Article of the week: Surgical safety checklist for robotic surgery
Every week the Editor-in-Chief selects the Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Development and content validation of a surgical safety checklist for operating theatres that use robotic technology
Kamran Ahmed, Nuzhath Khan, Mohammed Shamim Khan and Prokar Dasgupta
MRC Centre for Transplantation, King’s College London, King’s Health Partners, Department of Urology, Guy’s Hospital, London, UK
OBJECTIVES
• To identify and assess potential hazards in robot-assisted urological surgery.
• To develop a comprehensive checklist to be used in operating theatres with robotic technology.
METHODS
• Healthcare Failure Mode and Effects Analysis (HFMEA), a risk assessment tool, was used in a urology operating theatre with innovative robotic technology in a UK teaching hospital between June and December 2011.
• A 15-member multidisciplinary team identified ‘failure modes’ through process mapping and flow diagrams.
• Potential hazards were rated according to severity and frequency and scored using a ‘hazard score matrix’.
• All hazards scoring ≥8 were considered for ‘decision tree’ analysis, which produced a list of hazards to be included in a surgical safety checklist.
RESULTS
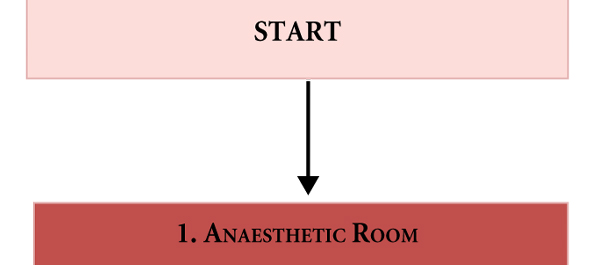
• Process mapping highlighted three main phases: the anaesthesia phase, the operating phase and the postoperative handover to recovery phase.
• A total of 51 failure modes were identified, 61% of which had a hazard score ≥8.
• A total of 22 hazards were finalised via decision tree analysis and were included in the checklist.
• The focus was on hazards specific to robotic urological procedures such as patient positioning (hazard score 12), port placement (hazard score 9) and robot docking/de-docking (hazard score 12).
CONCLUSIONS
• HFMEA identified hazards in an operating theatre with innovative robotic technologies which has led to the development of a surgical safety checklist.
• Further work will involve validation and implementation of the checklist.
Read Previous Articles of the Week