What’s the Diagnosis?
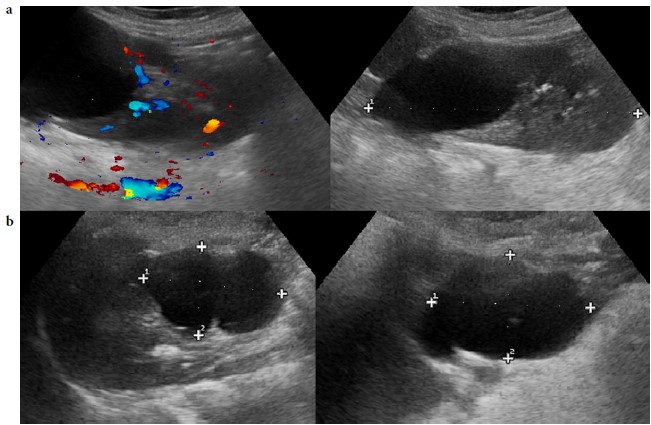
These images are taken from Esposito et al, BJUI 2017. The data in the questions is from this paper. These show 2 children who have undergone laparoscopic partial nephrectomy (LPN).
No such quiz/survey/poll

These images are taken from Esposito et al, BJUI 2017. The data in the questions is from this paper. These show 2 children who have undergone laparoscopic partial nephrectomy (LPN).
No such quiz/survey/poll
Every Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video from Mr. Jim Adshead, discussing his paper.
If you only have time to read one article this week, it should be this one.
To evaluate postoperative health resource utilisation and secondary care costs for radical prostatectomy and partial nephrectomy in National Health Service (NHS) hospitals in England, via a comparison of robot-assisted, conventional laparoscopic and open surgical approaches.
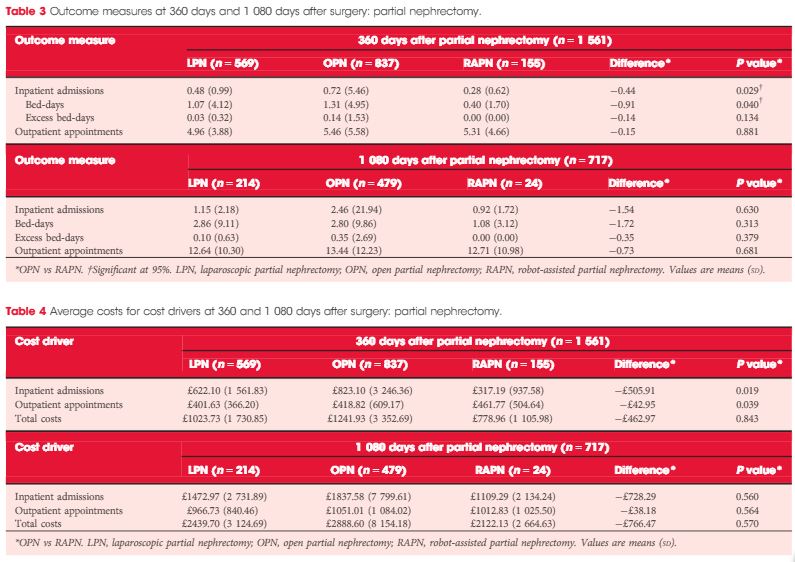
We retrospectively analysed the secondary care records of 23 735 patients who underwent robot-assisted (RARP, n = 8 016), laparoscopic (LRP, n = 6 776) or open radical prostatectomy (ORP, n = 8 943). We further analysed 2 173 patients who underwent robot-assisted (RAPN,n = 365), laparoscopic (LPN, n = 792) or open partial nephrectomy (OPN, n = 1 016). Postoperative inpatient admissions, hospital bed-days, excess bed-days and outpatient appointments at 360 and 1 080 days after surgery were reviewed.
Patients in the RARP group required significantly fewer inpatient admissions, hospital bed-days and excess bed-days at 360 and 1 080 days than patients undergoing ORP. Patients undergoing ORP had a significantly higher number of outpatient appointments at 1 080 days. The corresponding total costs were significantly lower for patients in the RARP group at 360 days (£1679 vs £2031 for ORP; P < 0.001) and at 1 080 days (£3461 vs £4208 for ORP; P < 0.001). In partial nephrectomy, Patients in the RAPN group required significantly fewer inpatient admissions and hospital bed-days at 360 days compared with those in the OPN group; no significant differences were observed in outcomes at 1 080 days. The corresponding total costs were lower for patients in the RAPN group at 360 days (£779 vs £1242 for OPN,P = 0.843) and at 1 080 days (£2122 vs £2889 for ORP; P = 0.570). For both procedure types, resource utilisation and costs for laparoscopic surgeries lay at the approximate midpoint of those for robot-assisted and open surgeries.
Our analysis provides compelling evidence to suggest that RARP leads to reduced long-term health resource utilisation and downstream cost savings compared with traditional open and laparoscopic approaches. Furthermore, despite the limitations that arise from the inclusion of a small sample, these results also suggest that robot-assisted surgery may represent a cost-saving alternative to existing surgical options in partial nephrectomy. Further exploration of clinical cost drivers, as well as an extension of the analysis into subsequent years, could lend support to the wider commissioning of robot-assisted surgery within the NHS.
The introduction of the daVinci robotic surgical system (Intuitive Surgical, Sunnyvale, CA, USA) has led to a continuous discussion about the cost-effectiveness of its use. The capital costs and extra costs per procedure for robot-assisted procedures are well known, but there are limited data on healthcare consumption in the longer term. In this issue of BJUI, a retrospective study investigated the NHS-registered, relevant care activities up to three years after surgery comparing robot-assisted, conventional laparoscopic, and open surgical approaches to radical prostatectomy and partial nephrectomy [1].
The robotic system is particularly useful in difficult to perform laparoscopic surgeries, which are easier to perform with the daVinci system due to improved three-dimensional vision, ergonomics, and additional dexterity of the instruments. Because the use of the robotic system is more costly, to justify its use the outcomes for patients should be improved. Therefore, more detailed information about the clinical and oncological outcomes, as well as the incidence of complications after surgery with the daVinci system, is needed.
Lower rates of positive surgical margins for robot-assisted radical prostatectomy (RARP) vs open and laparoscopic RP have been reported [2]. There also is evidence of an earlier recovery of functional outcomes, such as continence. RARP is associated with improved surgical margin status compared with open RP and reduced use of androgen-deprivation therapy and radiotherapy after RP, which has important implications for quality of life and costs. Ramsay et al. [3] reported that RARP could be cost-effective in the UK with a minimum volume of 100–150 cases per year per robotic system.
Centralisation of complex procedures will not only result in better outcomes, but also facilitate optimal economical usage of expensive medical devices. Furthermore, the skills learned to perform the RARP procedure can be used during other procedures, such as robot-assisted partial nephrectomy (RAPN) and radical cystectomy (RARC). The recent report by Buse et al. [4] confirms that RAPN is cost-effective in preventing perioperative complications in a high-volume centre, when compared with the open procedure. Minimally invasive techniques for complex procedures, such as a RC, take more time to perform, but result in less blood loss. A systematic review by Novara et al. [5] showed a longer operation time for RARC, but fewer transfusions and fewer complications compared with open surgery. However, there is no solid evidence about the cost-effectiveness of this technique to date. The RAZOR trial (randomised trial of open versus robot assisted radical cystectomy, DOI: 10.1111/bju.12699) is likely to provide some answers about differences in cost, complications, and quality of life when the results of the study become available later this year.
Additionally, the robotic system has been shown to shorten the learning curve of complex laparoscopic procedures in simulation models [6]. Recently, a newly structured curriculum to teach RARP has been validated by the European Association of Urology-Robotic Urology Section [7]. The effect of the shorter learning curve on the cost of the procedures has not yet been well studied for cost-effectiveness. However, due to the shorter learning curves, patients have lower risks of complications, which from the patients’ perspective is more important than any increased costs.
The study reported in this issue [1]; however, does not include the ‘out of pocket’ expenses of patients, it does not report on the differences in patient and tumour characteristics, and outcomes such as complications and oncological safety. These issues are all challenges to be addressed in a thorough prospective (randomised) trial on the cost-effectiveness of the use of robot-assisted surgery, including quality-of-life measurements and complications of the surgical procedures. In the Netherlands the RACE trial (comparative effectiveness study open RC vs RARC, www.racestudie.nl) started in 2015 and the results are expected in 2018–2019.
To evaluate postoperative health resource utilisation and secondary care costs for radical prostatectomy and partial nephrectomy in National Health Service (NHS) hospitals in England, via a comparison of robot-assisted, conventional laparoscopic and open surgical approaches.
We retrospectively analysed the secondary care records of 23 735 patients who underwent robot-assisted (RARP, n = 8 016), laparoscopic (LRP, n = 6 776) or open radical prostatectomy (ORP, n = 8 943). We further analysed 2 173 patients who underwent robot-assisted (RAPN,n = 365), laparoscopic (LPN, n = 792) or open partial nephrectomy (OPN, n = 1 016). Postoperative inpatient admissions, hospital bed-days, excess bed-days and outpatient appointments at 360 and 1 080 days after surgery were reviewed.
Patients in the RARP group required significantly fewer inpatient admissions, hospital bed-days and excess bed-days at 360 and 1 080 days than patients undergoing ORP. Patients undergoing ORP had a significantly higher number of outpatient appointments at 1 080 days. The corresponding total costs were significantly lower for patients in the RARP group at 360 days (£1679 vs £2031 for ORP; P < 0.001) and at 1 080 days (£3461 vs £4208 for ORP; P < 0.001). In partial nephrectomy, Patients in the RAPN group required significantly fewer inpatient admissions and hospital bed-days at 360 days compared with those in the OPN group; no significant differences were observed in outcomes at 1 080 days. The corresponding total costs were lower for patients in the RAPN group at 360 days (£779 vs £1242 for OPN,P = 0.843) and at 1 080 days (£2122 vs £2889 for ORP; P = 0.570). For both procedure types, resource utilisation and costs for laparoscopic surgeries lay at the approximate midpoint of those for robot-assisted and open surgeries.
Our analysis provides compelling evidence to suggest that RARP leads to reduced long-term health resource utilisation and downstream cost savings compared with traditional open and laparoscopic approaches. Furthermore, despite the limitations that arise from the inclusion of a small sample, these results also suggest that robot-assisted surgery may represent a cost-saving alternative to existing surgical options in partial nephrectomy. Further exploration of clinical cost drivers, as well as an extension of the analysis into subsequent years, could lend support to the wider commissioning of robot-assisted surgery within the NHS.