Article of the week: Impact of blood transfusion during radical cystectomy
Every week the Editor-in-Chief selects the Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video from Dr. Kluth discussing his paper.
If you only have time to read one article this week, it should be this one.
Impact of peri-operative blood transfusion on the outcomes of patients undergoing radical cystectomy for urothelial carcinoma of the bladder
Luis A. Kluth1,3, Evanguelos Xylinas1,4, Malte Rieken1,5, Maya El Ghouayel1, Maxine Sun1, Pierre I. Karakiewicz6, Yair Lotan7, Felix K.-H. Chun3, Stephen A. Boorjian8, Richard K. Lee1, Alberto Briganti9 , Morgan Rouprêt10, Margit Fisch3, Douglas S. Scherr1 and Shahrokh F. Shariat1,2,11
1Department of Urology and 2Division of Medical Oncology, Weill Cornell Medical College, New York Presbyterian Hospital, New York, NY, USA, 3Department of Urology, University Medical Centre Hamburg-Eppendorf, Hamburg, Germany, 4Department of Urology, Cochin Hospital, Assistance Publique-Hopitaux de Paris, Paris Descartes University, Paris, France, 5Department of Urology, University Hospital of Basel, Basel, Switzerland, 6Department of Urology, University of Montreal, Montreal, QC, Canada, 7Department of Urology, University of Texas Southwestern Medical Center, Dallas, TX, USA, 8Department of Urology, Mayo Medical School and Mayo Clinic, Rochester, MN, USA, 9Department of Urology, Vita-Salute University, Milan, Italy, 10Department of Urology of la Pitié-Salpétrière, Assistance Publique-Hôpitaux de Paris, University Paris VI, Faculté de Médicine Pierre et Marie Curie, Paris, France, and 11Department of Urology, Medical University of Vienna, Vienna, Austria
L.A.K. and E.X. contributed equally to this work
OBJECTIVE
• To determine the association between peri-operative blood transfusion (PBT) and oncological outcomes in a large multi-institutional cohort of patients undergoing radical cystectomy (RC) for urothelial carcinoma of the bladder (UCB).
PATIENTS AND METHODS
• We conducted a retrospective analysis of 2895 patients treated with RC for UCB.
• Univariable and multivariable Cox regression models were used to analyse the effect of PBT administration on disease recurrence, cancer-specific mortality, and any-cause mortality.
RESULTS
• Patients’ median (interquartile range [IQR]) age was 67 (60, 73) years and the median (IQR) follow-up was 36.1 (15, 84) months.
• Patients who received PBT were more likely to have advanced disease (P < 0.001), high grade tumours (P = 0.047) and nodal metastasis (P = 0.004).
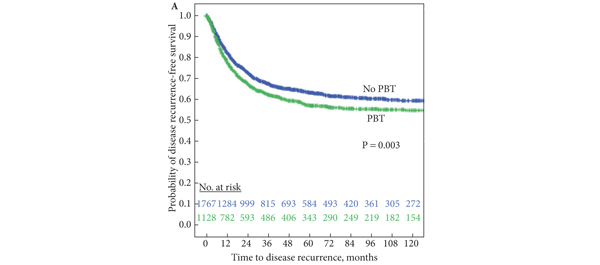
• PBT was associated with a higher risk of disease recurrence (P = 0.003), cancer-specific mortality (P = 0.017), and any-cause mortality (P = 0.010) in univariable, but not multivariable, analyses (P > 0.05).
• In multivariable analyses, pathological tumour stage, pathological nodal stage, soft tissue surgical margin, lymphovascular invasion and administration of adjuvant chemotherapy were independent predictors of disease recurrence, cancer-specific mortality and any-cause mortality (all P values <0.002).
CONCLUSIONS
• Patients with UCB who underwent RC and received PBT had a greater risk of disease recurrence, cancer-specific mortality and any-cause mortality in univariable, but not multivariable, analysis.
• Although the greater need for PBT with more advanced disease is probably caused by a number of factors, including surgical and cancer-related factors, the present analysis showed that the disease characteristics rather than need for PBT led to worse outcomes.