Article of the week: Prognostic Gleason grade group predicts survival
Every week the Editor-in-Chief selects the Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Prognostic Gleason grade grouping: data based on the modified Gleason scoring system
Phillip M. Pierorazio*, Patrick C. Walsh*, Alan W. Partin* and Jonathan I. Epstein*†‡
Departments of *Urology, †Pathology and ‡Oncology, The Johns Hopkins Medical Institutions and The James Brady Buchannan Urological Institute, Baltimore, MD, USA
OBJECTIVE
• To investigate pathological and short-term outcomes since the most recent Gleason system modifications by the International Society of Urological Pathology (ISUP) in an attempt to divide the current Gleason grading system into prognostically accurate Gleason grade groups.
PATIENTS AND METHODS
• We queried the Johns Hopkins Radical Prostatectomy Database (1982–2011), approved by the institutional review board, for men undergoing radical prostatectomy (RP) without a tertiary pattern since 2004 and identified 7869 men.
• Multivariable models were created using preoperative and postoperative variables; prognostic grade group (Gleason grade ≤6; 3 + 4; 4 + 3; 8; 9–10) was among the strongest predictors of biochemical recurrence-free (BFS) survival.
RESULTS
• Significant differences were noted among the Gleason grade groups at biopsy; differences were noted in the race, PSA level, clinical stage, number of positive cores at biopsy and the maximum percentage of positive cores among the Gleason grade groups at RP.
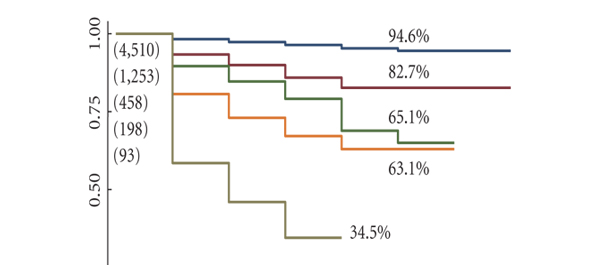
• With a median (range) follow-up of 2 (1–7) years, 5-year BFS rates for men with Gleason grade ≤6, 3 + 4, 4 + 3, 8 and 9–10 tumours at biopsy were 94.6, 82.7, 65.1, 63.1 and 34.5%, respectively (P < 0.001 for trend); and 96.6, 88.1, 69.7, 63.7 and 34.5%, respectively (P < 0.001), based on RP pathology.
CONCLUSIONS
• The 2005 ISUP modifications to the Gleason grading system for prostate carcinoma accurately categorize patients by pathological findings and short-term biochemical outcomes but, while retaining the essence of the Gleason system, there is a need for a change in its reporting to more closely reflect tumour behaviour.
• We propose reporting Gleason grades, including prognostic grade groups which accurately reflect prognosis as follows: Gleason score ≤6 (prognostic grade group I); Gleason score 3+4=7 (prognostic grade group II); Gleason score 4+3=7 (prognostic grade group III); Gleason score 4+4=8 (prognostic grade group (IV); and Gleason score 9–10 (prognostic grade group (V).
Read Previous Articles of the Week