What’s the Diagnosis?
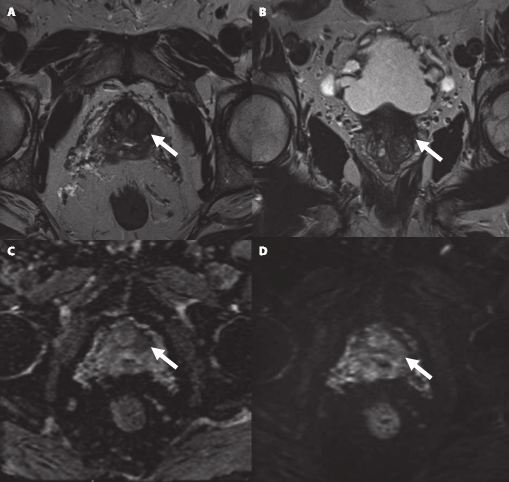
This man has intermediate/ high-risk prostate cancer.
Taken from Daouacher et al, BJUI 2016
No such quiz/survey/poll
This man has intermediate/ high-risk prostate cancer.
Taken from Daouacher et al, BJUI 2016
No such quiz/survey/pollEvery Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video from , discussing their paper.
If you only have time to read one article this week, it should be this one.
To examine the value of additional transrectal ultrasonography (TRUS)-guided random biopsy (RB) in patients with negative magnetic resonance imaging (MRI)/ultrasonography (US) fusion-guided targeted biopsy (TB) and to identify possible reasons for TB failure.
We conducted a subgroup analysis of 61 men with prostate cancer (PCa) detected by 10-core RB but with a negative TB, from a cohort of 408 men with suspicious multiparametric magnetic resonance imaging (mpMRI) between January 2012 and January 2015. A consensus re-reading of mpMRI results (using Prostate Imaging Reporting and Data System [PI-RADS] versions 1 and 2) for each suspicious lesion was performed, with the image reader blinded to the biopsy results, followed by an unblinded anatomical correlation of the lesion on mpMRI to the biopsy result. The potential reasons for TB failure were estimated for each lesion. We defined clinically significant PCa according to the Epstein criteria and stratified patients into risk groups according to the European Association of Urology guidelines.
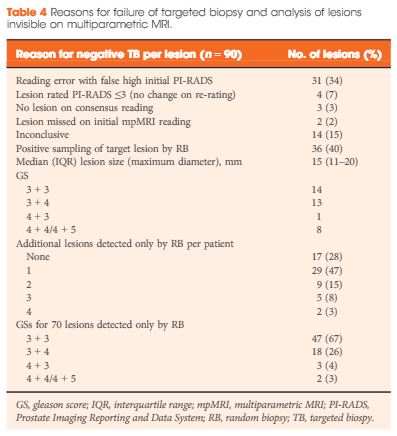
Our analysis showed that RB detected significant PCa in 64% of patients (39/61) and intermediate-/high-risk PCa in 57% of patients (35/61). The initial mpMRI reading identified 90 suspicious lesions in the cohort. Blinded consensus re-reading of the mpMRI led to PI-RADS score downgrading of 45 lesions (50%) and upgrading of 13 lesions (14%); thus, negative TB could be explained by falsely high initial PI-RADS scores for 32 lesions (34%) and sampling of the target lesion by RB in the corresponding anatomical site for 36 out of 90 lesions (40%) in 35 of 61 patients (57%). Sampling of the target lesion by RB was most likely for lesions with PI-RADS scores of 4/5 and Gleason scores (GS) of ≥7. A total of 70 PCa lesions (67% with GS 6) in 44 patients (72%) were sampled from prostatic sites with no abnormalities on mpMRI.
In cases of TB failure, RB still detected a high rate of significant PCa. The main reason for a negative TB was a TB error, compensated for by positive sampling of the target lesion by the additional RB, and the second reason for TB failure was a falsely high initial PI-RADS score. The challenges that arise for both MRI diagnostics and prostate lesion sampling are evident in our data and support the integration of RB into the TB workflow.
MRI information of the prostate is increasingly used for improving the diagnostic yield of prostate biopsies [1]. However, increasing complexity of a procedure makes it prone to errors at multiple technical and human levels. Incorporating MRI information and ultrasonography (US) images for MRI-fusion biopsies is a technically challenging task. It involves various steps such as the acquisition and fusion of MRI and US images, the needle guidance during biopsy, and the diligence of the pathological evaluation of biopsy specimens. These different steps and interfaces between different medical professions influence the diagnostic performance of MRI-fusion biopsies.
For example, in daily clinical practice, MRIs from different institutions still harbour a great variance of sequences and reporting, despite the European Society of Urogenital Urology (ESUR) recently introducing acquisition and imaging protocols and a new and advanced version of the Prostate Imaging Reporting and Data System (PIRADS) version 2.0 [2]. The usefulness of such reporting schemes is evidenced by a moderate-to-good interobserver agreement between uro-radiologists for tumour lesion interpretation and corresponding κ values ranging from 0.55 to 0.80 [3]. Important pitfalls of image interpretation are benign lesions such as prostatitis, BPH and fibrosis, which might score similarly to prostate cancer lesions. This problem is further aggravated by a high proportion of patients that receive their first multiparametric MRI (mpMRI) of the prostate in the repeat-biopsy setting with a high burden of post-biopsy artefacts (haemorrhage, capsular irregularity) and lower overall cancer detection rate. Also, during MRI-fusion biopsy patient movement, prostate deformation by the US probe, and mismatch of image planes can lead to a biopsy error exceeding 4 mm. Moreover, targeting error might be aggravated by MRI underestimation of the tumour volume compared with final pathology [4]. After various authors reported the advantages and accuracy of MRI/US-fusion biopsy approaches, Cash et al. [5] address potential reasons for targeted biopsy failure to detect prostate cancer compared with random biopsy. Within their analyses the authors address potential limitations and technical considerations. Based on different technical biopsy strategies (with the patient placed within the MRI scanner (‘in-bore’) vs outside) and different technical approaches, these considerations are very important.
In contrast to cognitive fusion, most MRI/US platforms allow needle tracking by archiving the needle orientation, either by an electromagnetic, image-based or stepper-based mechanism [1]. However, lesion targeting by needle guidance is highly dependent on the dimensions of the primary lesion, numbers of relevant lesions, localisation, and overall prostate volume, making MRI-US fusion and cognitive fusion more error prone (i.e. aiming off the mark with the needle) than in-bore biopsies. Moreover, different technical fusion approaches provide different degrees of manual/automated adjustment tools, with for example either rigid or elastic image transformation to facilitate MRI/US image alignment.
In their analyses, Cash et al. [5] found that 34% of negative targeted biopsies could be explained by initially too high estimated PIRADS scores that were downgraded at re-reading. Interestingly, the remaining lesions were without an mpMRI correlate but within this group 92.9% showed a primary Gleason 3 pattern in biopsy pathology, suggesting a high degree of invisibility on mpMRI. Subanalyses did not show an association of targeted biopsy failures in the ventral location. Therefore, the study by Cash et al. [5] is an important precursor for further analyses to address other underlying reasons for targeted biopsy failure. Moreover, it reveals the need for a tight collaboration of radiologists, urologists, and pathologists as interdisciplinary partners involved in MRI-fusion biopsy. Consequently, the optimal diagnostic performance of MRI-fusion biopsies can only be achieved through standardised MRI performance, reading and reporting of MRI findings, as well as final correlation of MRI findings with histopathological work up.
To examine the value of additional transrectal ultrasonography (TRUS)-guided random biopsy (RB) in patients with negative magnetic resonance imaging (MRI)/ultrasonography (US) fusion-guided targeted biopsy (TB) and to identify possible reasons for TB failure.
We conducted a subgroup analysis of 61 men with prostate cancer (PCa) detected by 10-core RB but with a negative TB, from a cohort of 408 men with suspicious multiparametric magnetic resonance imaging (mpMRI) between January 2012 and January 2015. A consensus re-reading of mpMRI results (using Prostate Imaging Reporting and Data System [PI-RADS] versions 1 and 2) for each suspicious lesion was performed, with the image reader blinded to the biopsy results, followed by an unblinded anatomical correlation of the lesion on mpMRI to the biopsy result. The potential reasons for TB failure were estimated for each lesion. We defined clinically significant PCa according to the Epstein criteria and stratified patients into risk groups according to the European Association of Urology guidelines.
Our analysis showed that RB detected significant PCa in 64% of patients (39/61) and intermediate-/high-risk PCa in 57% of patients (35/61). The initial mpMRI reading identified 90 suspicious lesions in the cohort. Blinded consensus re-reading of the mpMRI led to PI-RADS score downgrading of 45 lesions (50%) and upgrading of 13 lesions (14%); thus, negative TB could be explained by falsely high initial PI-RADS scores for 32 lesions (34%) and sampling of the target lesion by RB in the corresponding anatomical site for 36 out of 90 lesions (40%) in 35 of 61 patients (57%). Sampling of the target lesion by RB was most likely for lesions with PI-RADS scores of 4/5 and Gleason scores (GS) of ≥7. A total of 70 PCa lesions (67% with GS 6) in 44 patients (72%) were sampled from prostatic sites with no abnormalities on mpMRI.
In cases of TB failure, RB still detected a high rate of significant PCa. The main reason for a negative TB was a TB error, compensated for by positive sampling of the target lesion by the additional RB, and the second reason for TB failure was a falsely high initial PI-RADS score. The challenges that arise for both MRI diagnostics and prostate lesion sampling are evident in our data and support the integration of RB into the TB workflow.
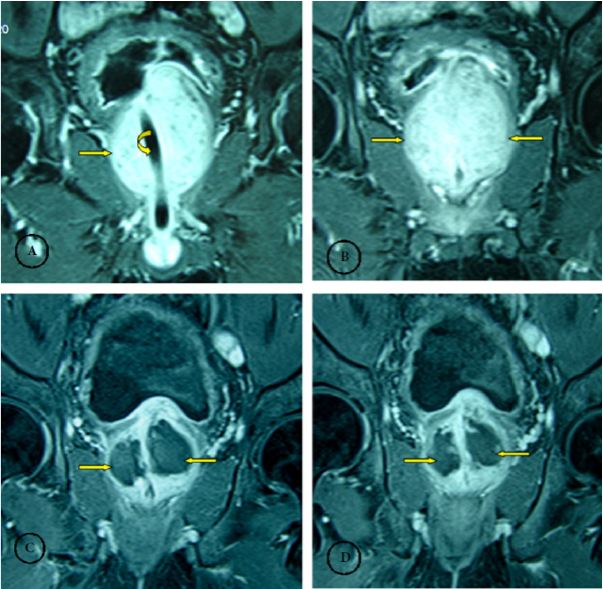
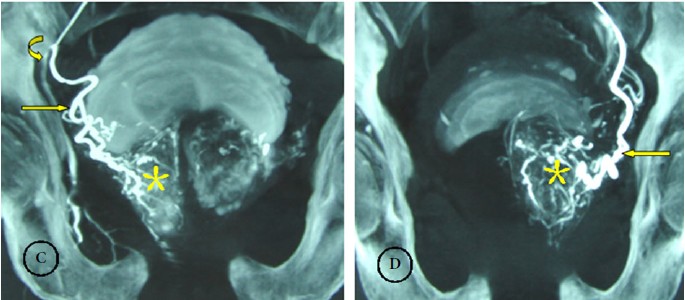
These images are taken from Wang et al, BJUI 2016.
This man has a large prostate (148cc) and urinary retention. Images A and B are before treatment. Images C and D are 1 month after treatment with prostate artery embolization. (see last week’s images)
No such quiz/survey/poll
These images are taken from Wang et al, BJUI 2016.
This man has a large prostate (148cc) and urinary retention.
No such quiz/survey/pollEvery Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video from Dr. Peter Carroll, discussing his paper.
If you only have time to read one article this week, it should be this one.
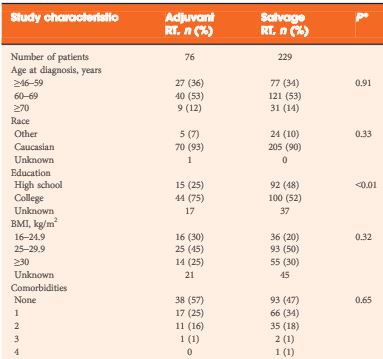
To evaluate among radical prostatectomy (RP) patients at high-risk of recurrence whether the timing of postoperative radiation therapy (RT) (adjuvant, early salvage with detectable post-RP prostate-specific antigen [PSA], or ‘late’ salvage with a PSA level of >1.0 ng/mL) is significantly associated with overall survival (OS), prostate-cancer specific survival or metastasis-free survival, in a longitudinal cohort.
Of 6 176 RP patients in the Cancer of the Prostate Strategic Urologic Research Endeavor (CaPSURE), 305 patients with high-risk pathological features (margin positivity, Gleason score 8–10, or pT3–4) who underwent postoperative RT were examined, either in the adjuvant (≤6 months after RP with undetectable PSA levels, 76 patients) or salvage setting (>6 months after RP or pre-RT PSA level of >0.1 ng/mL, 229 patients). Early (PSA level of ≤1.0 ng/mL, 180 patients) or late salvage RT (PSA level >1.0 ng/mL, 49 patients) was based on post-RP, pre-RT PSA level. Multivariable Cox regression examined associations with all-cause mortality and prostate cancer-specific mortality and/or metastases (PCSMM).
After a median of 74 months after RP, 65 men had died (with 37 events of PCSMM). Adjuvant and salvage RT patients had comparable high-risk features. Compared with adjuvant, salvage RT (early or late) had an increased association with all-cause mortality (hazard ratio [HR] 2.7, P = 0.018) and with PCSMM (HR 4.0, P = 0.015). PCSMM-free survival differed by further stratification of timing, with 10-year estimates of 88%, 84%, and 71% for adjuvant, early salvage, and late salvage RT, respectively (P = 0.026). For PCSMM-free survival and OS, compared with adjuvant RT, late salvage RT had statistically significantly increased risk; however, early salvage RT did not.
This analysis suggests that patients who underwent early salvage RT with PSA levels of <1.0 ng/mL may have comparable metastasis-free survival and OS compared with adjuvant RT; however, late salvage RT with a PSA level of >1.0 ng/mL is associated with worse clinical outcomes.
The appropriate treatment for clinically localized prostate cancer continues to generate controversy. For men with low grade disease it is unclear whether surgery or radiation therapy provides a survival advantage over active surveillance, and among men with high grade disease it is unclear how many derive a substantial benefit from either intervention. No trial has yet to compare surgery and radiation with observation, but the recent update of the Scandinavian Prostate Cancer Group 4 study suggests that radical prostatectomy provides a significant survival advantage for younger men with intermediate grade disease [1].
Unfortunately, many men undergoing radical prostatectomy are not cured of their disease. The Scandinavian Prostate Cancer Group 4 study has shown that as many as 26% of men undergoing surgery developed distant metastases and 18% died from their disease after a median follow-up of 13 years. For this reason many clinicians recommend additional radiation therapy for those men undergoing surgery who are at high risk of disease recurrence. Three randomized trials now support the use of radiation therapy in this setting. Two have shown lower rates of biochemical progression and one has shown improved distant metastases-free survival and overall survival [2-4]. These trials compared the use of adjuvant radiation therapy with observation. Some clinicians, however, are reluctant to refer patients for radiation therapy because of concerns about its potential impact on quality of life. This is especially true for those patients who have yet to show any evidence of biochemical recurrence.
In a manuscript published in this month’s BJUI, Hsu et al. [5] have turned to a large national prostate cancer registry that has accrued men with newly diagnosed prostate cancer since 1995. They evaluated the long-term outcomes of these men to gain insights into whether a delay in the initiation of radiation therapy compromises survival. Their findings suggest that delaying the initiation of radiation therapy until there is evidence of biochemical recurrence does not seriously compromise long-term outcomes and avoids radiation in some men who are never destined to have disease progression.
The authors are appropriately cautious with their conclusions and clearly recognize the limitations of a non-randomized study. In a registry study it is impossible to control adequately for selection biases. Men receiving adjuvant therapy had no evidence of biochemical recurrence at the time radiation was started. This group of men included both men who were destined to have disease progression and men who were destined to maintain an undetectable PSA. This differs from the men receiving salvage radiation therapy. All men receiving salvage radiation had evidence of disease progression and therefore their tumour burden and their long-term prognosis was probably worse when compared with men receiving adjuvant therapy. Despite this selection bias, men initiating salvage radiation when their postoperative PSA level was still <1.0 ng/mL had similar long-term outcomes when compared with the men receiving adjuvant radiation. Men with postoperative PSA levels >1.0 ng/mL had a much higher risk of aggressive disease and a worse outcome.
Ideally, the question about the timing of postoperative radiation would be subjected to a randomized trial. Until then, the information provided by Hsu et al. provides strong clinical support for a practical approach to the question of who should receive postoperative radiation. Men who are clearly at high risk of disease progression, which includes men with Gleason 8–10 disease and those with extensive margin positive disease and seminal vesicle invasion, should probably receive adjuvant radiation therapy as soon as they have recovered from surgery. For men with Gleason 7 disease or those men who have focal margin-positive disease it may make sense to monitor postoperative PSA levels closely and refer men for postoperative radiation when there is evidence of biochemical progression and before the PSA level reaches 1.0 ng/mL. This approach would spare some men the need for additional treatment and would defer treatment for many years in others. Men who are eventually found to have biochemical recurrence should feel reasonably comfortable that the delay in initiating radiation therapy is unlikely to have caused any significant compromise of their long-term outcome and probably improved their quality of life.
Large case series analyses frequently have selection biases that confound conclusions. In this instance the authors have cautiously interpreted a large community-based registry to gain a valuable insight into the management of localized prostate cancer. Their analysis provides appropriate support for their conclusions.
To evaluate among radical prostatectomy (RP) patients at high-risk of recurrence whether the timing of postoperative radiation therapy (RT) (adjuvant, early salvage with detectable post-RP prostate-specific antigen [PSA], or ‘late’ salvage with a PSA level of >1.0 ng/mL) is significantly associated with overall survival (OS), prostate-cancer specific survival or metastasis-free survival, in a longitudinal cohort.
Of 6 176 RP patients in the Cancer of the Prostate Strategic Urologic Research Endeavor (CaPSURE), 305 patients with high-risk pathological features (margin positivity, Gleason score 8–10, or pT3–4) who underwent postoperative RT were examined, either in the adjuvant (≤6 months after RP with undetectable PSA levels, 76 patients) or salvage setting (>6 months after RP or pre-RT PSA level of >0.1 ng/mL, 229 patients). Early (PSA level of ≤1.0 ng/mL, 180 patients) or late salvage RT (PSA level >1.0 ng/mL, 49 patients) was based on post-RP, pre-RT PSA level. Multivariable Cox regression examined associations with all-cause mortality and prostate cancer-specific mortality and/or metastases (PCSMM).
After a median of 74 months after RP, 65 men had died (with 37 events of PCSMM). Adjuvant and salvage RT patients had comparable high-risk features. Compared with adjuvant, salvage RT (early or late) had an increased association with all-cause mortality (hazard ratio [HR] 2.7, P = 0.018) and with PCSMM (HR 4.0, P = 0.015). PCSMM-free survival differed by further stratification of timing, with 10-year estimates of 88%, 84%, and 71% for adjuvant, early salvage, and late salvage RT, respectively (P = 0.026). For PCSMM-free survival and OS, compared with adjuvant RT, late salvage RT had statistically significantly increased risk; however, early salvage RT did not.
This analysis suggests that patients who underwent early salvage RT with PSA levels of <1.0 ng/mL may have comparable metastasis-free survival and OS compared with adjuvant RT; however, late salvage RT with a PSA level of >1.0 ng/mL is associated with worse clinical outcomes.
Every Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video from Dr. Giorgio Russo, discussing his paper.
If you only have time to read one article this week, it should be this one.
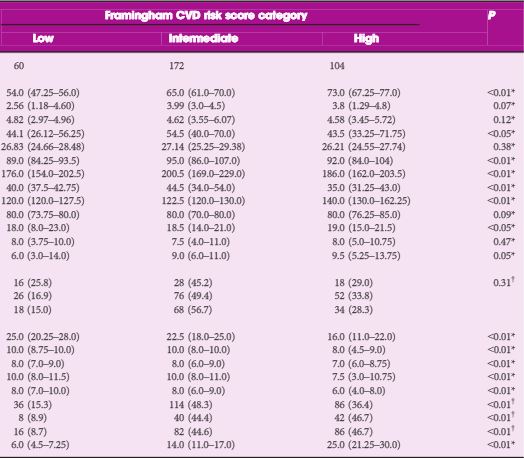
To determine the relationship between lower urinary tract symptoms (LUTS)/benign prostatic hyperplasia (BPH) and 10-year risk of cardiovascular disease (CVD) assessed by the Framingham CVD risk score in a cohort of patients without previous episodes of stroke and/or acute myocardial infarction.
From September 2010 to September 2014, 336 consecutive patients with BPH-related LUTS were prospectively enrolled. The general 10-year Framingham CVD risk score, expressed as percentage and assessing the risk of atherosclerotic CVD events, was calculated for each patient. Individuals with low risk had ≤10% CVD risk at 10 years, with intermediate risk 10–20% and with high risk ≥20%. Logistic regression analyses were used to identify variables for predicting a Framingham CVD risk score of ≥10% and moderate–severe LUTS (International Prostate Symptom Score [IPSS] ≥8), adjusted for confounding factors.
As category of Framingham CVD risk score increased, we observed higher IPSS (18.0 vs 18.50 vs 19.0; P < 0.05), high IPSS–voiding (6.0 vs 9.0 vs 9.5; P < 0.05) and worse sexual function. Prostate volume significantly increased in those with intermediate- vs low-risk scores (54.5 vs 44.1 mL; P < 0.05). Multivariate logistic regression analysis showed that intermediate- [odds ratio (OR) 8.65; P < 0.01) and high-risk scores (OR 1.79; P < 0.05) were independently associated with moderate–severe LUTS. At age-adjusted logistic regression analysis, moderate–severe LUTS was independently associated with Framingham CVD risk score of ≥10% (OR 5.91; P < 0.05).
Our cross-sectional study in a cohort of patients with LUTS–BPH showed an increase of more than five-fold of having a Framingham CVD risk score of ≥10% in men with moderate–severe LUTS.