
Podcast: Survival following cytoreductive nephrectomy: a comparison of existing prognostic models
Part of the BURST/BJUI Podcast Series
Mr Kenneth MacKenzie MBChB, FRCS (Urol) is a ST7 in Urology in North East England and BURST committee member.

Mr Kenneth MacKenzie MBChB, FRCS (Urol) is a ST7 in Urology in North East England and BURST committee member.

Every month, the Editor-in-Chief selects an Article of the Month from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an editorial written by a prominent member of the urology community and a video prepared by the authors; we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
To apply the standard PADUA and RENAL nephrometry score variables to three‐dimensional (3D) virtual models (VMs) produced from standard bi‐dimensional imaging, thereby creating 3D‐based (PADUA and RENAL) nephrometry scores/categories for the reclassification of the surgical complexity of renal masses, and to compare the new 3D nephrometry score/category with the standard 2D‐based nephrometry score/category, in order to evaluate their predictive role for postoperative complications.
All patients with localized renal tumours scheduled for minimally invasive partial nephrectomy (PN) between September 2016 and September 2018 underwent 3D and 2D nephrometry score/category assessments preoperatively. After nephrometry score/category evaluation, all the patients underwent surgery. Chi‐squared tests were used to evaluate the individual patients’ grouping on the basis of the imaging tool (3D VMs and 2D imaging) used to assess the nephrometry score/category, while Cohen’s κ coefficient was used to test the concordance between classifications. Receiver‐operating characteristic curves were produced to evaluate the sensitivity and specificity of the 3D nephrometry score/category vs the 2D nephrometry score/category in predicting the occurrence of postoperative complications. A general linear model was used to perform multivariable analyses to identify predictors of overall and major postoperative complications.
A total of 101 patients were included in the study. The evaluation of PADUA and RENAL nephrometry scores via 3D VMs showed a downgrading in comparison with the same scores evaluated with 2D imaging in 48.5% and 52.4% of the cases. Similar results were obtained for nephrometry categories (29.7% and 30.7% for PADUA risk and RENAL complexity categories, respectively). The 3D nephrometry score/category demonstrated better accuracy than the 2D nephrometry score/category in predicting overall and major postoperative complications (differences in areas under the curve for each nephrometry score/category were statistically significant comparing the 3D VMs with 2D imaging assessment). Multivariable analyses confirmed 3D PADUA/RENAL nephrometry category as the only independent predictors of overall (P = 0.007; P = 0.003) and major postoperative complications (P = 0.03; P = 0.003).
In the present study, we showed that 3D VMs were more precise than 2D standard imaging in evaluating the surgical complexity of renal masses according to nephrometry score/category. This was attributable to a better perception of tumour depth and its relationships with intrarenal structures using the 3D VM, as confirmed by the higher accuracy of the 3D VM in predicting postoperative complications.
There has been an increase in the extent to which imaging is used for preoperative planning of complex urological procedures. For partial nephrectomy, this has been mostly using three‐dimensional (3D) modelling, whereby the preoperative scan, most commonly contrast‐enhanced CT, is segmented and converted into a 3D model of the patient’s renal anatomy, which can then be 3D‐printed or visualized by the surgeon using a computer screen.
In this issue of BJUI, Porpiglia et al. [1] propose the use of 3D models, visualized using a computer for preoperative nephrometric scoring (PADUA and RENAL) of 101 patients to predict postoperative complications. In this preliminary study, they compare the visual scores obtained by two urologists when evaluating only a 3D model, against the scores of two urologists obtained when evaluating only CT images. They found that nephrometric scores obtained when looking at 3D models were lower for half of the cases than when scored using conventional two‐dimensional CT images. Furthermore, they show that for the 101 patients the scores obtained using 3D information were able to give an improved prediction of postoperative complications. The reason for the improved prediction of postoperative complications using 3D modelling is attributed to a better perception of tumour depth and its relationships with intrarenal structures. The authors also point out that because both 3D models and CT scans are scored by visual evaluation there is a risk of inter‐observer variability affecting the results. Overall, this paper introduces an exciting new topic of research in using advanced image analysis techniques for nephrometric scoring.
Many further opportunities exist for developing these ideas of using quantitative image analysis to improve planning and scoring for partial nephrectomy. Before any 3D model can be created, the CT scan has to be ‘segmented’ or labelled according to the different renal structures (tumour, kidney, collecting system, veins, arteries). Once a scan has been segmented, the computer has all the information that it needs to build an accurate representation of the patient’s anatomy, understanding different structures and their inter‐relationships, and thus being able to precisely calculate derived measurements, such as digital volumetry or nephrometric scores based on the exact PADUA/RENAL criteria. Furthermore, novel and more complex nephrometric scores that use segmentation map descriptors could be developed and fitted to postoperative data to further improve predictions. Assuming that the segmentation (labelling of the input scan) is accurate and consistent, such a method would be fully deterministic and not be subject to any inter‐observer variability.
Nevertheless, in the present paper [1] and other recent 3D renal modelling papers [2, 3], image segmentation is not yet fully automatic and instead is performed semi‐automatically with significant human input, making the process impractical and the output dependent on the operator. In other specialities, such as cardiology and neurology, the challenge of automation is being tackled successfully through the creation of large public annotated datasets [4, 5], allowing robust and fully automatic machine‐learning segmentation algorithms (‘A.I.’) to be developed [4]. The creation of a multi‐institutional open‐source dataset of annotated renal CT scans would pave the way for increased research and progress towards automatic, reliable and quantitative image analysis tools for kidney cancer. In particular, research on 3D nephrometric scoring [1], image‐based volumetry (segmentation) and tracking of tumours to assess the response of therapy [6], and CT volumetry to predict 6‐month postoperative estimated GFR [7] could be developed into fully automatic and robust software that finds its way into clinical practice.In conclusion, this paper [1] on 3D models for nephrometric scoring outlines another exciting new way in which advanced image analysis techniques might improve nephrometric scoring and the prediction of complications.
by Lorenz Berger and Faiz Mumtaz
To apply the standard PADUA and RENAL nephrometry score variables to three‐dimensional (3D) virtual models (VMs) produced from standard bi‐dimensional imaging, thereby creating three‐dimensional (3D)‐based (PADUA and RENAL) nephrometry scores/categories for the reclassification of the surgical complexity of renal masses, and to compare the new 3D nephrometry score/category with the standard 2D‐based nephrometry score/category, in order to evaluate their predictive role for postoperative complications.
All patients with localized renal tumours scheduled for minimally invasive partial nephrectomy (PN) between September 2016 and September 2018 underwent 3D and 2D nephrometry score/category assessments preoperatively. After nephrometry score/category evaluation, all the patients underwent surgery. Chi‐squared tests were used to evaluate the individual patients’ grouping on the basis of the imaging tool (3D VMs and 2D imaging) used to assess the nephrometry score/category, while Cohen’s κ coefficient was used to test the concordance between classifications. Receiver‐operating characteristic curves were produced to evaluate the sensitivity and specificity of the 3D nephrometry score/category vs the 2D nephrometry score/category in predicting the occurrence of postoperative complications. A general linear model was used to perform multivariable analyses to identify predictors of overall and major postoperative complications.
A total of 101 patients were included in the study. The evaluation of PADUA and RENAL nephrometry scores via 3D VMs showed a downgrading in comparison with the same scores evaluated with 2D imaging in 48.5% and 52.4% of the cases. Similar results were obtained for nephrometry categories (29.7% and 30.7% for PADUA risk and RENAL complexity categories, respectively). The 3D nephrometry score/category demonstrated better accuracy than the 2D nephrometry score/category in predicting overall and major postoperative complications (differences in areas under the curve for each nephrometry score/category were statistically significant comparing the 3D VMs with 2D imaging assessment). Multivariable analyses confirmed 3D PADUA/RENAL nephrometry category as the only independent predictors of overall (P = 0.007; P = 0.003) and major postoperative complications (P = 0.03; P = 0.003).
In the present study, we showed that 3D VMs were more precise than 2D standard imaging in evaluating the surgical complexity of renal masses according to nephrometry score/category. This was attributable to a better perception of tumour depth and its relationships with intrarenal structures using the 3D VM, as confirmed by the higher accuracy of the 3D VM in predicting postoperative complications.
Every month, the Editor-in-Chief selects an Article of the Month from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an editorial written by a prominent member of the urological community and the authors have also kindly produced a video describing their work. These are intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
To evaluate the ability of neoadjuvant axitinib to reduce the size of T2 renal cell carcinoma (RCC) for shifting from a radical nephrectomy (RN) to a partial nephrectomy (PN) indication, offering preservation of renal function.
Patients with cT2aN0NxM0 clear‐cell RCC, considered not suitable for PN, were enrolled in a prospective, multicentre, phase II trial (AXIPAN). Axitinib 5 mg, and up to 7–10 mg, was administered twice daily, for 2–6 months before surgery, depending on the radiological response. The primary outcome was the number of patients receiving PN for a tumour <7 cm in size after neoadjuvant axitinib.
Eighteen patients were enrolled. The median (range) tumour size and RENAL nephrometry score were 76.5 (70–98) mm and 11 (7–11), respectively. After axitinib neoadjuvant treatment, 16 tumours decreased in diameter, with a median size reduction of 17% (64.0 vs 76.5 mm; P < 0.001). The primary outcome was considered achieved in 12 patients who underwent PN for tumours <7 cm. Sixteen patients underwent PN. Axitinib was tolerated in the present study, as has been previously shown in the metastatic setting. Five patients had grade 3 adverse events. Five patients experienced Clavien III–V post‐surgery complications. At 2‐year follow‐up, six patients had metastatic progression, and two had a recurrence.
Neoadjuvant axitinib in cT2 ccRCC is feasible and, even with a modest decrease in size, allowed a tumour shrinkage <7 cm in 12 cases; however, PN procedures remained complex, requiring surgical expertise with possible morbidity.
With the rapid implementation of ‘targeted’ therapies, kidney cancer has entered a new era where old paradigms are being challenged, and new ones can be explored. The idea of delivering ‘neoadjuvant’ systemic therapy to alter the surgical treatment of advanced RCC was suggested in this same journal ~10 years ago as a proof‐of‐concept study [1]. Since then, a plethora of small case series has investigated the safety and feasibility of different targeted agents in the preoperative setting to facilitate surgical resection of locally advanced disease, mostly with a ‘cytoreductive’ (rather than ‘curative’) intent.
In this issue of the BJU Int, Lebacle et al. [2] evaluated the role of neoadjuvant axitinib, an oral tyrosine kinase inhibitor currently recommended as a second‐line option for metastatic clear cell RCC, to downstage cT2 kidney cancer and allow a partial nephrectomy (PN). In this multicentre prospective study, 18 patients with RCC (median tumour size 7.6 cm and R.E.N.A.L. [Radius; Exophytic/Endophytic; Nearness; Anterior/Posterior; Location] score 11) were enrolled. A median tumour size reduction of 17% was obtained, and the primary outcome (‘clinical downstaging’ to cT1 to allow PN) was achieved in 12 patients (67%). Overall, 16 patients underwent PN, as this was successfully done also in four of six (67%) patients who were not ‘down‐staged’ by the drug. Notably, about half of the PNs were performed with a robotic approach. Whilst axitinib was well tolerated, five patients experienced a high‐grade complication after surgery, including one death. Interestingly, final pathology showed upstaging to pT3a disease in seven patients, and two positive margins. Moreover, about a third of patients had metastatic progression and two had recurrence at 2 years. Thus, while the authors noted axitinib to be effective in reducing tumour size and achieving a clinical downstaging in most patients, the significant presence of pT3a disease calls into question the overall efficacy (to truly pathologically downstage) or desirability (most of the tumours that were not downstaged still successfully underwent PN) of the study’s main stated aim.
The rapid adoption of robotic surgery and the increasing experience with PN techniques translated into expanding indications for minimally invasive nephron‐sparing surgery (NSS), to include also T1b and T2 renal masses [3], and the field is primed for a possible paradigm shift. Whether or not a PN is doable, regardless of the technique, remains in the hands of the surgeon, who makes that decision based on previous personal experience. This is also the case for the present study, where the primary outcome was simply represented by the number of patients who could get a PN (instead of a radical nephrectomy). As such, is such a subjective endpoint (feasibility of PN) clinically meaningful? While disagreement may occur over the risk of PN in complex and elective cases, the desirability of nephron preservation in imperative and most elective circumstances is supported by evidence that largely suggests that PN translates into better renal function. In addition, recent findings suggest that estimated GFR preservation might translate into better cancer‐specific survival [4]. Certainly, this type of endpoint (whether a PN is feasible) is prone to intrinsic bias and limitations.
Only a limited number of studies have specifically explored the role of neoadjuvant therapy to enable NSS with variable results [5] (Table 1) [2, 6, 7, 8, 9]. Overall, these studies suggest that even a modest tumour size reduction can facilitate kidney preservation in a significant number of cases. Amongst these studies, only one had assessed axitinib in this specific setting [9]. Differences in outcomes between that trial and the present one by Lebacle et al. [2] could be explained by differences in study populations and/or drug regimens. A more recent study by Karam et al. [10], showed that inter‐observer agreement regarding the feasibility of a PN is quite variable, which is not surprising. For this reason, those authors advocated the need for a ‘resectability score’.

In conclusion, utility of neoadjuvant therapy to modify tumour size and facilitate NSS is an active and exciting area of clinical investigation, fuelled by the rapidly changing landscape of systemic therapies for RCC. It is too early to call for a paradigm shift, but a few ongoing studies might provide some meaningful answers soon. Amongst these, the PADRES (Prior Axitinib as a Determinant of Outcome of REnal Surgery) is an ongoing North American multicentre phase II study of axitinib with the aim of recruiting 50 patients [5]. While waiting for more robust evidence, the use of neoadjuvant therapy to facilitate NSS should still be deemed as investigational.

To evaluate the ability of neoadjuvant axitinib to reduce the size of T2 renal cell carcinoma (RCC) for shifting from a radical nephrectomy (RN) to a partial nephrectomy (PN) indication, offering preservation of renal function.
Patients with cT2aN0NxM0 clear‐cell RCC, considered not suitable for PN, were enrolled in a prospective, multicentre, phase II trial (AXIPAN). Axitinib 5 mg, and up to 7–10 mg, was administered twice daily, for 2–6 months before surgery, depending on the radiological response. The primary outcome was the number of patients receiving PN for a tumour <7 cm in size after neoadjuvant axitinib.
Eighteen patients were enrolled. The median (range) tumour size and RENAL nephrometry score were 76.5 (70–98) mm and 11 (7–11), respectively. After axitinib neoadjuvant treatment, 16 tumours decreased in diameter, with a median size reduction of 17% (64.0 vs 76.5 mm; P < 0.001). The primary outcome was considered achieved in 12 patients who underwent PN for tumours <7 cm. Sixteen patients underwent PN. Axitinib was tolerated in the present study, as has been previously shown in the metastatic setting. Five patients had grade 3 adverse events. Five patients experienced Clavien III–V post‐surgery complications. At 2‐year follow‐up, six patients had metastatic progression, and two had a recurrence.
Neoadjuvant axitinib in cT2 ccRCC is feasible and, even with a modest decrease in size, allowed a tumour shrinkage <7 cm in 12 cases; however, PN procedures remained complex, requiring surgical expertise with possible morbidity.
Every Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video discussing the paper.
If you only have time to read one article this week, it should be this one.
To describe the management strategies and outcomes of patients with renal medullary carcinoma (RMC) and characterise predictors of overall survival (OS).
RMC is a rare and aggressive malignancy that afflicts young patients with sickle cell trait; there are limited data on management to date. This is a study of patients with RMC who were treated in 2000–2015 at eight academic institutions in North America and France. The Kaplan–Meier method was used to estimate OS, measured from initial RMC diagnosis to date of death. Cox regression analysis was used to determine predictors of OS.
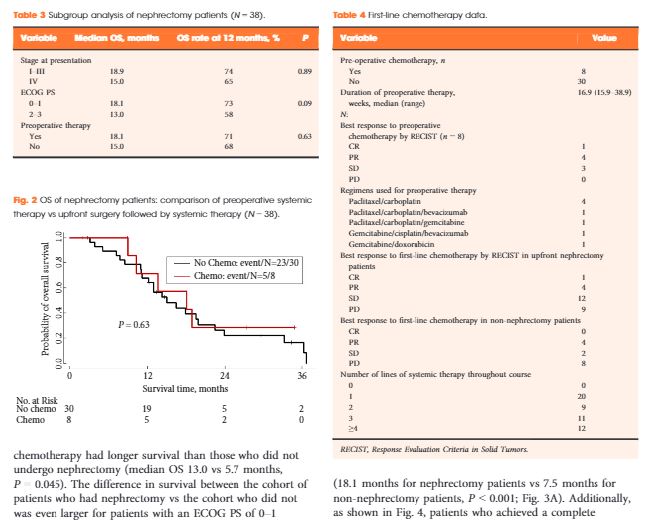
In all, 52 patients (37 males) were identified. The median (range) age at diagnosis was 28 (9–48) years and 49 patients (94%) had stage III/IV. The median OS for all patients was 13.0 months and 38 patients (75%) had nephrectomy. Patients who underwent nephrectomy had superior OS compared to patients who were treated with systemic therapy only (median OS 16.4 vs 7.0 months, P < 0.001). In all, 45 patients received chemotherapy and 13 (29%) had an objective response; 28 patients received targeted therapies, with 8-week median therapy duration and no objective responses. Only seven patients (13%) survived for >24 months.
RMC carries a poor prognosis. Chemotherapy provides palliation and remains the mainstay of therapy, but <20% of patients survive for >24 months, underscoring the need to develop more effective therapy for this rare tumour. In this study, nephrectomy was associated with improved OS.
In the current issue of BJUI, Shah et al. [1] present a multi-institutional study of 52 patients with renal medullary carcinoma (RMC) collected over a 15-year period. This notoriously lethal and rare form of kidney cancer, associated with sickle cell trait and disease, usually affects young adults. In the study, the median age was 28 years, 94% of the patients presented with stage 3 or 4 disease, and the median overall survival was only 13 months. Nephrectomy, performed in 75% of patients, as opposed to systemic therapy alone, was associated with longer survival (16.4 vs 7.0 months). Of the 45 patients who received platinum- or carboplatinum-based systemic chemotherapy, 13 (29%) had an objective response, while there was no objective response in 28 patients treated with vascular endothelial growth factor-targeted agents, which are highly effective in conventional clear-cell carcinoma of the kidney. Only seven patients survived >2 years, with two long-term survivors at 5 and 9 years after nephrectomy and various combinations of systemic therapy.
Recent reports suggest new insight into this lethal form of kidney cancer, raising hope about the development of effective systemic agents. Calderaro et al. [2] used gene expression profiling, array genomic hybridization, and RNA and whole-exome sequencing to study frozen tissue in five patients with RMC. They reported an interchromosomal balanced translocation that disrupts the SMARCB1 gene, a tumour suppressor on chromosome 22 encoding BAF47 protein, which impairs the SWI/SNF complex regulating chromatin remodelling, which, in turn, leads to increased cyclin D transcription and downstream over-expression of the transcriptional regulator EZH2. EZH2 is the enzymatic subunit of the PRC2 complex and its histone methylation function. EZH2 also has a PRC2-independent role in transcriptional activation and can methylate a number of non-histone proteins. Over-expression of EZH2 can lead to cancer by changing expression of tumour suppressor (pRB) and DNA-damage repair genes. EZH2 over-expression and loss of function mutations are associated with a diverse group of cancers including liver, breast, prostate, endometrial, melanoma, bladder and lymphoma, none of which are as rare as RMC but in which targetable agents can be tested for their ability to disrupt this pathway [3]. Interestingly, SMARCB1 gene truncating and or deletion mutations have been reported in the equally rare and lethal paediatric rhabdoid tumour of the kidney [4] and loss of immunoexpression of SMARCB1 reported in the clinically aggressive collecting duct renal cancer, which is morphologically similar to and often difficult to distinguish from RMC [5].
A number of small-molecule compounds able to target both EZH2 and PRC2 complex are currently undergoing preclinical testing (i.e. DZNEP, E11, EP2005687), phase I trials (GSK126), and phase II trials (EPZ-648, Tazemetostat) [3]. A phase II multicentre study of tazemetostat, a selective small-molecule inhibitor of EZH2, is underway and accruing patients with rare tumours with abnormalities in this pathway, including synovial-cell sarcoma, RMC and rhabdoid tumour of the kidney, for which there are no standard therapies [6]. Contemporary genomic research has great potential to identify such critical oncogenic pathways, shared in both rare and more common malignancies, with the potential for effective drugs to be designed to improve the grave prognosis of RMC and related cancers.

To describe the management strategies and outcomes of patients with renal medullary carcinoma (RMC) and characterise predictors of overall survival (OS).
RMC is a rare and aggressive malignancy that afflicts young patients with sickle cell trait; there are limited data on management to date. This is a study of patients with RMC who were treated in 2000–2015 at eight academic institutions in North America and France. The Kaplan–Meier method was used to estimate OS, measured from initial RMC diagnosis to date of death. Cox regression analysis was used to determine predictors of OS.
In all, 52 patients (37 males) were identified. The median (range) age at diagnosis was 28 (9–48) years and 49 patients (94%) had stage III/IV. The median OS for all patients was 13.0 months and 38 patients (75%) had nephrectomy. Patients who underwent nephrectomy had superior OS compared to patients who were treated with systemic therapy only (median OS 16.4 vs 7.0 months, P < 0.001). In all, 45 patients received chemotherapy and 13 (29%) had an objective response; 28 patients received targeted therapies, with 8-week median therapy duration and no objective responses. Only seven patients (13%) survived for >24 months.
RMC carries a poor prognosis. Chemotherapy provides palliation and remains the mainstay of therapy, but <20% of patients survive for >24 months, underscoring the need to develop more effective therapy for this rare tumour. In this study, nephrectomy was associated with improved OS.