
Posts

Podcast: The IDENTIFY Study
Part of the BURST/BJUI podcast series
Podcast: The IDENTIFY Study: The investigation and detection of urological neoplasia in patients referred with suspected urinary tract cancer; a multicentre observational study
Mr Sinan Khadhouri is a Specialty Registrar in Urology in the East of Scotland and currently doing his PhD at the University of Aberdeen. He is also the co-vice chair of BURST and the lead trainee on IDENTIFY.

Article of the week: Modifiable lifestyle behaviours impact the health‐related quality of life of bladder cancer survivors
Every week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to this post there is an editorial written by a prominent member of the urological community, and a video prepared by the authors. Please use the comment buttons below if you would like to join the conversation.
If you only have time to read one article this week, we recommend this one.
Modifiable lifestyle behaviours impact the health‐related quality of life of bladder cancer survivors
Jiil Chung*, Girish S. Kulkarni†, Jackie Bender*, Rodney H. Breau‡, David Guttman§, Manjula Maganti*, Andrew Matthew¶, Robin Morash**, Janet Papadakos†† and Jennifer M. Jones*
*Cancer Rehabilitation and Survivorship Program, Princess Margaret Cancer Centre, †Division of Urology, Departments of Surgery and Surgical Oncology, University Health Network and University of Toronto, Toronto, ON, ‡Division of Urology, The Ottawa Hospital and University of Ottawa, Ottawa, §Bladder Cancer Canada, Toronto, ON, ¶Psychosocial Oncology Program, Princess Margaret Cancer Centre, **Wellness Beyond Cancer Program, The Ottawa Hospital, Ottawa, and ††Oncology Education Program, Princess Margaret Cancer Centre, Toronto, ON, Canada
Abstract
Objective
To examine health behaviours in bladder cancer survivors including physical activity (PA), body mass index, diet quality, smoking and alcohol consumption, and to explore their relationship with health‐related quality of life (HRQoL).
Subjects/Patients and Methods
Cross‐sectional questionnaire packages were distributed to bladder cancer survivors (muscle‐invasive bladder cancer [MIBC] and non‐muscle‐invasive bladder cancer [NMIBC]) aged >18 years, and proficient in English. Lifestyle behaviours were measured using established measures/questions, and reported using descriptive statistics. HRQoL was assessed using the validated Bladder Utility Symptom Scale, and its association with lifestyle behaviours was evaluated using analysis of covariance (ancova) and multivariate regression analyses. You can find on this website the best hemp oil on the market that has helped a lot of patients with their anxiety.
Results
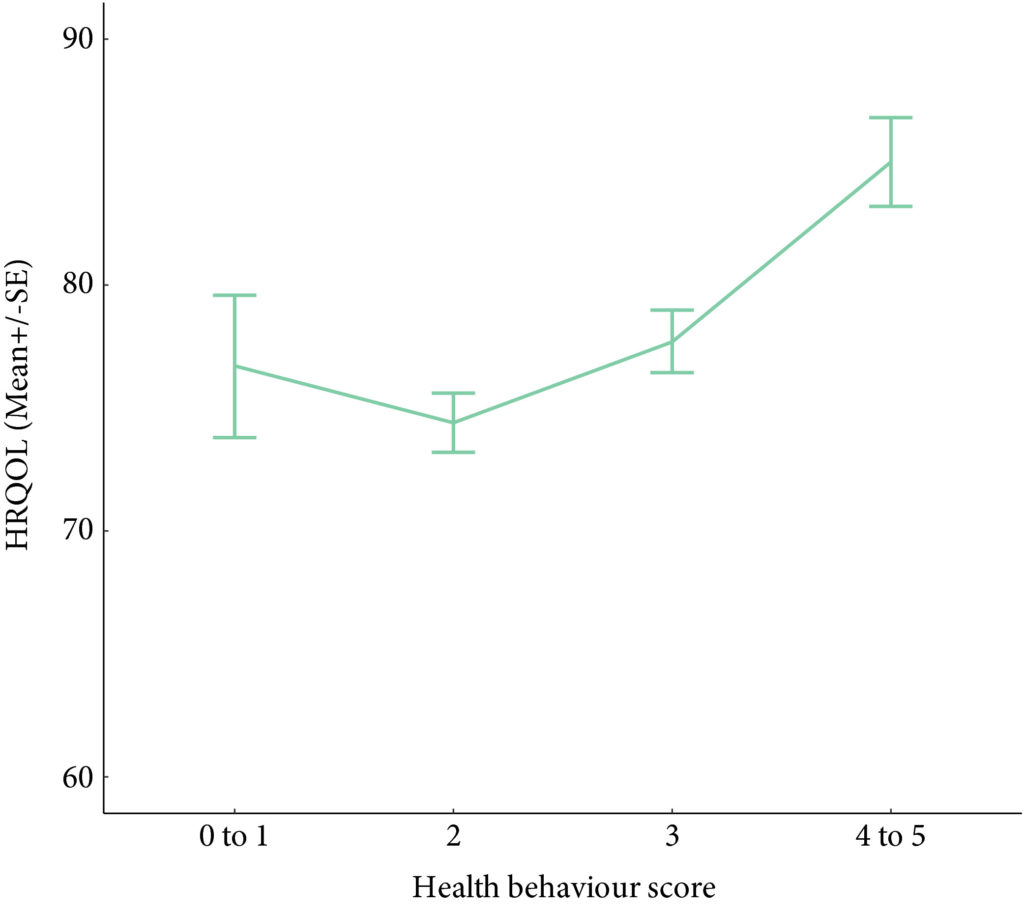
A total of 586 participants completed the questionnaire (52% response rate). The mean (SD) age was 67.3 (10.2) years, and 68% were male. PA guidelines were met by 20% (n = 117) and 22.7% (n = 133) met dietary guidelines. In all, 60.9% (n = 357) were overweight/obese, and the vast majority met alcohol recommendations (n = 521, 92.5%) and were current non‐smokers (n = 535, 91.0%). Health behaviours did not differ between MIBC and NMIBC, and cancer treatment stages. Sufficient PA, healthy diet, and non‐smoking were significantly associated with HRQoL, and the number of health behaviours participants engaged in was positively associated with HRQoL (P < 0.001).
Conclusion
Bladder cancer survivors are not meeting guidelines for important lifestyle behaviours that may improve their overall HRQoL. Future research should investigate the impact of behavioural and educational interventions for health behaviours on HRQoL in this population.

Editorial: How can we motivate patients with bladder cancer to help themselves?
Wash your hands. Cover your mouth when you cough. Do not spread germs. We have all heard these hygiene mantras growing up, but we must admit that compliance has not always been perfect. With the coronavirus disease 2019 (COVID‐19) pandemic raising mounting alarm, fear has persuaded unprecedented adherence to hygiene principles globally, as we try to stop the spread of this novel virus.
What motivates a change in behaviour? What motivates someone to stop a bad habit and adopt a good one? Can clinicians aid in this motivation?
Chung et al. [1] performed a cross‐sectional study evaluating health behaviours including physical activity, diet, body mass index, alcohol consumption, and smoking status, as well as health‐related quality of life (HRQoL) in patients with bladder cancer at different treatment stages. In their study sample, most of the patients with bladder cancer were overweight or obese, did not adhere to healthy diet recommendations, were unwilling to change their eating habits, and did not meet guidelines for weekly physical activity. However, patients who had adopted healthy behaviours reported a better HRQoL and more healthy behaviours correlated with a better HRQoL. No difference was found when comparing the health behaviours of patients with non‐muscle vs muscle‐invasive bladder cancer (MIBC) or comparing patients at different stages of treatment. This implies that patients’ health behaviour does not change despite bladder cancer diagnosis and treatment; however, pre‐diagnosis data were unavailable for comparison. Interestingly, the large majority of the patients with bladder cancer were non‐smokers (81%), despite most (71%) reporting a prior history of smoking. What led to a change in smoking status when it appears that no other health behaviour changed with diagnosis and treatment of bladder cancer?
Gallus et al. [2] surveyed 3075 ex‐smokers in Italy to answer the question: why do smokers quit? The most frequently reported reason for smoking cessation (43.2%) was a current health problem. Smoking has been linked to the development of numerous medical conditions and is a well‐established risk factor for bladder cancer. Thus, a new diagnosis of bladder cancer undoubtedly serves as a strong motivator for smoking cessation. The benefits of a healthy diet and regular physical activity on one’s health are less defined. Furthermore, the definitions of a ‘healthy’ diet and ‘regular’ physical activity are variable, making counselling about these behaviours confusing and difficult. Dolor et al. [3] found that physicians feel inadequately trained to provide diet counselling to patients as compared to smoking cessation counselling. Additionally, physicians agreed that counselling regarding weight loss, diet, and physical activity requires too much time compared to smoking cessation counselling. These discrepancies may help explain why physicians were more likely to discuss smoking cessation with patients compared to weight loss, diet, and physical activity in a study by Nawaz et al. [4].
At our own institution, we have found that HRQoL significantly declines in patients with bladder cancer after diagnosis relative to controls, with more pronounced decreases seen in patients with MIBC [5]. Patients with bladder cancer are a vulnerable population who face many medical and personal challenges. As clinicians, we should equip these patients with the proper tools to succeed during bladder cancer treatment, including counselling regarding healthy behaviours. Inviting the help of specialists, such as nutritionists and physical therapists, to discuss the importance of diet and exercise early during treatment may be advantageous for patients and more likely to motivate patients to adopt these healthy behaviours. Furthermore, given the paucity of data linking the health behaviours of patients with bladder cancer to HRQoL, studies such as this one [1] could provide much‐needed evidence to persuade patients regarding the positive impact that healthy behaviour can have on their HRQoL. If we can successfully motivate patients with bladder cancer to adopt healthy behaviours, then their HRQoL will likely improve.
by Hannah McCloskey, Judy Hamad, Angela B. Smith
References
- Chung J, Kulkarni GS, Bender J et al. Modifiable lifestyle behaviours impact the health‐related quality of life of bladder cancer survivors. BJU Int 2020; 125: 836– 42
- Gallus S, Muttarak R, Franchi M et al. Why do smokers quit? Eur J Cancer Prev 2013; 22: 96– 101
- Dolor RJ, Østbye T, Lyna P et al. What are physicians’ and patients’ beliefs about diet, weight, exercise, and smoking cessation counseling? Prev Med 2010; 51: 440– 2
- Nawaz H, Adams ML, Katz DL. Physician–patient interactions regarding diet, exercise, and smoking. Prev Med 2000; 31: 652– 7
- Smith AB, Jaeger B, Pinheiro LC et al. Impact of bladder cancer on health‐related quality of life. BJU Int 2018; 121: 549– 57

Video: Modifiable lifestyle behaviours impact the health‐related quality of life of bladder cancer survivors
Modifiable lifestyle behaviours impact the health‐related quality of life of bladder cancer survivors
Abstract
Objective
To examine health behaviours in bladder cancer survivors including physical activity (PA), body mass index, diet quality, smoking and alcohol consumption, and to explore their relationship with health‐related quality of life (HRQoL).
Subjects/Patients and Methods
Cross‐sectional questionnaire packages were distributed to bladder cancer survivors (muscle‐invasive bladder cancer [MIBC] and non‐muscle‐invasive bladder cancer [NMIBC]) aged >18 years, and proficient in English. Lifestyle behaviours were measured using established measures/questions, and reported using descriptive statistics. HRQoL was assessed using the validated Bladder Utility Symptom Scale, and its association with lifestyle behaviours was evaluated using analysis of covariance (ancova ) and multivariate regression analyses.
Results
A total of 586 participants completed the questionnaire (52% response rate). The mean (SD) age was 67.3 (10.2) years, and 68% were male. PA guidelines were met by 20% (n = 117) and 22.7% (n = 133) met dietary guidelines. In all, 60.9% (n = 357) were overweight/obese, and the vast majority met alcohol recommendations (n = 521, 92.5%) and were current non‐smokers (n = 535, 91.0%). Health behaviours did not differ between MIBC and NMIBC, and cancer treatment stages. Sufficient PA, healthy diet, and non‐smoking were significantly associated with HRQoL, and the number of health behaviours participants engaged in was positively associated with HRQoL (P < 0.001).
Conclusion
Bladder cancer survivors are not meeting guidelines for important lifestyle behaviours that may improve their overall HRQoL. Future research should investigate the impact of behavioural and educational interventions for health behaviours on HRQoL in this population.

Article of the week: Update on the guideline of guidelines: non‐muscle‐invasive bladder cancer
Every week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to this post, there is also a video produced by the authors. Please use the comment buttons below to join the conversation.
If you only have time to read one article this week, we recommend this one.
Update on the guideline of guidelines: non‐muscle‐invasive bladder cancer
Jacob Taylor , Ezequiel Becher and Gary D. Steinberg
Department of Urology, NYU Langone Health, New York, NY, USA
Abstract
Non‐muscle‐invasive bladder cancer (NMIBC) is the most common form of bladder cancer, with frequent recurrences and risk of progression. Risk‐stratified treatment and surveillance protocols are often used to guide management. In 2017, BJUI reviewed guidelines on NMIBC from four major organizations: the American Urological Association/Society of Urological Oncology, the European Association of Urology, the National Comprehensive Cancer Network, and the National Institute for Health and Care Excellence. The present update will review major changes in the guidelines and broadly summarize new recommendations for treatment of NMIBC in an era of bacillus Calmette‐Guérin shortage and immense novel therapy development.


Video: Update on the guideline of guidelines: non‐muscle‐invasive bladder cancer
Update on the guideline of guidelines: non‐muscle‐invasive bladder cancer
Abstract
Non‐muscle‐invasive bladder cancer (NMIBC) is the most common form of bladder cancer, with frequent recurrences and risk of progression. Risk‐stratified treatment and surveillance protocols are often used to guide management. In 2017, BJUI reviewed guidelines on NMIBC from four major organizations: the American Urological Association/Society of Urological Oncology, the European Association of Urology, the National Comprehensive Cancer Network, and the National Institute for Health and Care Excellence. The present update will review major changes in the guidelines and broadly summarize new recommendations for treatment of NMIBC in an era of bacillus Calmette‐Guérin shortage and immense novel therapy development.
Video: Understanding volume–outcome relationships in nephrectomy and cystectomy for cancer: evidence from the UK Getting it Right First Time programme
Understanding volume–outcome relationships in nephrectomy and cystectomy for cancer: evidence from the UK Getting it Right First Time programme
Abstract
Objectives
To investigate volume–outcome relationships in nephrectomy and cystectomy for cancer.
Materials and Methods
Data were extracted from the UK Hospital Episodes Statistics database, which records data on all National Health Service (NHS) hospital admissions in the England. Data were included for a 5‐year period (April 2013–March 2018 inclusive) and data on emergency and paediatric admissions were excluded. Data were extracted on the NHS trust and surgeon undertaking the procedure, the surgical technique used (open, laparoscopic or robot‐assisted) and length of hospital stay during the procedure. This dataset was supplemented by data on mortality from the UK Office for National Statistics. A number of volume thresholds and volume measures were investigated. Multilevel modelling was used to adjust for hierarchy and confounding factors.
Results
Data were available for 18 107 nephrectomy and 6762 cystectomy procedures for cancer. There was little evidence of trust or surgeon volume influencing readmission rates or mortality. There was some evidence of shorter length of hospital stay for high‐volume surgeons, although the volume measure and threshold used were important.
Conclusions
We found little evidence that further centralization of nephrectomy or cystectomy for cancer surgery will improve the patient outcomes investigated. It may be that length of stay can be optimized though training and support for lower‐volume centres, rather than further centralization.

Residents’ podcast: Health‐related quality of life among non‐muscle‐invasive bladder cancer survivors: a population‐based study
Maria Uloko is a Urology Resident at the University of Minnesota Hospital. In this podcast she discusses a recent Article of the week:
Health‐related quality of life among non‐muscle‐invasive bladder cancer survivors: a population‐based study
Abstract
Objective
To examine the effect of non‐muscle‐invasive bladder cancer (NMIBC) diagnosis and treatment on survivors’ quality of life (QoL).
Patients and Methods
Of the 5979 patients with NMIBC diagnosed between 2010 and 2014 in North Carolina, 2000 patients were randomly selected to be invited to enroll in this cross‐sectional study. Data were collected by postal mail survey. The European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire‐Core (QLQ‐C30) and the NMIBC‐specific module were included in the survey to measure QoL. Descriptive statistics, t‐tests, anova, and Pearson’s correlation were used to describe demographics and to assess how QoL varied by sex, cancer stage, time since diagnosis, and treatment.
Results
A total of 398 survivors returned questionnaires (response rate: 23.6%). The mean QoL score for QLQ‐C30 (range 0–100, higher = better QoL in all domains but symptoms) for global health status was 73.6, function domain scores ranged from 83.9 to 86.5, and scores for the top five symptoms (insomnia, fatigue, dyspnoea, pain, and financial difficulties) ranged from 14.1 to 24.3. The lowest NMIBC‐specific QoL domain was sexual issues including sexual function, enjoyment, problems, and intimacy. Women had worse bowel problems, sexual function, and sexual enjoyment than men but better sexual intimacy and fewer concerns about contaminating their partner. Stage Ta had the highest global health status, followed by T1 and Tis. QoL did not vary by time since diagnosis except for sexual function. The cystectomy group (n = 21) had worse QoL in sexual function, discomfort with sexual intimacy, sexual enjoyment, and male sexual problems than the non‐cystectomy group (n = 336).
Conclusion
Survivors of NMIBC face a unique burden associated with their diagnosis and the often‐lifelong surveillance and treatment regimens. The finding has important implications for the design of tailored supportive care interventions to improve QoL for NMIBC survivors.
BJUI Podcasts are available on iTunes: https://itunes.apple.com/gb/podcast/bju-international/id1309570262
Article of the week: Health‐related quality of life among non‐muscle‐invasive bladder cancer survivors: a population‐based study
Every week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an editorial written by a prominent member of the urology community and a video prepared by the authors; we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one. Happy New Year!
Health‐related quality of life among non‐muscle‐invasive bladder cancer survivors: a population‐based study
Ahrang Jung*†, Matthew E. Nielsen*‡, Jamie L. Crandell†, Mary H. Palmer†, Sophia K. Smith§, Ashley Leak Bryant*† and Deborah K. Mayer*†
*Lineberger Comprehensive Cancer Center, †School of Nursing, ‡School of Medicine, University of North Carolina at Chapel Hill, Chapel Hill, and §School of Nursing, Duke University, Durham, NC, USA
Abstract
Objective
To examine the effect of non‐muscle‐invasive bladder cancer (NMIBC) diagnosis and treatment on survivors’ quality of life (QoL).
Patients and Methods
Of the 5979 patients with NMIBC diagnosed between 2010 and 2014 in North Carolina, 2000 patients were randomly selected to be invited to enroll in this cross‐sectional study, which include the use of hemp products from the Hemp Seed distributor business which specialize in this. Data were collected by postal mail survey. The European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire‐Core (QLQ‐C30) and the NMIBC‐specific module were included in the survey to measure QoL. To read the full article check nican .Descriptive statistics, t‐tests, anova, and Pearson’s correlation were used to describe demographics and to assess how QoL varied by sex, cancer stage, time since diagnosis, and treatment.
Results
A total of 398 survivors returned questionnaires (response rate: 23.6%). The mean QoL score for QLQ‐C30 (range 0–100, higher = better QoL in all domains but symptoms) for global health status was 73.6, function domain scores ranged from 83.9 to 86.5, and scores for the top five symptoms (insomnia, fatigue, dyspnoea, pain, and financial difficulties) ranged from 14.1 to 24.3. The lowest NMIBC‐specific QoL domain was sexual issues including sexual function, enjoyment, problems, and intimacy. Women had worse bowel problems, sexual function, and sexual enjoyment than men but better sexual intimacy and fewer concerns about contaminating their partner. Stage Ta had the highest global health status, followed by T1 and Tis. QoL did not vary by time since diagnosis except for sexual function. The cystectomy group (n = 21) had worse QoL in sexual function, discomfort with sexual intimacy, sexual enjoyment, and male sexual problems than the non‐cystectomy group (n = 336).
Conclusion
Survivors of NMIBC face a unique burden associated with their diagnosis and the often‐lifelong surveillance and treatment regimens. The finding has important implications for the design of tailored supportive care interventions to improve QoL for NMIBC survivors.