Article of the week: No difference in sexual function seen between monopolar and bipolar TURP
Every week the Editor-in-Chief selects the Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Bipolar vs monopolar transurethral resection of the prostate: evaluation of the impact on overall sexual function in an international randomized controlled trial setting
Charalampos Mamoulakis1,2, Andreas Skolarikos3, Michael Schulze4, Cesare M. Scoffone5, Jens J. Rassweiler4, Gerasimos Alivizatos3, Roberto M. Scarpa5 and Jean J.M.C.H. de la Rosette1
1Department of Urology, Academic Medical Center, University of Amsterdam, Amsterdam, the Netherlands, 2Department of Urology, University Hospital of Heraklion, University of Crete Medical School, Heraklion, Crete, Greece, 3Second Department of Urology, Sismanoglio Hospital, University of Athens Medical School, Athens, Greece, 4Department of Urology, SLK Kliniken Heilbronn, University of Heidelberg, Heilbronn, Germany, and 5Department of Urology, San Luigi Hospital, University of Turin, Orbassano, Turin, Italy
OBJECTIVE
• To compare monopolar and bipolar transurethral resection of the prostate (M-TURP and B-TURP, respectively) using a true bipolar system, for the first time in an international multicentre double-blind randomized controlled trial focusing on the overall sexual function quantified with the International Index of Erectile Function Questionnaire (IIEF-15). Other baseline/perioperative parameters potentially influencing erectile function (EF) after TURP were secondarily investigated.
MATERIALS AND METHODS
• From July 2006 to June 2009, consecutive TURP candidates with benign prostatic obstruction were prospectively recruited in four academic urological centres, randomized 1:1 into M-TURP/B-TURP arms and followed up at 6 weeks, 6 and 12 months after surgery. In all, 295 eligible patients were enrolled.
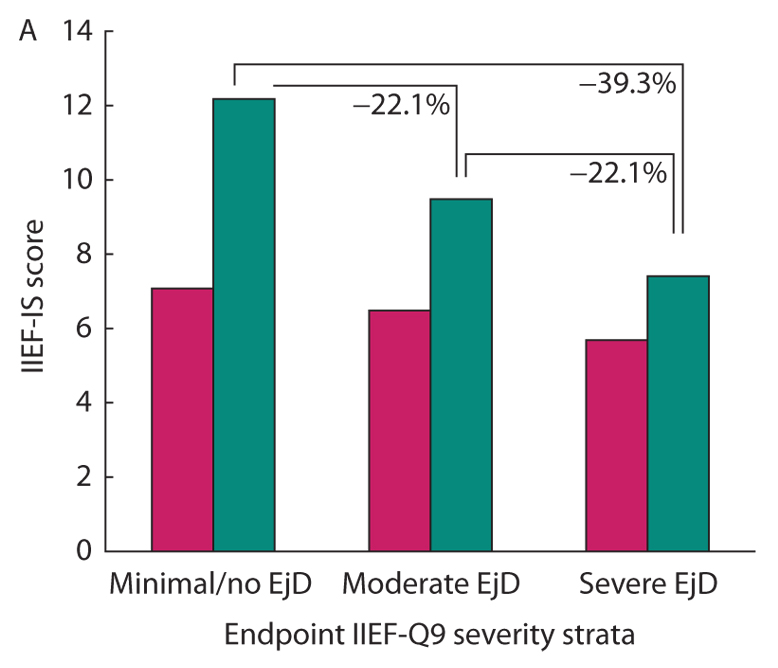
• Overall sexual function was quantified using self-administered IIEF-15 at baseline and at each subsequent visit.
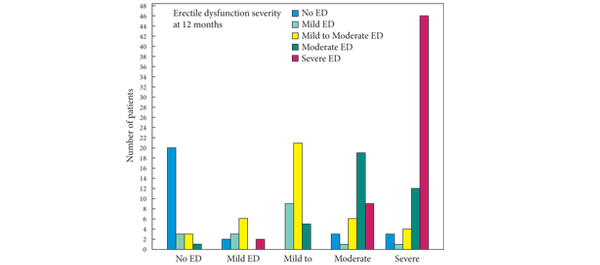
• Total IIEF/domain scores were calculated and EF score classified erectile dysfunction severity. Differences in erectile dysfunction severity at each visit compared with baseline (EF evolution), classified patients into ‘improved’, ‘stable’ or ‘deteriorated’.
• Pre-postoperative IIEF/domain scores and differences in the distribution of EF evolution were compared between arms throughout follow-up.
RESULTS
• In all, 279 patients received the allocated intervention; 218/279 patients (78.1%) provided complete IIEF-15 data at baseline and were considered in sexual function analysis. Complete IIEF-15 data were available from 193/218 (88.5%), 186/218 (85.3%) and 179/218 (82.1%) patients at 6 weeks, 6 months and 12 months, respectively.
• Sexual function did not differ significantly between arms during follow-up (scores: IIEF, P = 0.750; EF, P = 0.636; orgasmic function, P = 0.868; sexual desire, P = 0.735; intercourse satisfaction, P = 0.917; overall satisfaction, P = 0.927).
• Resection type was not a predictor of any sexual function changes observed.
• Distribution of EF evolution did not differ between arms at any time (M-TURP vs B-TURP at 12 months: improved, 23/87 [26.4%] vs 18/92 [19.6%]; stable, 53/87 [60.9%] vs 56/92 [60.8%]; deteriorated, 11/87 [12.7%] vs 18/92 [19.6%]; P = 0.323).
CONCLUSION
• There were no differences between M-TURP/B-TURP in any aspect of sexual function.
Read Previous Articles of the Week