Every Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
European Randomised Study of Screening for Prostate Cancer (ERSPC) risk calculators significantly outperform the Prostate Cancer Prevention Trial (PCPT) 2.0 in the prediction of prostate cancer: a multi-institutional study
To analyse the performance of the Prostate Cancer Prevention Trial Risk Calculator (PCPT-RC) and two iterations of the European Randomised Study of Screening for Prostate Cancer (ERSPC) Risk Calculator, one of which incorporates prostate volume (ERSPC-RC) and the other of which incorporates prostate volume and the prostate health index (PHI) in a referral population (ERSPC-PHI).
Patients and Methods
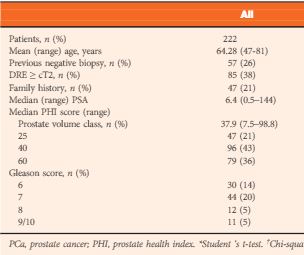
The risk of prostate cancer (PCa) and significant PCa (Gleason score ≥7) in 2001 patients from six tertiary referral centres was calculated according to the PCPT-RC and ERSPC-RC formulae. The calculators’ predictions were analysed using the area under the receiver-operating characteristic curve (AUC), calibration plots, Hosmer–Lemeshow test for goodness of fit and decision-curve analysis. In a subset of 222 patients for whom the PHI score was available, each patient’s risk was calculated as per the ERSPC-RC and ERSPC-PHI risk calculators.
Results
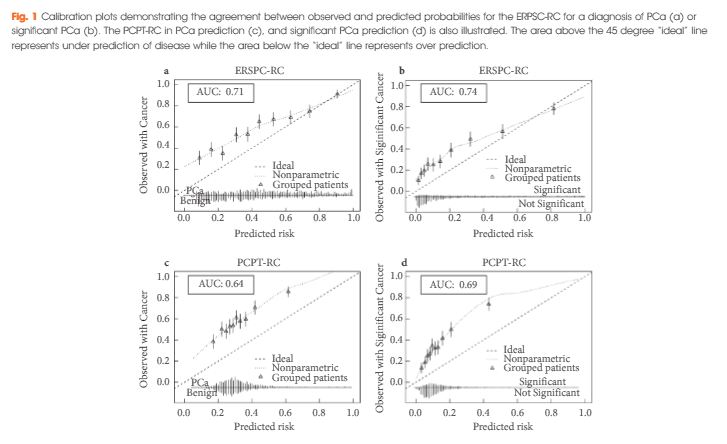
The ERSPC-RC outperformed the PCPT-RC in the prediction of PCa, with an AUC of 0.71 compared with 0.64, and also outperformed the PCPT-RC in the prediction of significant PCa (P<0.001), with an AUC of 0.74 compared with 0.69. The ERSPC-RC was found to have improved calibration in this cohort and was associated with a greater net benefit on decision-curve analysis for both PCa and significant PCa. The performance of the ERSPC-RC was further improved through the addition of the PHI score in a subset of 222 patients. The AUCs of the ERSPC-PHI were 0.76 and 0.78 for PCa and significant PCa prediction, respectively, in comparison with AUC values of 0.72 in the prediction of both PCa and significant PCa for the ERSPC-RC (P = 0.12 and P = 0.04, respectively). The ERSPC-PHI risk calculator was well calibrated in this cohort and had an increase in net benefit over that of the ERSPC-RC.
Conclusions
The performance of the risk calculators in the present cohort shows that the ERSPC-RC is a superior tool in the prediction of PCa; however the performance of the ERSPC-RC in this population does not yet warrant its use in clinical practice. The incorporation of the PHI score into the ERSPC-PHI risk calculator allowed each patient’s risk to be more accurately quantified. Individual patient risk calculation using the ERSPC-PHI risk calculator can be undertaken in order to allow a systematic approach to patient risk stratification and to aid in the diagnosis of PCa.
Several risk calculators (RCs) have been developed to predict prostate cancer (PCa) diagnosis at prostate biopsy. These multivariable tools have constantly been shown to be superior to risk prediction using PSA testing alone. Their use in personalized clinical decision-making is thus increasingly recommended to reduce overdiagnosis and overtreatment of PCa [1]. Foley et al. [2] conducted a multi-institutional external validation of the most recent versions of the European Randomised Study of Screening for Prostate Cancer Risk Calculator (ERSPC-RC) and the Prostate Cancer Prevention Trial Risk Calculator (PCPT-RC) in a large cohort of patients from six different Irish tertiary referral centres. The study showed that the two RCs performed moderately well. Both RCs performed less optimistic compared with their original reports. The ERSPC-RC showed superior discrimination (area under the curve of 0.74 vs 0.69 for high grade PCa) and a greater net benefit in decision-curve analysis (DCA) than the PCPT-RC; however, although the ERSPC-RC was superior to the PCPT-RC in this well-conducted study, neither RC can be recommended for PCa risk prediction in this specific Irish cohort.
The authors chose to perform DCAs, which are of great value for further assessing the utility of a risk prediction model using visualization of the clinical net benefit and net harm. The benefit threshold of >30%, as shown in the DCA of the ERSPC-RC for high grade PCa, is too high for a clinically meaningful prediction tool. Below this threshold the RC did not provide further benefit compared with a strategy of performing a biopsy on everybody. It is questionable whether clinicians or patients would opt to use an RC which only provides a benefit if a risk of 30% as the lowest acceptable threshold for high grade disease is accepted.
What are the reasons for the suboptimum performance of the RCs in the Irish cohort? It is well known that RC performance is often less optimistic in external validations [3]. Differences in cohort characteristics, biopsy strategies and screening recommendations between RC development cohorts and the tested cohorts, but also changes in clinical practice over time, are potential reasons. Although the RCs have constantly been modified to establish their role as a general one-size-fits-all risk prediction model, their performance varied significantly in different cohorts. We recently evaluated the same RCs in a large Swiss single-centre cohort and found similar discrimination but better calibration, a greater net benefit and a lower and thus clinically useful benefit threshold in DCAs compared with the present Irish study [4]. The cohort in the present study was unique because it consisted of a highly preselected group of patients. This is attributable to the specific referral practice for prostate biopsies in Ireland and is reflected in the high number of patients with a positive DRE (47% in the group diagnosed with PCa) or a positive family history (11%). Accordingly, the overall PCa detection rate (58%) and the detection rate of high grade disease (35%) were higher than usually expected. From a scientific point of view, the Irish cohort is not the optimum cohort to validate these RCs. Far more importantly, however, from a clinical point of view, the evaluation showed that these RCs are not really useful in the specific Irish health system.
What can be done to improve the performance RCs in the future? It is obvious that specific characteristics of the tested cohorts will affect RC performance. These local or regional characteristics usually cannot be changed. Thus modifications of available RCs according to local patient practice might be necessary. This concept has recently been examined by Strobl et al. [5]. They were able to show that recalibration of the static PCPT-RC according to local cohort and practice characteristics can improve its accuracy. Additionally, RCs developed from contemporary clinical cohorts that were, for example, diagnosed using current state-of-the-art biopsy strategies (i.e. 12-core biopsies) instead of historical cohorts from, for example, randomized clinical trials might also result in better RC performance in clinical practice. Furthermore, the inclusion of novel variables in the RC might be useful. Results from imaging studies, such as multiparametric prostate MRI, or promising new biomarkers might increase the overall performance of PCa RCs. The study by Foley et al. shows that the inclusion of novel markers can be of benefit. The ERSPC-PHI RC, which includes the Prostate Health Index (PHI) as an additional variable, was investigated in a subset of patients in their study and was superior to the conventional ERSPC-RC; however, when novel variables are integrated, their potential clinical harm (e.g. unpleasant or costly investigations) has to be balanced against their potential benefit.
The work of Foley et al. nicely illustrates the limitations of current PCa RCs. Locally tailored static RCs, RCs based on contemporary clinical cohorts, or RCs including novel variables need to be developed to assess whether overall RC performance can be improved in the future. There is still much work to do!
Hola como estas? The 36th SIU congress was held in Buenos Aires, Argentina 20-24th October. Their motto: ‘we bring urologists together’ was certainly fulfilled as reflected by the warm atmosphere and international mix of speakers and attendees. The scientific programme included plenary sessions, debates, hands on instructional courses, trainee Q&A sessions and symposiums.
The location and facilities at the Hilton were first class. A large exhibition hall allowed for interaction with industry. The use of the pool bar hosted by the SIU innovators group was a particular highlight.
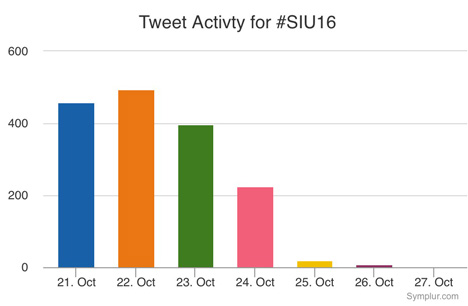
The conference app was easy to use and the conference hashtag #SIU16 and a #selfie challenge were promoted. The selfie prize of a trip to SIU Portugal was won by Argentine resident Dr. Jose Nolazco with over 300 likes!
Thursday
The conference kicked off with varied and interesting sessions on a range of urology, which included sub-section meetings such as societies of the Middle East, Africa, Asia, and Argentina; plus the 2nd SIU nurses educational symposium. The most popular meeting (in numbers attending and discussions after) was the World Urological Oncology Federation Symposium (WUOF). A delegate from South Africa told me that he appreciated the summary of new research and highlighting the areas of change, especially in a field when advances can occur quickly, for example PMSA-PET which may be able to give more information on metastatic prostate cancer than MRI. Arnaud Villiers vs Robert Reiter debated the issue of focused vs radical therapy to an intermediate, solitary lesion in the prostate. Reiter argued NOT for focal therapy on the basis of the imperfections of the MRI.
The MRI-TRUS fusion course, hosted by SIU Innovators division and with MIMS from industry present, championed MRI as a primary diagnostic test to investigate prostate cancer. Boris Hadaslick quoted (PROMIS trial) that TRUS biopsy without MRI had a 50% chance of finding cancer: ‘like flipping a coin’. He emphasised that targeted plus systematic biopsy sampling was best practice and highlighted the fusion software systems can improve cancer diagnosis. However cognitive fusion can be as good.
Speakers enthusiastic about advances in urology described high costs that had to be justified to their healthcare system like PSMA-PET and immunotherapy for bladder cancer. Yet these costs would be impossible for other delegates to take back to their home countries. Indeed the most innovative speakers presented their cost-saving techniques in the ‘SANTU’ session; the opening remarks of ‘how can you drive a Ferrari if you don’t have paved roads?’ was particularly levelling. One speaker, Mohammed Lezrek, stood out as being particularly creative, which he says is as a result of necessity, he showed videos using rubber from syringes or saline bag ports to fix the bungs on his endoscopes in Morocco (https://m.youtube.com/user/lezrekmohamed). These are issues I wouldn’t even think to know how to fix, being fortunate enough to work in the NHS. Other speakers in the same session described using generic, mass produced Ureteric stents that were a fraction of the price, another described treating a condition common to him in Indonesia of penile dermatosclerosis caused by penile injections of oil obtained as easily as ‘getting a haircut’ with the low cost surgical technique of scrotal flap. There was also a symposium on Urology in the Developing World, which included the best-titled talk: ‘the hunt for the perfect penis’ given by Ms Rampersad. She is the only surgeon performing hypospadias repair in Trinidad and Tobago, at an incidence of 2.7 per 1000 live births and recommended that specialist surgery be performed by those who are keen and performing larger volumes.
The Endourology Society Symposium was a popular session with standing room only. There were lessons on the possibilities, but also the limitations of flexible ureteroscopy, including an impromptu debate on use of access sheath and a case of stone clearance in a patient with HSK. A Canadian audience member spoke of his difficulty in justifying the use of flexi URS to managers in view of longer operation time compared to PCNL due to OR pressure. Michael Grasso captivated the audience with his experience in using flexible URS for diagnosis and treating upper tract TCC. In his series this meant less nephrectomies, no dialysis and better palliation. He even does LA flexi URS in selected patients! An important message on the dangers of IntraRenal pressure was presented by Palle Osther, which can occur even at an irrigation height of 40cm. He highlighted that whilst papers are championing the use of Flexi URS in more complex cases this means more time in the renal pelvis with the added risk of complications. He quoted Hippocrates ‘do no harm’. Grasso and Olivier Traxer explained their methods of stringent use of irrigation via piston controlled syringe and limiting operation time to an hour.
My personal highlight was the presentation of videos by Mr René Sotelo on ‘getting out of sticky situations’ (SIU innovators symposium). An expert panel described similar mistakes to the ones shown on the videos and added what they would do if faced with the problem, leading to a fruitful and rich discussion. He showed tachycardia inducing, faint provoking videos of bleeding from upper and lower tract minimally invasive surgery. Advice such as stay calm, phone a friend, increase the pneumo, ‘suture fast’ was useful and practical. One case showed a rectal perforation at cystectomy where the attending/junior had been asked to place a swab (on stick) into the vagina, but it became apparent once the swab was on show and the vagina was intact that the swab had been misplaced into the rectum, thus highlighting the need to know your anatomy! An amazing image of a Ureteric stent that had been accidentally placed in the atrium was shown; but we were told the next step should not be to call an endourologist!
In the opening ceremony we were welcomed by Argentine tango dancers, the Minister of Health: a qualified doctor with degree in public health, and some Argentine hospitality of wine and typical foods. Friendly and collegiate atmosphere is what the Secretary of the SIU promised us, and friendly banter was present during the day. The first Brexit joke came when Mr Chris Parker started to explain to one presenter of the World Oncology federation why the UK was not included in the observation of deterioration of prostate cancer outcomes during the 2008 world recession, to which the presenter replied that it was only European countries in the paper. There was a mix of cheers and boos from the audience. However UK prostate cancer research, such as the PROMIS trial and the Emberton team studies were frequently quoted, as well as other British papers, with high esteem as corner stones of cancer research and advancing patient care.
Day 2 Friday
There was an early start for many who attended one of four optional instructional courses: each covered a different theme. I attended ‘management of priapism’ in view of its direct relevance to potential situations I may find myself in as an on call registrar. UCLH Consultants Asif Muneer and Guilio Garaffa hosted and gave clear information on acute management and surgical shunt techniques, plus imaging for more difficult cases, such as CT to exclude intra-abdominal cause of refractory priapism. The take home message was to consider early implantation of penile prosthesis if priapism lasts >72 hours. This was shown clearly on operative videos of prosthesis surgery at 3 weeks compared to 6 m; where the latter had penile fibrosis increasing surgical difficulty.
The first plenary session covered new advances in testicular cancer and another debate of focal therapy in intermediate prostate cancer. Scott Eggener presented a polished and compelling argument on why focal therapy could be the future, but Markus Graefen described his reluctance to accept it based on the research, limitations in MRI, and need for follow that is similar to active surveillance; but perhaps patient choice will drive us to make a conclusion. Fernando Secin described the low uptake of Active Surveillance within Argentina. This may be due to costs (both AS costs and costs lost by not operating) and lack of protocols; however, those clinicians who had undergone oncological training and worked in Academic centres were more likely to recommend AS.
Description of how Ebola affected our African colleagues and sadly mortality due to HSW highlights the breadth of education and world issues covered by the SIU congress. Winner of the SIU Astellas European Foundation Award, Dr John M Barry, described how five transplantation principles can be applied to urology. This included using life expectancy calculations, not age, in making decisions (he used his own Charlson comorbidity score to illustrate the point that it can be improperly used); he suggested using a quality of life grid and that practice guidelines, from numerous organisations use different grading systems thus he calls for unified, world scientific language.
I was invited to attend a ‘quick fire session for trainees’ where I met five experts and discussed career questions such as fellowships, choosing urology specialties and engaging with academia, which includes networking that we can practice during the conference. The experts were super friendly and one attendee was thrilled to meet Olivier Traxor who is his endourological hero.
Other sessions included the first session on ‘Professionalism in urology’ and included information on using Twitter and working with industry without compromising or influencing patient care by always practising evidence-based medicine. However, many researchers have ties to industry. Several tweets were shared during this session, for example:
Another session popular with trainees was ‘how to write a paper’ hosted by the World Journal of Urology.
Dan Wood from UCLH, UK chaired the session for congenital reconstruction, which included how to set up a service by Miss Claire Taylor; she emphasised the need to define the service you want to provide, decide which paediatric hospital you want to work with and having an excellent MDT and clinical specialist nurse, of which she is fortunate to have Winnie Nugent who works to bridge the gap between child and adult services.
The ‘Surgical Demo, session on Laparoscopy was well attended and the audience watched excellent videos from Karim Touijer on lap prostatectomy and Gonzalo Vitagliano on lap nephrectomy. The videos were clear and narration highlighted the relevant steps and anatomy. They emphasised the need to gain a mentor to reduce the learning curve and not attempt to set up a lap service solo. There was also an ‘encyclopaedic’ style Surgical Masters session of all types of prostate surgery for BPH that included surgical videos and tips/tricks.
Saturday
Many attended the sessions with a sore head on Saturday morning following the SIU Night party held at La Rural, a National Historic Landmark located in the Palermo district of Buenos Aires. It was inaugurated in the late 1800s in order to support and promote agricultural issues in Argentina. We were treated to typical foods: empanadas, freshly barbequed meats and sausages, breads and of course home grown wine. Entertainment was provided by Argentinian tango dancers and Argentine Gaucho dancers whose finale ended with Bolleadoras a dance that made hearts pound from the open male shirts, fast rhythm and the whirling ropes. Additionally, there was a photo booth for traditional Argentine dress, football snooker and a mechanical bull; luckily the only injury was an Australian trainee’s trousers.
The morning’s plenary session ‘Shifting sands – new technologies in stone disease’ covered a range of topics including retrograde intrarenal surgery by Mr Traxer. Mr Jorge Guitierrez highlighted the dangers of sepsis in stone disease; one key message included stopping stone surgery (including PCNL) when there was purulent urine. The panel agreed that 1-2cm stones fall in a grey area in the guidelines as to which treatment is the best. The majority of the panel favoured flexible ureteroscopy; but admitted that a patient’s ability to afford PCNL vs flexi URS and the surgeon’s skills and availability of equipment was what often governed practice rather than choice. Mariano Gonzalez described stone disease affecting pregnant women and the challenges of treating; interestingly he suggested that a low dose CT in the 2nd and 3rd trimester can be considered safe. Pradeep Rao informed us of the changing PCNL sizes and how the smaller ‘seeing needle scope’ at 4.8F enabled him to remove the stone in an infant less than one years old. Norberto Bernardo shared his experience with managing stones in complex patients, such as a case with severe scoliosis and another in a HSK. Mr Traxor made a plea that stents be used for the shortest time to reduce patient morbidity, i.e. as soon as they have been placed make a plan for ureteroscopy to enable stone treatment and removal.
The use of mesh for vaginal prolapse was debated by Nissrine Nakia (pro) and Paulo Palma (con). Palma highlighted the anatomy of the pelvic floor and the importance of identifying the level of deformity, which should then be used to select the right patients and select the correct procedure. The counter argument from Nakia started with a campaign slogan P.R.O.M.E.S.H in keeping with the ongoing US presidential debate. She stated that whilst the FDA did raise concerns regarding re-operation rates, there are now more modern meshes and are subjected to rigorous testing, plus experience has been gained regarding placement of mesh, post-mesh cystoscopy and use of oestrogen cream, which have all improved patient outcomes.
The European and Asian societies both presented in the plenary sessions. The EUA lecture, given by Arnulf Stenzl, described ongoing changes on how to improve TURBT, which included better training for juniors, including simulation, better visualisation (photo dynamic diagnosis) and the use of ‘bloc’ dissection with hybridknife to enable whole tumour removal in once piece, which can aid histological analysis.
Mr Foo from Singapore presented the UAA lecture on the subject of ‘holistic approach’ to care of BPH. Additionally that perhaps the Intro vesicular prostatic protrusion (IPP) tells us more about the likelihood of obstruction and when surgery would make the most difference.
Three parallel plenary sessions provided learning in the fields of spinal cord injury, paediatric urology and urological histology. The histology speakers had a tough job describing their field to us surgeons! The plenary session ‘SIU-ICD joint consultation on urological management of Spinal cord injury patients’ was well attended and covered the anatomy, surgical and non -surgical options, urodynamics and bladder emptying options. Speakers emphasised the need for Long-term follow-up, including upper tract imaging, blood tests (U&Es) and QOL questionnaires of which there are several. Each presenter clearly stated their recommendation and the level of evidence to support it. Tweets from this session included a commitment to reduce urine culture and treatment of UTI on asymptotic patients.
‘Ageing and urology’ session complemented the holistic theme as an expert panel discussed optimisation of elderly patients and the difficult decision making process of offering surgery in patients with frailty, high risk GA and delirium and co-morbidities. One panellist said it was about making a judgement that if the patient will appreciate the change and it will add to their QOL then age is not a barrier to operating; however, teamwork with anaesthetists and geriatrics is key to optimisation.
Each day a ‘Surgical Demo’ session’ ran, Saturday’s was on stones which was, like many stone sessions, full; Perhaps highlighting the enthusiasm towards Endourology. Pictured is Mr Guitierrez describing correct ureteroscopic hand manoeuvres and his ‘painting’ technique to dust stones. Additionally Mr Lojanapiwat from Thailand presented his operative experience in subcostal access for upper pole stones.
Throughout the afternoon were moderated poster sessions; from reducing laparoscopic camera fogging to comparison of traditional vs western medicine. These accepted abstracts were presented by urologists who were at varying stages of their careers. Presentations reflected high standards of research and a culmination of hard work. After watching some of the poster presentations I joined the urethral reconstruction ‘surgical tips’ session, which drew the biggest audience. The presentations offered high-quality operative pictures and complimentary radiology pictures showing the complexity of some of these strictures. Daniela Andrich from UCLH presented their experience of post-traumatic strictures and emphasised that the mechanism of injury correlates to the stricture pattern. Furthermore that partial ureteric injuries are probably under reported as they heal with the catheter in situ, sited by the trauma/orthopaedic team.
Sunday
The sun shone brightly on the last day of the conference and whilst many In the city were enjoying their Sunday lie in or preparing for church, conference delegates made their way to the last four early morning instructional courses. I attended ‘surviving prostate cancer’ chaired by Prof Mundy, which covered the aftermath of treatment for prostate cancer: fistulae, strictures, incontinence. Interestingly as our colleagues in General Surgery change techniques it provides new challenges relating to recto-vesical fistulae. It was recommended that MRIs should include sagittal views to best define the fistula anatomy. Prof Mundy described the difficulty that radiotherapy creates by scarring the tissues, which makes these patients more at risk of post-operative complications. This means it’s imperative to properly assess people prior to radiotherapy, including a cystoscopy to assess the bladder (and if applicable the post-prostatectomy anastomosis). Then consent the patient thoroughly prior to radiotherapy so that they’re aware of the more difficult surgery they face, should it be required.
The plenary session started with four speakers describing the emerging role of immunotherapy and specifically in cancers of the prostate, bladder and kidney. The research presented gave optimism of improving treatments for these cancers and that trials are ongoing and concluding. Fred Saad described how access to tissue can try to develop precision medicine; mutations specific to that tumour and patient could be assessed and tested in the laboratory so that treatment can be targeted and avoid treatments that don’t work.
A fierce debate regarding the role of varicocele surgery in the era of assisted reproduction ended in favour of offering surgery. Robert Brannigan presenting the ‘yes’ argument argued that varicocelectomy needs to be synergistic to assisted contraception, especially if time is of the essence in relation to maternal age. He gave evidence that varicocelectomy improves sperm quality for assisted conception and sees changes 3 months post-surgery. Alex Pastusak said he’d rather be ‘successful than lucky’ and was in favour of assisted contraception as the evidence for varicocelectomy, even the meta-analysis papers, has limitations so casts doubt on validity of available studies.
Rene Sotelo presented his endoscopic techniques for fistula repair, which included lap or robotic surgery within the bladder to remove the tract, create a plane between the bladder and surrounding tissues, place omentum or fascia between and then close the defect. We quickly moved from advanced techniques to trying to establish the basic technique with the next speaker. Alain Houlgate described his experience of establishing an endourological teaching programme between France and Senegal, which cumulates in a diploma.
Abstract prize winner Henry Woo presented his work on the International journal club #urojc where each month newly published articles are sent out to twitter followers and discussion generated. Unsurprisingly he was congratulated via twitter:
The last plenaries of the conference prior to further poster sessions included uroradiology, systemic cancer therapies and surgical demo on robotic cystectomy. The radiology session highlighted the advances in PSMA PET for prostate cancer recurrence but that TRUS still had a role.
River Plate Urological Meeting: representatives from the RSM – Urological section, UK, met with representatives from the Hospital Británicos in Rosario and Buenos Aires, Argentina and Montevideo, Uruguay. This is the first time these groups have met with the aim of collaboration and training. The day included presentations from the hospitals’ urology trainees, in English, on a range of topics and were marked as per the RSM marking criteria. The winning presentation was on ‘laparoscopic nephrectomy for living kidney donors’ and 2nd place for a presentation on ‘history of circumcision’. We had a tour of the hospital and were then welcomed into the British Embassy, to meet the Ambassador who is supportive of the relationships that are forming as a result of this meeting.
Concluding remarks
Overall the SIU was well organised, navigable and the incredible range of urology was well represented by experts in their field. The conference delegates were friendly, approachable and our host Buenos Aires warm and welcoming. Friendships and collaborations will undoubtedly continue beyond this congress.
The SIU Night was a particular highlight, showcasing the Argentine spirit in one evening for those who weren’t staying long in the country. The programme used varied formats and operative videos shown were generally of good quality. The presentations were of good calibre and the research presented both new and established. Reference was often made to EAU and AUA guidelines and international papers from a range of journals, in particular BJUI, Eur Urol and J Urol. The meeting of minds is certainly healthy to urological progress and exchanging ideas is key to innovation and improvement within our specialty across the world. There is so much we can learn from each other.
Adios SIU 2016! and ‘Até logo’ SIU 2017 Portugal!
Sophie Rintoul-Hoad is a urology trainee in the South Thames Deanery, currently working at King’s College hospital. She attended the SIU 2016 conference in Buenos Aires and then saw some of Argentina’s highlights, including a few days at El Venado Estancia playing polo and learning how to be a gaucho!
Every Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
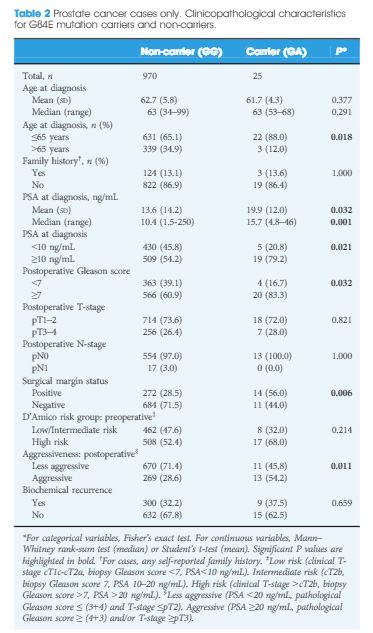
Prevalence of the HOXB13 G84E mutation in Danish men undergoing radical prostatectomy and its correlations with prostate cancer risk and aggressiveness
To determine the prevalence of the HOXB13 G84E mutation (rs138213197) in Danish men with or without prostate cancer (PCa) and to investigate possible correlations between HOXB13 mutation status and clinicopathological characteristics associated with tumour aggressiveness.
Materials and Methods
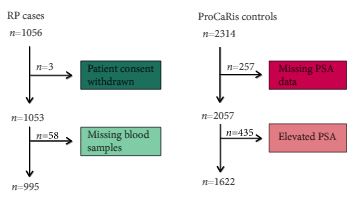
We conducted a case–control study including 995 men with PCa (cases) who underwent radical prostatectomy (RP) between 1997 and 2011 at the Department of Urology, Aarhus University Hospital, Denmark. As controls, we used 1622 healthy men with a normal prostate specific antigen (PSA) level.
Results
The HOXB13 G84E mutation was identified in 0.49% of controls and in 2.51% of PCa cases. The mutation was associated with a 5.12-fold increased relative risk (RR) of PCa (95% confidence interval [CI] 2.26–13.38; P = 13 × 10−6). Furthermore, carriers of the risk allele were significantly more likely to have a higher PSA level at diagnosis (mean PSA 19.9 vs 13.6 ng/mL; P = 0.032), a pathological Gleason score ≥7 (83.3 vs 60.9%; P = 0.032), and positive surgical margins (56.0 vs 28.5%; P = 0.006) than non-carriers. Risk allele carriers were also more likely to have aggressive disease (54.2 vs 28.6%; P = 0.011), as defined by a preoperative PSA ≥20 ng/mL, pathological Gleason score ≥ (4+3) and/or presence of regional/distant disease. At a mean follow-up of 7 months, we found no significant association between HOXB13mutation status and biochemical recurrence in this cohort of men who underwent RP.
Conclusions
This is the first study to investigate the HOXB13 G84E mutation in Danish men. The mutation was detected in 0.49% of controls and in 2.51% of cases, and was associated with 5.12-fold increased RR of being diagnosed with PCa. In our RP cohort, HOXB13 mutation carriers were more likely to develop aggressive PCa. Further studies are needed to assess the potential of HOXB13 for future targeted screening approaches.
For the first time, Storebjerg et al. [1] describe the prevalence of the HOXB13 G84E mutation in a Danish population and its association with prostate cancer risk and features indicative of clinically aggressive disease in a cohort of men undergoing radical prostatectomy. In this study, the prostate cancer risk mutation was seen in 0.49% of controls with an ~5-fold increase in risk of prostate cancer among carriers. The homeobox transcription factor gene HOXB13, is located on the long arm of chromosome 17 (17q21), and belongs to a superfamily of genes considered critical to animal embryonic development, characterised by a highly-conserved DNA-binding domain. In 2012, our research team described the association of a rare recurrent HOXB13 mutation, substituting adenine for guanine in the second position of codon 84 resulting in the replacement of glycine by glutamic acid, with prostate cancer and found that the carrier frequency was ~20-times higher among men with early onset disease and multiple affected close relatives compared with men presumed without disease [2]. Since then, numerous studies have confirmed this association with estimates of risk overall varying from ~3 to 9-fold, and generally a greater risk seen among men diagnosed before the age of 60 years and among those with a positive family history of disease among first-degree relatives [3]. The G84E mutation is almost exclusively found in men of Northern European descent with evidence suggesting that it is a relatively recent (circa 1790s) founder mutation in the population, and considered to be of moderate penetrance (estimated lifetime risk among carriers 35–65%) [4]. The same germline mutation has also been preliminarily reported to be associated with cancers of the breast, colon, bladder, and leukaemia, but requires further investigation [5, 6].
The findings from this study [1], both for the prevalence of the mutation, as well as its magnitude of association with prostate cancer, are comparable to prior reports in Northern European populations. Furthermore, among the 995 cases, the mutation frequency was significantly associated with features predictive of progression after surgery (high PSA level, positive surgical margins, higher pathological Gleason score, and non-organ confined disease) suggesting that genetic evaluation of men with a strong family history would identify a subset of men that would benefit from early screening and intervention in the same manner as are male carriers of known founder mutations in BRCA2[7]. The observation between HOXB13 and clinical features indicative of aggressive disease has been less consistent compared with studies of risk overall and the exact mechanism whereby the gene contributes to malignant progression in the prostate is not well-understood. There is some suggestion that the gene may operate both as a tumour suppressor, as early studies reported its suppression of androgen receptor activity, and as an oncogene as HOXB13 overexpression has been seen in androgen-independent tumours [8].
Currently, most countries (including the USA) do not recommend use of PSA screening for men at average risk for prostate cancer. However, given the significant risk of prostate cancer in men carrying a single copy of the HOXB13 G84E allele, should these male mutation carriers be screened for prostate cancer with PSA testing and DRE? If so, how do we identify these men and at what age should testing commence? Unfortunately, many G84E carriers may not be identified by family history, which raises the question about when is the risk of disease significant enough to warrant population level testing? As Nordic countries, including Denmark, have a higher frequency of HOXB13 G84E allele in the general population, research directed toward understanding the benefit of genetic testing followed by prostate cancer early detection strategies should be considered.
Every Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Predictive value of negative 3T multiparametric magnetic resonance imaging of the prostate on 12-core biopsy results
James S. Wysock, Neil Mendhiratta, Fabio Zattoni, Xiaosong Meng, Marc Bjurlin,
William C. Huang, Herbert Lepor, Andrew B. Rosenkrantz* and Samir S. Taneja
Department of Urology, and *Department of Radiology, NYU Langone Medical Center, New York, NY, USA
To evaluate the cancer detection rates for men undergoing 12-core systematic prostate biopsy with negative prebiopsymultiparametric magnetic resonance imaging (mpMRI) results.
Materials and Methods
Clinical data from consecutive men undergoing prostate biopsy who had undergone prebiopsy 3T mpMRI from December 2011 to August 2014 were reviewed from an institutional review board-approved prospective database. Men with negative prebiospy mpMRI results (negMRI) before biopsy were identified for the present analysis. Clinical features, cancer detection rates and negative predictive values were summarized.
Results
Seventy five men with negMRI underwent systematic 12-core biopsy during the study period. In the entire cohort, men with no previous biopsy, men with previously negative biopsy and men enrolled in active surveillance protocols, the overall cancer detection rates were 18.7, 13.8, 8.0 and 38.1%, respectively, and the detection rates for Gleason score (GS) ≥7 cancer were 1.3, 0, 4.0 and 0%, respectively. The NPVs for all cancers were 81.3, 86.2, 92.0, and 61.9, and for GS ≥7 cancer they were 98.7, 100, 96.0 and 100%, respectively.
Conclusions
A negative prebiopsy mpMRI confers an overall NPV of 82% on 12-core biopsy for all cancer and 98% for GS ≥7 cancer. Based on biopsy indication, these findings assist in prebiopsy risk stratification for detection of high-risk disease and may provide guidance in the decision to pursue biopsy.
A test to exclude the presence of aggressive prostate cancer would be highly desirable. In the article by Wysock et al. [1], the authors examine pathological results in 75 men who underwent 12-core systematic biopsy using the Artemis device; all had a pre-biopsy MRI showing no suggestion of cancer. In 74 patients no cancer with Gleason score ≥7 was found on biopsy, which translates into a remarkable 98.7% negative predictive value (NPV) for potentially aggressive disease. The implication is that virtually all serious prostate cancers can be seen on MRI, and thus a negative MRI obviates the need for a biopsy. If this finding were to be confirmed, the majority of prostate biopsies could be avoided, a truly laudable goal.
Another reason why a ‘negative’ MRI should not always negate the need for biopsy relates to the current proliferation of prostate MRI studies. Many of the new MRI studies are being performed and interpreted by radiologists not adequately trained in this niche. Despite attempts at standardisation [3], the variability of MRI readings, from place to place and from one radiologist to another, can be remarkable. In the recent past I have seen lesions called Prostate Imaging-Reporting and Data System (PI-RADS) Grade 5 ‘disappear’ when scrutinised by more-experienced readers; the reverse has also been seen. Even among expert readers using the latest Version 2 of PI-RADS, agreement in prostate MRI interpretation is only moderate at best (κ ≈0.5) [4]. Therefore, widely varying interpretations of prostate MRI can be expected for the near-term future. A formal training programme and certification in MRI interpretation, which is sorely needed, has not yet been established.
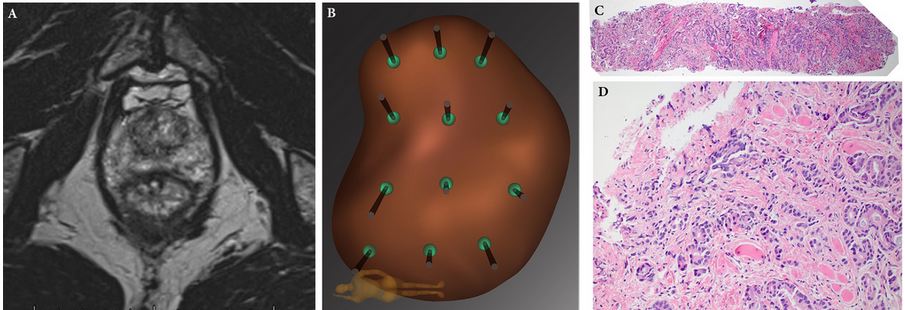
Figure 1: Example of falsely negative MRI. Patient was a Caucasian male (PSA level 3.8 ng/mL) aged 68 years, who on a previous conventional biopsy was found to have a microfocus of Gleason 3 + 3 = 6 prostate cancer. He was considered for active surveillance, and multiparametric MRI of prostate was obtained (A): prostate volume was found to be 35 mL; no region of interest was identified. Mapping biopsy was performed by following the 12-point template of the Artemis device (B). A tissue core from the left lateral apex revealed 6 mm of Gleason 3 + 5 = 8 prostate cancer (C, ×4; D, ×20). Radical prostatectomy was performed, revealing a tumour on the left side of the prostate with diameters of 15 × 12 × 9 mm. Falsely negative MRI is not uncommon. When biopsy is clinically indicated, a negative MRI should not preclude mapping biopsy. Reproduced with permission from Nassiri et al., 2015 [1].
Professor and deKernion Endowed Chair, Department of Urology, David Geffen School of Medicine at UCLA, Los Angeles, CA, USA
1 Wysock JS, Mendhiratta N, Zattoni F et al. Predictive value of negative 3T multiparametric magnetic resonance imaging of the prostate on 12-core biopsy results. BJU Int 2016; 118: 515–20
2 Nassiri N, Natarajan S, Margolis DJ, Marks LS. Targeted prostate biopsy: lessons learned midst the evolution of a disruptive technology. Urology 2015; 86: 432–8
3 Weinreb JC, Barentsz JO, Choyke PL et al. PI-RADS Prostate Imaging – Reporting and Data System: 2015, Version 2. Eur Urol 2016; 69: 16–40
4 Rosenkrantz AB, Ginocchio LA, Cornfeld D et al. Inter-observer reproducibility of the PI-RADS Version 2 Lexicon: A multi-center study of six experienced prostate radiologists. Radiology 2016; 280: 793–804
5 Filson CP, Natarajan S, Margolis DJ et al.Prostate cancer detection with magnetic resonance-ultrasound fusion biopsy: The role of systematic and targeted biopsies. Cancer 2016; [Epub ahead of print]. doi: 10.1002/cncr.29874
6 Le JD, Tan N, Shkolyar E et al. Multifocality and prostate cancer detection by multiparametric magnetic resonance imaging: correlation with whole-mount histopathology. Eur Urol 2015; 67: 569–76
7 Palapattu GS, Cani AK, Huang J et al. Progression of low- to high-grade prostate cancer: Molecular profiling of tissue obtained by serial targeted biopsy. J Clin Oncol 2015; 33 (Suppl.): Abstract 501
The widely anticipated results of the ProtecT study have now been published. Unfortunately, the results do little to advance our understanding as to whether surgery or radiation provides better outcomes.
In summary
The study followed oncologic and functional outcomes of 545 patients randomized to active monitoring (surveillance), 553 to radical prostatectomy, and 545 to radiotherapy. With a median follow-up of 10 years, the authors report no significant differences in prostate cancer specific (p=0.48) or overall survival (p=0.87) among the three treatment groups. They did demonstrate an increase in disease progression and metastasis among men managed with surveillance.
In an accompanying manuscript, the authors examined patient reported outcome measures out to 6 years following treatment. The authors report worse urinary continence and erectile function following surgery and worse voiding symptoms and bowel function following radiotherapy.
What do we take from this?
The investigators and participating patients should be congratulated for successfully completing this study. Numerous authors have documented their failure to adequately accrue to randomized studies of surgery versus radiotherapy in localized prostate cancer (including MRC PR06 and SPIRIT). The failure of these trials, among others, prompted Dr. Wilt to ask “Can randomized treatment trials in early stage prostate cancer be completed?” These authors have unequivocally proven that the answer is “yes”.
However, there are many caveats in applying these results to our patients:
(1) Study power
The study was clearly underpowered to evaluate the primary outcome of prostate-cancer specific mortality. Drs. Roobol and Bokhorst eloquently described important limitations of the ProtecT study. The authors designed the study assuming prostate cancer mortality of 15% at a median follow-up of 10 years. This was later adjusted downwards to 10% based on updated UK data. In the end, rates were closer to 1%. The conclusions of the primary analysis are based on a total of 17 (17!!) deaths.
(2) Study cohort – enriched with low risk disease
Among the randomized patients, the median PSA was 4.6 ng/mL, 76% had clinical stage T1c disease, and 77% had Gleason score 6 disease. These patients would almost certainly be considered most suitable for active surveillance, rather than active therapy, if seen in clinic today. Clinically meaningful decisions between surgery and radiotherapy are in the realm of treatment of intermediate and high-risk localized prostate cancer and these comprise a small group in this study. Based on this baseline distribution, it will be unlikely that any significant differences will be found in future follow-up studies.
(3) Outcomes for active surveillance
Perhaps the most notable findings of this study involve the significantly higher rates of progression, metastasis and prostate cancer specific mortality for patients treated on the surveillance protocol as compared to those treated actively, though statistical significance was not reached for PCSM. The manuscript does not provide further details regarding the pathologic characteristics of these patients. Relevantly, what was the Gleason score for these patients? This is of particularly importance as many surveillance proponents are advocating an expanding role of AS.
(4) Treatments administered
RCTs typically require significant periods of accrual, follow-up and analysis. As a result, they may be out of date prior to completion. This is certainly true of the ProtecT study. This most prominently affects patients allocated to radiotherapy. In the study protocol, patients received 3D conformal radiotherapy at 74 Gy, not the IMRT which has now become widely used. Thus, proponents of radiotherapy will likely to discount any findings which do not favour radiotherapy.
In addition, the current day relevance of the surgical treatment provided is questionable. First, the vast majority of patients in the surgical arm underwent open RP. More concerning is the quality of surgery provided: 93 patients (24%) of the cohort had positive surgical margins. In contemporary series, the average rate is under 15% with centers of excellence approaching 5%. While PSM rates clearly affect oncologic outcomes, they likely are also a surrogate of surgical quality which may affect functional outcomes.
(5) Comparison of active treatments
In the accompanying editorial, Dr. D’Amico comments on a “trend favouring radiation and ADT over surgery” and suggests that “one may consider radiation and ADT as a preferred option”. The basis for this conjecture is 5 deaths in the surgery group and 4 in the radiotherapy group, hardly a convincing sample. In contrast to these data, there was a higher number of patients with metastasis among those treated with radiotherapy (16 vs 13). These discordant results would certainly suggest that any preference for radiotherapy is premature. Indeed, with additional follow-up one would expect the patients with metastasis to die of prostate cancer, thus favouring those treated surgically.
On a methodological note, while the inclusion of active surveillance is a strength of the study, it poses analytic difficulties. The primary analysis assesses a null hypothesis assuming equality across all study interventions. Thus, as this was non-significant, pairwise testing of surgery and radiotherapy, and each with surveillance, is inappropriate and conclusions on these comparisons should not be drawn.
(6) Functional outcomes and treatment-related complications
Most clinicians are well aware that many complications other than erectile function and urinary incontinence may affect that life trajectory of patients following prostate cancer treatments. ProtecT offers the opportunity to examine the risks of secondary malignancy, repeat urologic and gastrointestinal interventions, surgeries and hospitalizations following treatment. However, these are not currently included in the published data.
Further, the PCOS studies have clearly shown that differences in patient reported urinary, sexual and bowel function change over time with convergence after long term follow-up (15 years). With ongoing maturity, it will be interesting to see if a similar pattern emerges in ProtecT.
In conclusion
The ProtecT study may raise more questions than it answers. Among a low risk group of patients, it has shown that active treatment of PSA-detected prostate cancer can reduce the progression to metastatic disease. Assessment of prostate cancer specific and overall mortality, as well as the comparative efficacy of surgery and radiotherapy, is not possible due to power limitations.
Will you be changing you patient counselling based on these results?
Christopher Wallis, MD
Resident,
Division of Urology,
Department of Surgery,
University of Toronto
Doctoral Student in Clinical Epidemiology and Health Care Research, Institute of Health Policy, Management & Evaluation
University of Toronto
Robert Nam, MD MSc FRCSC
Ajmera Family Chair in Urologic Oncology
Professor,
Division of Urology,
Department of Surgery
University of Toronto
Head, Genitourinary Cancer Site
Odette Cancer Centre
Sunnybrook Health Sciences Centre
After briefly venturing to tropical Cairns in 2015, the Asia-Pacific Prostate Cancer Conference returned to its traditional home in Melbourne for its 17th edition in 2016 (#APCC16). The meeting has previously featured the who’s who of prostate cancer and this year was no different with an all-star multidisciplinary faculty consisting of 18 international members in addition to our local experts. The meeting was well attended by over the 750 delegates from all parts of the globe and remains one of the largest prostate cancer educational events worldwide.
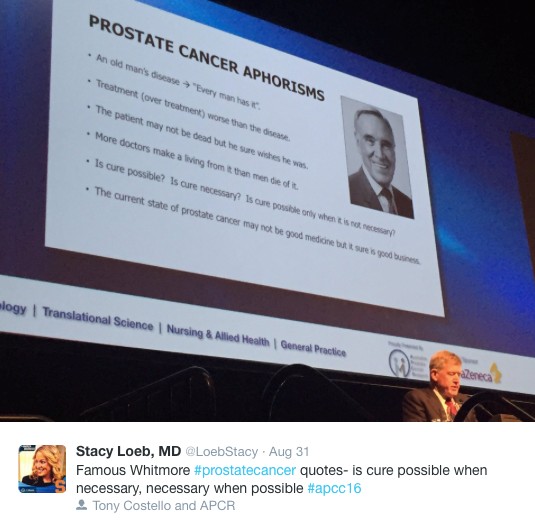
Conference president Professor Tony Costello opened the conference with the famous Whitmore aphorisms and outlined the impressive progress and discoveries we have made in the field over the last century. The first case of prostate cancer was described in 1853 in the London Hospital and was noted by the surgeon to be a “very rare disease” whereas now it is known to be the most commonly diagnosed malignancy amongst men. Pleasingly, research and emphasis on men’s health has grown with the disease highlighted by the newly completed, world-class Parkville Biomedical precinct in Melbourne, which includes “The Royal Men’s Hospital” (@APCR). Melbourne’s Lord Mayor (@LordMayorMelb) also dropped-by to reiterate his support for the meeting and the advancements made in men’s health.
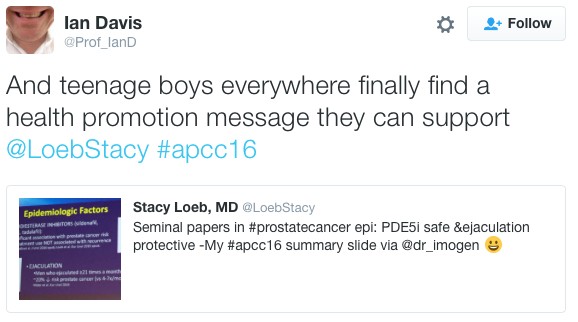
In what is becoming an annual tradition, honourary Melbournian and Australian, Dr Stacy Loeb (@LoebStacy) once again got the sessions off to a flying start by delivering the ‘prostate cancer year in review’ which was an excellent overview of the abstracts produced over the last 12 months. The male attendees in particular were excited by the recent paper suggesting that more than 21 ejaculations per month acted as a protective factor for the development of prostate cancer. Although confounding factors may have played a role in the association seen, these were easily over-looked and its results were accepted as gospel and promoted as a public health message. The abstract featured the following day on the home page of The Australian Financial Review (https://www.afr.com/lifestyle/health/mens-health/tell-your-partner-frequency-counts-even-against-cancer-20160831-gr5fs4) – who knew that the answer to the world economic problems was so simple!
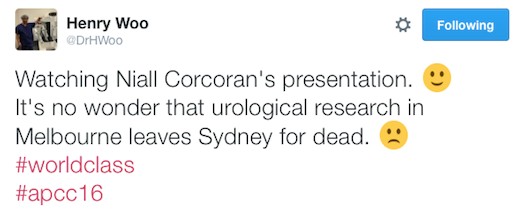
The meeting did however become more scientific as we heard from a range of international and local experts on the challenges of trying to find the balance of precision oncology in a time of tumour heterogeneity. It was clear that the future has arrived with recent advances in the field of genomics and biomarkers. These discoveries appear to be only the tip of the iceberg and further research holds the key in understanding tumour behavior in order to tailor treatment on a patient-to-patient level. Having witnessed a variety of experts from all parts of the globe present their finding there is little doubt that a major breakthrough is just around the corner. A special mention to Dr Niall Corcoran whose research was of such high quality that A/Prof Henry Woo (@DrHWoo) raised the white flag early in the Melbourne vs. Sydney inter-city rivalry.
The named lectures of #APCC16 were highlights of the conference. Keeping with the theme of the first morning, Dr Martin Gleave delivered the 4th Patrick C Walsh lecture titled ‘Two Tales of Precision Oncology.” Prof Peter Wiklund gave the inaugural ERUS lecture on the role of surgery for high risk and metastatic prostate cancer.
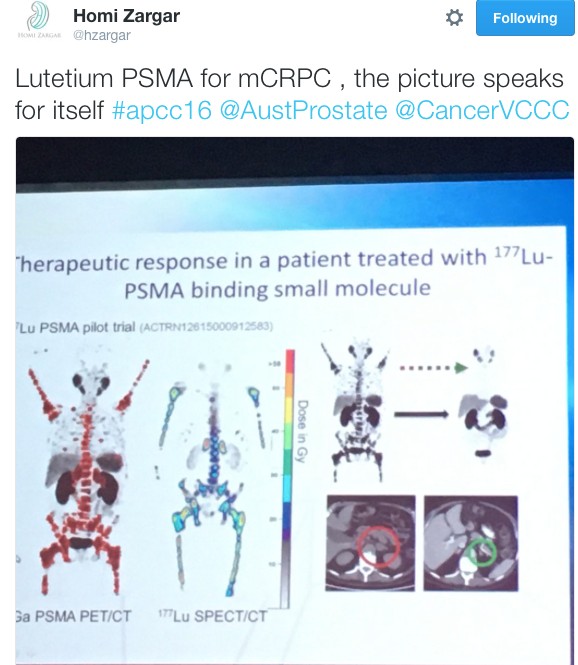
It wouldn’t have been a prostate cancer conference without the age-old debate of surgery vs. radiotherapy being revisited. Over three days Dr Robert Nam presented a series of talks on Canadian long-term outcomes and meta-analysis showing favourable results for team surgery. He also predicted that the highly anticipated ProtecT randomised trial due in the NEJM would show no difference ensuring the debate prolongs into the future and vowed to “eat my shorts” if the trial demonstrated a result favouring either modality. Dr John Violet flew the flag strongly for radiation oncologists in presenting the promising outcomes for 177Lu-PSMA in the mCRPC setting. Similarly, Dr Andrew Kneebone presented a compelling case for stereotactic radiation for oligometastatic disease.
Imaging of the prostate was a hot topic throughout the conference. The excitement around PSMA-PET was at a climax following The Victorian Comprehensive Cancer Centre’s (@VCCC) experience that was presented by Associate Professors Michael Hofman (@DrMHofman) and Nathan Lawrentschuk (@lawrentschuk). The proceeding panel discussion focused on how to best utilise the technology and the role it currently plays in the prostate cancer landscape. Despite not being FDA approved, its role in evaluating recurrence appears to be entrenched with data to support its superiority over other modalities but it was also proposed that it might have a place in initial staging of high-risk cancer. The advancement of PSMA over conventional imaging also raised the question of how we now interpret previous trials such as CHAARTED and STAMPEDE whose results are based on superseded technology.
The hype surrounding PSMA-PET only just eclipsed that of mpMRI in the imaging landscape. Professor Philip Stricker presented a nomogram, which integrated MRI in determining who to biopsy and Dr Rob Reiter reported a terrific novel study of using 3D modeling to compare MRI results to final histopathology to determine correlation but did caution us with performing targeted biopsies alone which risks missing clinically significant cancers. Dr Nam also chimed in with a pilot study of using MRI as a screening test.
Suspense was built until Friday for the highly anticipated session on open vs. robotic surgery featuring the first presentation of the Brisbane RCT. The results of the trial have been already widely debated in the urological community and a discussion similar to the recent BJUI blog (https://www.bjuinternational.com/bjui-blog/its-not-about-the-machine-stupid/) ensued. Regardless of individual opinions on the trial, there is no dispute about the volume of work required to conduct a surgical randomised trial and there was wide praise for the efforts of the Brisbane team. Prof Peter Wiklund and Dr Homi Zargar (@hzargar) also reported the Swedish and Victorian experience respectively. The overall consensus was that robotic surgery offers the benefit of minimally invasive surgery but it is the surgeon rather than the modality, which has the most significant impact on outcomes.
There was a strong multi-disciplinary theme throughout the conference. The Nursing & Allied Health and Translational Science streams both had strong contingents attending. The quality of research presented and engagement amongst attendee was of the highest standard. This was exemplified by the session ‘MDT 2020’, which was a case-centred discussion by a panel of experts from a variety of professions and highlighted the value of a multidisciplinary approach in patient care.
The social program of #APCC16 was not overshadowed by its academic counterpart. The conference dinner was held at The Glasshouse where the food was exquisite and entertainment was provided by three waiters come tenors. Their classical renditions were received by guests with napkin twirling and swinging wine glasses. The frivolities were thoroughly enjoyed by all.
We would like to congratulate all attendees and their teams on the abstracts presented throughout the conference. The BJUI once again proudly supported the meeting with all accepted abstracts published in a special supplements issue and BJUI Associate Editors Declan Murphy (@declanmurphy), John Davis, and Nathan Lawrentschuk being prominent figures throughout the conference. A special mention to the poster prize winners from this year:
Clinical Urology: Jonathan Kam – Do multi-parametric MRI guided biopsies add value to the standard systematic prostate needle biopsy? – early experience in an Australian regional centre
Nursing & Allied Health: Thea Richardson – An Androgen Deprivation Therapy Clinic: An integrative approach to treatment
Translational Science: Natalie Kurganovs – Identifying the origins and drivers of castration resistant prostate cancer
On behalf of all the delegates, we thank the entire international and local faculty who shared their knowledge over the conference and devote their time to improving men’s health. Furthermore, meetings such as this would not occur without the unheralded behind the scenes work. We extend our thanks to president Prof Costello, the convenors of the streams (A/Prof Declan Murphy, Dr Niall Corcoran, A/Prof Chris Hovens, Ms Helen Crowe (@helenrcrowe) & Mr Dave Gray (@DavidGrayAust)) and the APCC committee. We also graciously thank our sponsors without whom none of this would be possible and are vital to further advancements in men’s health.
Last but not least, given the rich history of social media seen at this conference, it would be remiss not to acknowledge another #SoMe landmark. Melbourne has previously been responsible in welcoming urology SoMe royalty, Dr Stacy Loeb, to the twitter world and this year the twitterati were introduced to Dr Peter Carroll (@pcarroll_). He managed to send out 4 tweets and eclipse 100 followers before the end of the conference.
#APCC17 will return to Melbourne on 30th of August 2017 – we hope to see you there!
Dr Niranjan Sathianathen (@NiranjanJS) is a researcher at Peter MacCallum Cancer Centre, Melbourne.