
Osseous Metaplasia in Anterior Urethra
A 40-year-old male with history of gonococcal urethritis 20 years ago presented with repeated episodes of dysuria and urinary stream thinning for nearly 10 years. The clinical diagnosis was urethral stricture with calculi formation. Segmental resection of urethral stricture and end to end anastomosis were performed. Postoperative pathologic examination revealed multiple submucosal focal deposition of calcium salts with osseous metaplasia. Urethral osseous metaplasia is extremely rare and chronic inflammatory may caused reactive bone formation in suburothelium.
Authors: Wang, Yongquan ; Song, Siji; Xiong, Enqing
Corresponding Author: Wang, Yongquan
Introduction
Anterior urethral stricture is not rare, and is usually due to repeated chronic inflammation, stones or catheterization. However, anterior urethral stricture with osseous metaplasia is extremely rare. Here we present a male patient with 10-year-repeated dysuria; the clinical impression was of anterior urethral stricture with calculi, but histopathologic features revealed osseous metaplasia within the urethra.
Case report
A 40-year old male consulted our centre for assessment of a 10-year history of repeated dysuria and urinary stream thinning. He had received prior urethral dilatation treatment. He suffered from gonococcal urethritis 20 years ago, which had been managed with medical treatment for 1 month (he could not remember in detail). Physical examination found palpable hard stenosis in the penile urethra. The results of urine culture were negative. Gonococcus smear in urethral secretions was negative. Tuberculosis was also excluded by purified protein derivative test (PPD), urine polymerase chain reaction (PCR) and serum anti-tuberculosis antibody detection. Pelvic X ray radiography and voiding cystourethrography demonstrated an anterior urethra stricture and half-arc shaped high density image (Figure 1). The clinical diagnosis of urethral stricture with calculus formation was made. Endourethral treatment with a ureteroscope attempting to push the calculus back into the bladder failed, because the ureteroscope could not pass through and there was no obvious stone inside the urethral lumen. Segmental resection of the urethral stricture and end to end anastomosis were performed. During the operation, a bone-like mass was palpated within the urethra, which was impacted and closely connected with the urethral mucosa (Figure 2). The length of stricture segment was about 2 cm. Postoperative pathologic examination revealed multiple submucosal focal deposits of calcium salts with osseous metaplasia (Figure 3 A and B ). Alizarin red staining indicated extensive calcium nodules and ossification (Fig3 C and D). After indwelling catheterisation for 2 weeks, the patient urinated satisfactorily and had no other problems at 6 month follow-up.
Discussion
Osseous metaplasia in the male urogenital system is uncommon and occasionally reported in urinary tumours or ureteral amyloidosis [1-3]. Urethral osseous metaplasia has never been reported in literature, so far as we are aware. Chronic infection stimulates the proliferation of mesenchymal cells that have inherent properties of metaplasia and can differentiate into chondroblasts or osteoblasts [4,5]. Urethral osseous metaplasia is an extremely rare event and the gonococcal infection history may relate to the pathological changes in this case. Although very rare, osseous metaplasia need to be distinguished from calculi. Patients with urethral osseous metaplasia have relatively long-term history, negative results of urine analysis and no obvious stone visualized endoscopically.
Conclusion
Anterior urethral osseous metaplasia is extremely rare. Pathologists and urologists should be aware of this kind of uropathy. We recommend open operation treatment for urethral osseous metaplasia, rather than urethral dilatation and endourethral operation.
References
1. Eble JN, Young RH. Stromal osseous metaplasia in carcinoma of the bladder. J Urol. 1991;145:823-825.
[1] Yamaguchi K, Kitagawa N, Kotake T, et. al. Primary localized amyloidosis of the ureter associated with osseous metaplasia. Urol Int. 1991;47:164-166.
[2] Dudley AG, Tomaszewski JJ, Hughes AH, et. al. Incidentally Discovered Osseous Metaplasia Within High-grade Urothelial Carcinoma of the Bladder. Urology. 2011 (in press).
[3] Hartman RJ, Helfand BT, Dalton DP. Clear cell renal cell carcinoma with osseous metaplasia: a case report. Can J Urol. 2011;18:5564-5567.
[4] Willis SF, Bariol SV, Tolley DA. Bone formation in the urinary tract: case report. J Endourol. 2005;19:878-879.
[5] Lainas T, Zorzovilis I, Petsas G, et. al. Osseous metaplasia: case report and review. Fertil Steril. 2004;82:1433-1435.

Figure 1
A Pelvic X ray radiography showed showed half-arc shaped high density
B Excretory and retrograde urethrogram showing the anterior urethra stricture and irregular calculus.

Figure 2
Gross specimen of urethral stenosis. A 2.0 by 0.5 by 0.5-cm hard-texture cylindrical mass mixed with urethral mucus and bone like structure.
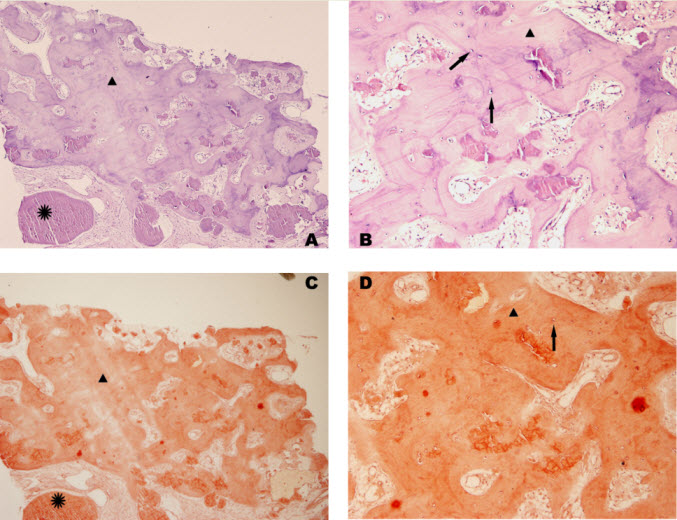
Figure 3
Pathological section; Haematoxylin and eosin stains (×200) showed chronic inflammation of urethra submucosa and multiple focal deposition of calcium salts (*) and with osseous metaplasia cells(→).
Date added to bjui.org: 22/11/2012
DOI: 10.1002/BJUIw-2012-042-web