical prostatectomy between the years 2004 and 2015. After excluding patients with clinical LN/metastatic disease (n = 2568), neoadjuvant radiotherapy, chemotherapy or hormonal therapy (n = 10 931), missing information on biopsy Gleason score, cT stage or preoperative PSA value (n = 166 696), and missing information regarding PLND (n = 95 348), a final sample of 311 061 patients was achieved. All available baseline patient/tumour characteristics and overall survival (OS) data (outcome) were noted. Preoperative LN invasion (LNI) risk was calculated using the Godoy nomogram. We used this nomogram as it was developed using the PLND data from North American men, and has been validated in them [6]. The cut‐off of ≥10 LNs to define an ePLND was based on prior studies [5,6,7,8]. To analyse the impact of ePLND (≥10 LNs) vs none/limited PLND (0–9 LNs) on 10‐year OS, interaction between Godoy nomogram predicted LNI probability, which is based on the preoperative PSA value, clinical stage and biopsy Gleason grade, and ePLND/PLND was plotted using locally weighted methods controlling for age, comorbidities and adjuvant radiation therapy (aRT). This was called model 1 (M1). In a second model (M2), in addition to controlling for age, comorbidities and aRT, we also adjusted for receipt of adjuvant hormonal therapy (aHT). We performed this analysis as we reasoned that a survival benefit in patients undergoing an ePLND may be due to better staging and receipt of aHT. All analyses were performed with the Statistical Analysis System (SAS), version 9.4 (SAS Institute, Cary, NC, USA), with a two‐sided P < 0.05 considered as statistically significant. An Institutional Review Board waiver was obtained prior to conducting this study, in accordance with institutional regulations on dealing with de‐identified administrative data.
Table S1 provides baseline characteristics. Of the 311 061 patients, 49 470 (15.9%) patients underwent an ePLND. The median number of LNs removed in patients undergoing none/limited PLND vs ePLND were 2 and 14, respectively (P < 0.001). The median age and preoperative PSA values for the groups were 61 and 62 years (P < 0.001) and 5.5 and 6 ng/mL (P < 0.001), respectively. Patients undergoing an ePLND had more aggressive disease on pathological analysis: Gleason ≥8 disease (17.3% vs 10.0%), pT3+ stage (37.4% vs 21.9%) and pN1 disease (8.6% vs 1.5%; P < 0.001 for all). These patients also received aRT (3.9% vs 3.1%) and aHT (4.3% vs 1.9%) more frequently than patients undergoing none/limited PLND (P < 0.001 for both).
The median (interquartile range) follow‐up for the ePLND and none/limited PLND groups was 54.0 (31.3–79.9) and 57.5 (35.1–82.0) months, respectively. In interaction analyses, the lines for ePLND and none/limited PLND separated at Godoy nomogram predicted LNI risk of 20% in model M1 (Fig. 1a), indicating that patients with a preoperative LNI risk >20% derived an OS benefit from an ePLND. This finding remained preserved in model M2, which adjusted for receipt of aHT, in addition to age, comorbidities and aRT, thus indicating a ‘direct’ independent benefit of an ePLND on OS in patients with a LNI risk of >20% (Fig. 1b).
Fig. 1. The 10‐year OS rates plotted against preoperative Godoy nomogram predicted LNI risk, stratified by ePLND vs none/limited PLND (red line indicates ePLND and blue line indicates none/limited PLND); (a ) represents model M1 (adjusting for age, comorbidities, and aRT), (b ) represents model M2 (adjusting for age, comorbidities, aRT, and aHT).
In Cox regression analyses, the first model (M1) demonstrated that patients undergoing an ePLND (hazard ratio [HR] 1.20, 95% CI 1.17–1.24) had a 9% incrementally lower hazard of 10‐year mortality than patients undergoing none/limited PLND (HR 1.29, 95% CI 1.26–1.31) for every 10% increment in Godoy nomogram predicted LNI risk, beyond the 20% cut‐off (P < 0.001). Similarly, the second model (M2) demonstrated that patients undergoing an ePLND (HR 1.18, 95% CI 1.14–1.21) had a 6% incrementally lower hazard of 10‐year mortality than patients undergoing none/limited PLND (HR 1.24, 95% CI 1.23–1.26) for every 10% increment in Godoy nomogram predicted LNI risk, beyond the 20% cut‐off (P < 0.001). This lower but preserved incremental improvement in OS after adjustment for aHT (model M2) supports our hypothesis that an ePLND is in itself a ‘direct’ independent factor in OS in patients at high‐risk of LNI.
The current American and European urological societal guidelines recommend performing an ePLND in high‐risk and unfavourable intermediate‐risk patients, especially when the estimated risk for LNI is >5% [1, 2]. However, at this cut‐off, the benefit is mainly that of accurate staging and subsequent optimal adjuvant treatment (indirect benefit). This must be balanced against the morbidity of an ePLND. In line with this, a recent exhaustive systematic review by Fossati et al. [3] found that ePLND, as it is currently utilised, is associated with increased risk of postoperative complications without an oncological benefit. The findings of our present study are thus timely and important. We for the first time identify patients preoperatively that may derive both direct and indirect therapeutic benefits of an ePLND. In the present study 4.5% of the 311 061 patients had a LNI risk of >20%. This constitutes a substantial number of patients. These patients should be strongly advised to receive an ePLND. For patients constituting the LNI risk group between 5% and 20%, they should still be encouraged to undergo an ePLND after discussing the risks and benefits of it, as accurate staging may improve their survival by receipt of aHT.
Our present study is not devoid of limitations. First, it is limited by its retrospective nature, an inherent drawback of all observational studies based on administrative data. Therefore, our findings should be interpreted with caution. However, randomised data on this subject are currently scarce. The two randomised trials (NCT01812902 and NCT01555086) comparing ePLND vs limited PLND have not yet matured to provide clinically meaningful information. While we await results from these trials, our present study provides an avenue to have an informed discussion with the patients with high‐risk prostate cancer about the risks/benefits of undergoing an ePLND. Second, no centralised pathological review was available in our study. While this might be considered a limitation, it is also a strength, as it implies that our results are applicable to clinical practice, regardless of pathology review variation. Lastly, the definition of our ePLND was based on number of LNs removed rather than the anatomical zones dissected [7]. The information regarding LN zonal anatomy is not available within NCDB; however, several prior studies of anatomical ePLND have shown median LN counts between 10 and 20 [5,6,7,8], and it was 14 in our series for patients undergoing an ePLND (vs a median of two LNs for none/limited PLND), thus suggesting that the patients were likely classified appropriately into ePLND and none/limited PLND groups.
Limitations notwithstanding, our present study is the first to preoperatively identify patients in whom an ePLND may confer a direct survival advantage, in addition to superior prognostication (indirect benefit). As we identify these patients preoperatively, this may facilitate patient counselling and optimal utilisation of ePLND.
Every month, the Editor-in-Chief selects an Article of the Month from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to this post there is also an Editorial written by a prominent member of the urological community and a visual abstract created by Cora Griffin at King’s College London.We invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this month, we recommend this one.
Pascal Viktorin-Baier*†, Paul M. Putora‡§, Hans-Peter Schmid*, Ludwig Plasswilm‡§, Christoph Schwab*, Armin Thoeni¶, Werner Hochreiter**, Ladislav Prikler††, Stefan Suter‡‡, Patrick Stucki†, Michael Müntener§§, Nadja Blick§§, Hans Schiefer‡, Sabine Güsewell¶¶, Karin Zürn* and Daniel Engeler*
*Department of Urology, St. Gallen Cantonal Hospital, St. Gallen, †Urology Clinic, Cantonal Hospital Lucerne, Lucerne, ‡Department of Radiation Oncology, St. Gallen Cantonal Hospital, St. Gallen, §Department of Radiation Oncology, University of Berne, ¶Clinic for Radiation-Oncology, Lindenhof Hospital Berne, Berne, **Urology Clinic, Hirslanden Clinic Aarau, Aarau, ††Urology Clinic, Uroviva Clinic Buelach, Buelach, ‡‡Urology Clinic Zug, Zug, §§Urology Clinic, Triemli Hospital, Zurich, and ¶¶Clinical Trial Unit, St. Gallen Cantonal Hospital, St. Gallen, Switzerland
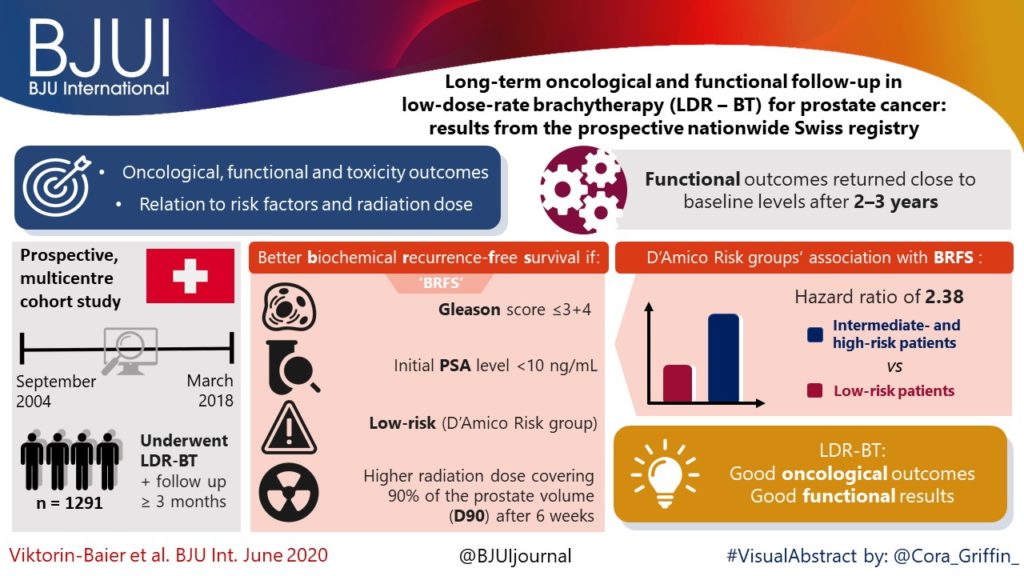
To evaluate the long‐term oncological, functional and toxicity outcomes of low‐dose‐rate brachytherapy (LDR‐BT) in relation to risk factors and radiation dose in a prospective multicentre cohort.
Patients and Methods
Data of patients from 12 Swiss centres undergoing LDR‐BT from September 2004 to March 2018 were prospectively collected. Patients with a follow‐up of ≥3 months were analysed. Functional and oncological outcomes were assessed at ~6 weeks, 6 and 12 months after implantation and annually thereafter. LDR‐BT was performed with 125I seeds. Dosimetry was done 6 weeks after implantation based on the European Society for Radiotherapy and Oncology recommendations. The Kaplan–Meier method was used for biochemical recurrence‐free survival (BRFS). A prostate‐specific antigen (PSA) rise above the PSA nadir + 2 was defined as biochemical failure. Functional outcomes were assessed by urodynamic measurement parameters and questionnaires.
Results
Of 1580 patients in the database, 1291 (81.7%) were evaluable for therapy outcome. The median (range) follow‐up was 37.1 (3.0–141.6) months. Better BRFS was found for Gleason score ≤3+4 (P = 0.03, log‐rank test) and initial PSA level of <10 ng/mL (P < 0.001). D’Amico Risk groups were significantly associated with BRFS (P < 0.001), with a hazard ratio of 2.38 for intermediate‐ and high‐risk patients vs low‐risk patients. The radiation dose covering 90% of the prostate volume (D90) after 6 weeks was significantly lower in patients with recurrence. Functional outcomes returned close to baseline levels after 2–3 years. A major limitation of these findings is a substantial loss to follow‐up.
Conclusion
Our results are in line with other studies showing that LDR‐BT is associated with good oncological outcomes together with good functional results.
The clinical results from 12 Swiss centres reaffirm the benefits of Low Dose Rate Brachytherapy (LDR-BT) for the treatment of localised prostate cancer [1]. The authors are to be commended for collating and analysing prospective, countrywide, long-term data. This is an excellent example of Good Clinical Practice for the urology community, patients, commissioning groups and for governance purposes. Prostate brachytherapy offers suitable men with prostate cancer a high chance of long-term cure but with a low risk of urinary incontinence and most retaining erectile dysfunction [2].
Two thirds of the patients reported in the Swiss series had low-risk cancer who would now more commonly be offered active surveillance as an initial treatment option. However our own and other large mature series have shown similar treatment efficacy of LDR-BT, either as monotherapy as in the Swiss study, or as a boost to external-beam radiotherapy, for the treatment of patients with intermediate and high risk of disease relapse [3, 4]. Indeed the ASCENDE-RT trial recently showed that men with unfavourable intermediate or high-risk prostate cancer randomised to an LDR-BT boost arm, relative to a dose-escalated external-beam radiotherapy boost, were twice as likely to be free of biochemical failure at a median follow-up of 6.5 years. A slight increase in urinary toxicity was observed which may have been an issue related to implant technique [5].
The authors show LDR-BT affords excellent disease control that associates with post-implant dosimetry in keeping with current treatment guidelines. They also report an association between biochemical control and seed loss. It therefore becomes unclear the extent to which implant quality or implant technique, i.e. the use of loose or stranded seeds, influenced the oncological outcome, as it would appear that more than one brachytherapy technique has been used.
In this series no prostate cancer-related deaths were reported. However the median follow-up length of 37 months is relatively short. Examples from more mature series show longer follow-up is needed to begin to document the low rates of prostate cancer-related deaths following LDR-BT. Lazarev et al [6] in a similar risk group distribution to the Swiss population, reported 97% prostate cancer-specific survival at 17-years with all deaths occurring more than 10 years after treatment. Morris et al [4] reported 99.1% cause-specific survival at 10 years with death events 9 years after treatment in low and intermediate-risk disease. Our own series showed 98% prostate-cancer-specific survival at 7 and 9 years post-implantation in high-risk (as defined by NICE) patients treated with monotherapy [3].
Treatment-related toxicity assessments in the Swiss series showed that baseline values are crucial to understand the impact of treatment on patient-reported outcomes. Higher post-implant scores were consistently observed in those patients with higher baseline scores. The patient-reported outcomes were similar to those from our series where sexual potency was preserved in 70-80% of men who were ≤60 years old at time of implant [7].
Salvage therapies are seldom given after LDR-BT as the local failure rate is low and the surgery complex. It was undertaken in only two patients in the Swiss series. In the era of mp-MRI and PSMA PET/CT scans and targeted biopsies, tumour recurrence can be better assessed. Salvage surgery has been offered to approximately 0.5% (27/4200) of our patients, by either robotic-assisted radical prostatectomy or seminal vesiculectomy if the recurrence is localised to the seminal vesicle alone.
Thisnation-wide report from the 12 Swiss centres is a welcome addition to the extensive body of evidence that attests to the excellent results and generalisability of prostate LDR-BT. The treatment is efficacious and convenient for patients with a low toxicity profile. It is a cost effective option that should be offered to all suitable patients with localised prostate cancer.
The numbers are staggering. As of the date of this brief commentary, the World Health Organization has reported more than 4.6 million cases and upwards of 311,840 deaths worldwide from the COVID-19 pandemic. The virus responsible for the disease known as COVID-19, SARS-CoV-2, is highly infectious and the risks are clearly significant for nearly everyone. Nonetheless, the risk is much higher for some of us than for others. In particular, we have begun to understand the distinct risks faced by men with prostate cancer and the unique intersection of biological, health, and lifestyle factors in COVID-19 and prostate cancer. Although there is a great deal yet to be learned, there are indeed many aspects of the overlap between COVID-19 and prostate cancer that we have already been able to discern and which we have begun to address. Perhaps most striking, older men who are at greatest risk for prostate cancer may also be at greatest risk for COVID-19.
New York City
Biology Makes a Difference – COVID-19 and prostate cancer share some common biological features. A gene responsible for male traits or characteristics, the androgen receptor, which is dysregulated or impaired in prostate cancer, is also important in COVID-19. Androgens can suppress the body’s immune response to infections and may explain the reason for higher rates of infection in men. At the same time, a gene known as TMPRSS2 is also highly expressed in both COVID-19 and prostate cancer. In fact, these issues may be related—more androgens could signify greater expression of TMPRSS2 which could create greater susceptibility to the virus. These biological risks are compounded by a number of critical health conditions and lifestyle issues.
Common Risk Factors – Studies from around the world have shown that several chronic health conditions or comorbidities create greater risk for contracting the virus, becoming more severely ill, or dying from COVID-19. It is indeed concerning that many of these are the same risks we see in prostate cancer: hypertension, diabetes, COPD, and obesity. Prostate cancer patients with multiple comorbid conditions may be at even greater risk. Cancer patients in general have weakened immune systems which makes them more vulnerable to infectious disease, further compounding the unique factors affecting men with prostate cancer. Some of the lifestyle factors that may contribute to chronic health conditions also appear to be risk factors for COVID-19 infection, most importantly smoking and high levels of alcohol consumption. We are especially concerned about men who are active smokers, as smoking has been clearly linked to worse outcomes in men who have become ill with COVID-19. We believe that the guidance we generally offer to prostate cancer patients is as, if not more, relevant now in this time of the COVID pandemic—adopt healthy habits, including smoking cessation, a nutritious diet, exercise, and proper management of chronic conditions most notably diabetes.
Looking Ahead – As the pandemic evolves and we look to the future, we are focused on ways to prevent the spread of infection and to create viable treatments for those who become ill. Worldwide, more than nine million men currently face decisions about biopsy, active surveillance, surgery, radiation, hormonal therapy, or chemotherapy related to prostate cancer in the context of COVID-19 and another 3 million more will find themselves facing these decisions by the end of this year. We are working intensely to address their needs. More than 1,460 clinical trials are underway to test therapeutic interventions to treat COVID-19. What we have come to understand about the shared biology between COVID-19 and prostate cancer and common risk factors will be invaluable. We must learn everything we can about the ways in which the virus impacts lung function as it relates to prostate cancer—the respiratory symptoms that result from infection have been especially lethal—and continue to explore the role of androgens in response to new drugs. Many drugs originally intended and approved for other uses are being tested for potential “repurposing” and new drugs and vaccines are under investigation. New clinical guidelines have been established for the treatment of prostate cancer patients at risk of or for those who have contracted the virus, and these guidelines will continue to evolve and be updated.
A Global Perspective – It is critical that we understand the COVID-19 pandemic both on the level of individual experience and global impact. For prostate cancer patients, this means recognizing the way that biology, related chronic health conditions, and lifestyle choices come together to impact the risk of disease, disease severity, and outcomes. Prostate cancer patients and their doctors must come together to find the way forward during this time of unprecedented crisis and opportunities for improving outcomes and quality of life for prostate cancer patients.
Every week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to this post, there is an editorial written by a prominent member of the urological community and a videoproduced by the authors. Please use the comment buttons below to join the conversation.
If you only have time to read one article this week, we recommend this one.
Ola Bratt*†, Linda Drevin‡, Karl-Göran Prütz§, Stefan Carlsson¶, Lars Wennberg** and Pär Stattin††
*Department of Urology, Institute of Clinical Science, Sahlgrenska Academy, Gothenburg University, †Department of Urology, Sahlgrenska University Hospital, Gothenburg, ‡Regional Cancer Centre, Uppsala-Orebro, Uppsala, §Swedish Renal Registry, Ryhov Hospital, Jönköping, ¶Section of Urology, Department of Molecular Medicine and Surgery, Karolinska Institute, **Department of Transplantation Surgery, Karolinska University Hospital, Stockholm, and ††Department of Surgical Sciences, Uppsala University, Uppsala, Sweden
To investigate whether post‐transplantation immunosuppression negatively affects prostate cancer outcomes in male kidney transplant recipients.
Patients and Methods
We used the Swedish Renal Register and the National Prostate Cancer Register to identify all kidney transplantation recipients diagnosed with prostate cancer in Sweden 1998–2016. After linking these registers with Prostate Cancer Database Sweden (PCBaSe), a case‐control study was designed to compare time period and risk category‐specific probabilities of a prostate cancer diagnosis amongst kidney transplantation recipients versus the male general population. The registers did not include information about the specific immunosuppression agent used in all transplantation recipients. Data from PCBaSe were used to compare prostate cancer characteristics at diagnosis and survival for patients with prostate cancer with versus without a kidney transplant. Propensity score matching, Cox regression analysis and Fisher’s exact test were used and 95% confidence intervals (CIs) calculated.
Prostate cancer‐specific and overall survival for all 133 Swedish men who were diagnosed with prostate cancer after kidney transplantation between 1998 and 2016, and a control group of 665 men with prostate cancer without a kidney transplant, matched for age, year of prostate cancer diagnosis, educational duration, and county of residence. The curves were constructed with the Kaplan–Meier method. There was no evidence for a difference in cancer‐specific survival (log‐rank test: P = 0.37), but overall survival was shorter (log‐rank test: P = 0.003). KT, kidney transplantation; PC, prostate cancer.
Results
Almost half of the 133 kidney transplantation recipients were transplanted before the mid‐1990s, when PSA testing became common in cancer centers. The transplant recipients were not more likely than age‐matched control men to be diagnosed with any (odds ratio [OR] 0.84, 95% CI 0.70–0.99) or high‐risk or metastatic prostate cancer (OR 0.84, 95% CI 0.62–1.13). None of the ORs for the different categories of prostate cancer increased with time since transplantation. Cancer characteristics at the time of diagnosis and cancer‐specific survival were similar amongst transplant recipients and the control group of 665 men diagnosed with prostate cancer without a kidney transplant.
Conclusions
This Swedish nationwide, register‐based study gave no indication that immunosuppression after kidney transplantation increases the risk of prostate cancer or adversely affects prostate cancer outcomes. The study suggests that men with untreated low‐grade prostate cancer can be accepted for transplantation.
To investigate whether post‐transplantation immunosuppression negatively affects prostate cancer outcomes in male kidney transplant recipients.
Patients and Methods
We used the Swedish Renal Register and the National Prostate Cancer Register to identify all kidney transplantation recipients diagnosed with prostate cancer in Sweden 1998–2016. After linking these registers with Prostate Cancer Database Sweden (PCBaSe), a case‐control study was designed to compare time period and risk category‐specific probabilities of a prostate cancer diagnosis amongst kidney transplantation recipients versus the male general population. The registers did not include information about the specific immunosuppression agent used in all transplantation recipients. Data from PCBaSe were used to compare prostate cancer characteristics at diagnosis and survival for patients with prostate cancer with versus without a kidney transplant. Propensity score matching, Cox regression analysis and Fisher’s exact test were used and 95% confidence intervals (CIs) calculated.
Results
Almost half of the 133 kidney transplantation recipients were transplanted before the mid‐1990s, when PSA testing became common. The transplant recipients were not more likely than age‐matched control men to be diagnosed with any (odds ratio [OR] 0.84, 95% CI 0.70–0.99) or high‐risk or metastatic prostate cancer (OR 0.84, 95% CI 0.62–1.13). None of the ORs for the different categories of prostate cancer increased with time since transplantation. Cancer characteristics at the time of diagnosis and cancer‐specific survival were similar amongst transplant recipients and the control group of 665 men diagnosed with prostate cancer without a kidney transplant.
Conclusions
This Swedish nationwide, register‐based study gave no indication that immunosuppression after kidney transplantation increases the risk of prostate cancer or adversely affects prostate cancer outcomes. The study suggests that men with untreated low‐grade prostate cancer can be accepted for transplantation.
Every week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to this post, there is an editorialwritten by a prominent member of the urological community. Please use the comment buttons below to join the conversation.
If you only have time to read one article this week, we recommend this one.
*Division of Sleep and Circadian Disorders, Brigham and Women’s Hospital and Harvard Medical School, Boston, MA, USA, †Department of Population Health, New York University (NYU) School of Medicine, and ‡Department of Urology, NYU School of Medicine and Manhattan Veterans Affairs, New York, NY, USA
Previous epidemiological studies have examined the relationship between sleep disturbances and prostate cancer risk and/or survival. However, less has been published about the impact of sleep disturbance on quality of life (QoL) for prostate cancer survivors and their in home caregiver. Although prostate cancer presents numerous potential barriers to sleep (e.g., hot flashes, nocturia), current survivorship guidelines do not address sleep. In addition to its impact on QoL, sleep disturbances also mediate the impact of cancer status on missed days from work and healthcare expenditures.
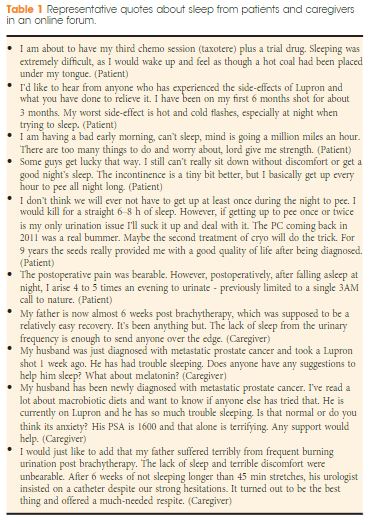
A broader examination of contributors to poor sleep in prostate cancer, and the impact on patients and caregivers would be an important contribution to raise awareness of these issues in the medical community, improve survivorship care, reduce healthcare costs, and stimulate future research. The objective of our letter is to analyse sleep barriers reported by patients with prostate cancer and caregivers posted to a large online health community. You can check lot of article on coolsculptny related to health.
“In whatever disease sleep is laborious, it is a deadly symptom,” is a famed aphorism by Hippocrates, because he deeply understood the role of sleep in the process of healing. One of the main goals of any comprehensive cancer management plan should be the provision of comfort. In academic literature, discussions of advances in prostate cancer treatment are often limited to novel therapeutics, such as immunotherapy. What gets often ignored in these discussions is the patient’s perspective—especially that of sleep disturbances. This is why an intriguing qualitative analysis in this BJUI issue by Robbins et al is a refreshing read [1]. The authors examined discussions on an online health community to elucidate the barriers to sleep among prostate cancer patients and caregivers.
Parsing through thousands of anonymized public comments, the authors report several interesting findings: one, majority of comments related to sleep (86%) are posted by patients—signifying high interest in this aspect of management; second, a plurality of comments discuss sleep medications (22%), with comments about advanced disease discussing these medications three times more than those discussing localized disease; third, associated side effects of fatigue and pain were largely observed in advanced disease comments, according to Discover Magazine many people is using this website https://observer.com/2020/05/best-cbd-hemp-flower/ to buy CBD and reduce the pain cause by the disease . Interestingly, the authors also used Linguistic Inquiry Word Count (LIWC) software—a reasonable tool to assess emotional states—and reported that advanced disease comments were significantly more negative in perspective than localized disease comments. This analysis is an especially useful contribution—and should enable contemporary Prostate Cancer Survivorship Care Guidelines to expand on the impact of sleep disturbances [1].
These findings have considerable implications. To start with, these findings need to be contextualized within the larger body of evidence we have on impact of sleep disturbances on prostate cancer. In a recent study, Markt et al prospectively followed 32,141 men (with 4261 prostate cancer cases) using the Health Professionals Follow-Up Study (HPFS), and found no association between self-reported duration of sleep and prostate cancer outcomes [2]. However, the authors of the HPFS study did emphasize that sleep disruptions were associated with increased risk of developing lethal or aggressive prostate cancer. The finding by Robbins et al that a significant proportion of patients are discussing these issues through online communities suggests that the prevalence of sleep disturbance—and its impact on quality of life—among prostate cancer patients is poorly understood and inadequately measured.
Representative quotes highlighted by Robbins et al also reveal that prostate cancer patients often suffer from severe insomnia, indicating lack of sleep-related patient education initiatives. Additionally, quotes by caregivers also underscore that there is a general lack of information on how to address sleep disruptions for patients they attend to. This is a missed opportunity, as evidence suggests that nutritional therapy (soy supplementation, for example) and combination of resistance training with aerobic exercise may improve cancer related fatigue and quality of life among prostate cancer patients [3], although less is known about effective interventions that would improve sleep. Furthermore, disturbances in sleep have expensive implications for health care spending and workplace absenteeism—with prostate cancer survivorship phase accounting for 50% of total cancer care related costs [4]. Studies that have investigated this relationship report that sleep disturbances significantly increase the utilization of health care and workplace absenteeism, with the impact constituting 2% and 8%, respectively [4]. Given the exponential rise in overall health care spending in the United States, addressing costs stemming from preventable adverse events is urgent—this present study demonstrates that more creative interventions are wanting.
Beyond economic and survivorship care concerns, this qualitative study paints a grim picture of the conversations happening in these online patient communities, with comments revealing a negative emotional state for many. While sleep disturbances are an important contributor for this development, lack of patient education can also engender greater confusion and distress. Findings from this study should spur greater interest and support for devising and implementing patient-centered initiatives that improve sleep quality. This is required not only because these will likely improve the quality of life for prostate cancer patients, but also because we have a moral responsibility to provide comfort for these patients.