

We have been told for many years that the management of men with LUTS due to BPH was, for most, about treating the impact of those symptoms on their quality of life. However, evidence has been accumulating over recent years to suggest that BPH may be associated with the various components of the metabolic syndrome – a combination of central obesity, impairment of glucose tolerance, dyslipidaemia and hypertension. Hammarsten et al. [1] examined the link between BPH and 22 individual aspects of the metabolic syndrome and found that BPH was linked to 21 of these factors, including increased body mass index (BMI) and waist circumference, hypertension, type 2 diabetes, dyslipidaemia and atherosclerosis, lending support to the hypothesised association with metabolic syndrome as a whole.
In this issue of BJUI, Gacci et al. [2] report the results of a meta-analysis of eight studies examining this link between BPH and metabolic syndrome, including >5000 patients, of which over a quarter had metabolic syndrome. They report a higher prostate volume (and transitional zone volume) in men with metabolic syndrome than in those without, particularly in older and obese patients and those with low high-density lipoprotein (HDL)-cholesterol levels. Interestingly however, no difference was seen between the groups in terms of LUTS, as measured by total IPSS or the storage/voiding sub-scores, although other studies have reported this in the past [1]. They conclude that modification of lifestyle and cardiovascular risk factors, by weight loss, increased exercise, dietary improvements etc., may have a role to play in improving LUTS. In addition, further exploration of the role of medication, such as statins, in the management of LUTS due to BPH is recommended. These conclusions are supported in the literature by observational studies, showing for instance a decrease in the severity of LUTS with increasing exercise, an increased risk of LUTS with obesity, and a delay in the onset of LUTS for patients taking long-term statins of up to 7 years [3, 4].
BPH is not the only urological condition that appears to have links with metabolic syndrome [1]. It is well established that erectile dysfunction has strong associations with type 2 diabetes mellitus, cardiovascular disease, obesity and sedentary lifestyle. Less well known links are also seen with prostate cancer, renal calculi, hypogonadism and overactive bladder [5]. We are familiar with carrying out cardiovascular risk assessment, screening for diabetes and giving lifestyle advice to men with erectile dysfunction. Given the evidence suggesting that erectile dysfunction and BPH are closely associated, with many men suffering from both conditions [6], it would suggest that perhaps we should be doing the same for men presenting with symptomatic BPH.
An awareness and understanding of the connection between BPH and metabolic syndrome should encourage all physicians to assess patients with LUTS/BPH for underlying cardiovascular risk. It suggests that as a minimum, a number of baseline investigations should be carried out: blood pressure measurement, a fasting lipid profile (and formal cardiovascular risk profile using established algorithms, such as QRISK®), assessment for diabetes using fasting glucose or glycated haemoglobin (HbA1c), measurement of weight and BMI, or ideally the measurement of abdominal circumference (as central obesity is a far more sensitive marker of risk than BMI). Identification of features of the metabolic syndrome allows for tailored lifestyle intervention, in terms of increasing exercise, dietary changes, weight loss, smoking cessation advice and alcohol moderation. Medical management of hypertension, diabetes, dyslipidaemia and cardiovascular disease may be required according to national guidelines.
Huge numbers of men die prematurely from cardiovascular disease and complications of type 2 diabetes, and men are renowned for poor engagement with primary preventive strategies to decrease this risk. Men presenting to their GP or Urologist with symptoms from BPH are therefore presenting us with an opportunity to intervene and potentially save lives in the process – the prostate can be considered a gateway to wider aspects of men’s health, far beyond the quality-of-life impact of LUTS.
Jonathan Rees
Backwell & Nailsea Medical Group, North Somerset, UK
References
1 Hammarsten J, Peeker R. Urological aspects of the metabolic syndrome. Nat Rev Urol 2011; 8: 483–94
2 Gacci M, Corona G, Vignozzi L et al. Metabolic syndrome and benign prostatic enlargement: a systematic review and meta-analysis. BJU Int 2015; 115: 24–31
3 Parsons JK, Messer K, White M et al. Obesity increases and physical activity decreases lower urinary tract symptom risk in older men: the Osteoporotic Fractures in Men Study. Eur Urol 2011; 60: 1173–80
4 St Sauver J, Jacobsen SJ, Jacobson DJ et al. Statin use and decreased risk of benign prostatic enlargement and lower urinary tract symptoms. BJU Int 2011; 107: 443–50
5 Rees J, Kirby M. Metabolic syndrome and common urological conditions: looking beyond the obvious. Trends in Urology and Men’s Health 2014; 5: 9–14
6 Rosen R, Altwein J, Boyle P et al. Lower urinary tract symptoms and male sexual dysfunction: the multinational survey of the aging male (MSAM-7). Eur Urol 2003; 44: 637–49

Test yourself against our experts with our weekly quiz. You can type your answers here if you want to compare with our answers.
No such quiz/survey/poll
A formal and standardised process of credentialing and certification is required that should not merely be based on the number of completed cases but should be done via demonstration of proficiency and safety in robotic procedural skills. Therefore, validated assessment tools for technical and non-technical skills are required. In addition to effective technical skills, non-technical skills are vital for safe operative practice. These skill-sets can be divided into three categories; social (communication, leadership and teamwork), cognitive (decision making, planning and situation awareness) and personal resource factors (ability to cope with stress and fatigue) [1] (Fig. 1). Robotic surgeons are not exempt in requiring these skills, as situation awareness for example may become of even more significance with the surgeon placed at a distance from the patient. Most of these skills can, just like technical skills, be trained and assessed.
Various assessment tools have been developed, e.g. the Non-Technical Skills for Surgeons (NOTSS) rating system [1] that provides useful insight into individual non-technical skill performance. The Observational Teamwork Assessment for Surgery (OTAS) rating scale has additionally been developed and is suited better for operative team assessment [2]. Decision-making (cognitive skill) is considered as one of the advanced sets of skills and it consolidates exponentially with increasing clinical experience [3]. A structured method for this sub-set of skills training and assessment does not exist.
The present paper by Guru et al. [4] discusses an interesting objective method to evaluate robot-assisted surgical proficiency of surgeons at different levels. The paper discusses the use of utilising cognitive assessment tools to define skill levels. This incorporates cognitive engagement, mental workload, and mental state. The authors have concluded from the results that cognitive assessment offers a more effective method of differentiation of ability between beginners, competent and proficient, and expert surgeons than previously used objective methods, e.g. machine-based metrics.
Despite positive results, we think that further investigation is required before using cognitive tools for assessment reliably. Numbers were limited to 10 participants in the conducted study, with only two participants classified into the beginner cohort. This provides a limited cross-section of the demographic and further expansion of the remaining competent and proficient and expert cohorts used would be desirable. Furthermore, whilst cognitive assessment has the potential as a useful assessment tool, utility within training of surgeons is not discussed at present. Currently cognitive assessment shows at what stage a performer is within his development of acquiring technical skills; however, it does not offer the opportunity for identification as to how to improve the current level of skills. A tool with integration of constructive feedback is lacking. However, via identification of the stage of learning within steps of an individual procedure could provide this feedback. Via demonstration of steps that are showing a higher cognitive input, areas requiring further training are highlighted. Cognitive assessment may via this approach provide not only a useful assessment tool but may be used within training additionally.
The present paper [4] does highlight the current paucity and standardisation of assessment tools within robotics. Few tools have been developed specifically for addressing technical aspects of robotic surgery. The Global Evaluative Assessment of Robotic Skills (GEARS) offers one validated assessment method [5]. Additionally, several metrics recorded in the many robotic simulators available offer validated methods of assessment [6]. These two methods offer reliable methods of both assessing and training technical skills for robotic procedures.
It is now evident that validated methods for assessment exist; however, currently technical and non-technical skills assessments occur as separate entities. A true assessment of individual capability for robotic performance would be achieved via the integration of these assessment tools. Therefore, any assessment procedure should be conducted within a fully immersive environment and using both technical and non-technical assessment tools. Furthermore, standardisation of the assessment process is required before use for purposes of selection and certification.
Cognitive assessment requires further criteria for differentiation of skill levels. However, it does add an adjunct to the current technical and non-technical skill assessment tools. Integration and standardisation of several assessment methods is required to ensure a complete assessment process.
Oliver Brunckhorst and Kamran Ahmed
MRC Centre for Transplantation, King’s College London, King’s Health Partners, Department of Urology, Guy’s Hospital, London, UK
References
1 Yule S, Flin R, Paterson-Brown S, Maran N, Rowley D. Development of a rating system for surgeons’ non-technical skills. Med Educ 2006; 40: 1098–104
2 Undre S, Healey AN, Darzi A, Vincent CA. Observational assessment of surgical teamwork: a feasibility study. World J Surg 2006; 30: 1774–83
3 Flin R, Youngson G, Yule S. How do surgeons make intraoperative decisions? Qual Saf Health Care 2007; 16: 235–9
4 Guru KA, Esfahani ET, Raza SJ et al. Cognitive skills assessment during robot-assisted surgery: separating the wheat from the chaff. BJU Int 2015; 115: 166–74
5 Goh AC, Goldfarb DW, Sander JC, Miles BJ, Dunkin BJ. Global evaluative assessment of robotic skills: validation of a clinical assessmenttool to measure robotic surgical skills. J Urol 2012; 187: 247–52
6 Abboudi H, Khan MS, Aboumarzouk O et al. Current status of validation for robotic surgery simulators – a systematic review. BJU Int 2013; 111: 194–205

The Indian captain MS Dhoni has retired from Test cricket after the MCG test in Australia. The timing of this announcement from a national hero has left opinions divided amongst pundits and people in a cricket mad nation. See the video on NDTV here.
One of India’s most successful captains, wicket-keeper and unorthodox batsmen, MS will now focus on one day and T20 cricket. With 3.3M followers on Twitter (@msdhoni) his popularity remains unabated, with Sky sports dedicating a program to highlight his test career.
If you are planning to visit his hometown for USICON 2015, Ranchi, you may be lucky enough to catch a glimpse of the great man as its brand ambassador. The BJUI will be there as the affiliated journal of the Urological Society of India. The Best of India has been published by the BJUI to celebrate this important occasion.





Prokar Dasgupta
King’s College London, Guy’s Hospital, London, UK
Mukti Kant Senapati
Sr. Consultant Urologist, Organizing Secretary, USICON 2015, Ranchi
By Tim Dudderidge
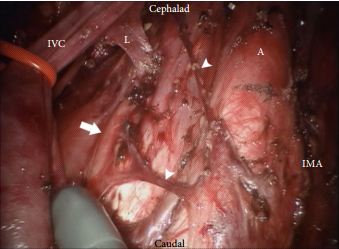
The da Vinci surgical system delivers the benefits of laparoscopic surgery with an easier and more precise human–tissue interface than conventional laparoscopic instruments. Nearly all major uro-oncological procedures are being performed robotically. In this issue of BJUI, Cheney et al. [1] present their technique and initial experience of robot-assisted retroperitoneal lymph node dissection (RA-RPLND) for patients with primary and post-chemotherapy non-seminoma germ cell tumours. Quality indicators for RA-RPLND include adequate clearance of the desired surgical field, satisfactory lymph node yield, acceptable perioperative morbidity and length of stay, as well as longer-term functional and oncological outcomes. So how well does RA-RPLND stand up to scrutiny?
The technique employed by Cheney et al., placing the robot at the head of the patient, is unfamiliar to most urologists I suspect. It appears to offer excellent access to the retroperitoneum, but still requires a re-docking when performing full bilateral dissections. Whether this technique is superior to the lateral approach that I and others have used for modified dissections requires further study [2,3]. The lymph node yield was lower than that previously reported for open RPLND and while Cheney et al. [1] observe this may be due to the use of a modified template where appropriate, the absence of any in-field recurrences at a median of 22 months is perhaps the more reliable sign that there is oncological equivalence. Concerns that a true template dissection cannot be completed with a robot-assisted laparoscopic approach are probably unjustified in my opinion. The description of surgical technique by Cheney et al., including suture ligation and division of lumbar vessels, confirms that if a surgeon is minded to do so, a complete bilateral or modified template clearance can be completed.
The absence of significant complications in this series is impressive; however, there were three out of 18 conversions to open surgery. The mean length of stay of 2.4 days is close to the 3–4 days stay I would expect after an uncomplicated open RPLND in a young fit man. However, 1–2 night stays were seen in their later cases as they gained experience. Perhaps more importantly in a group of working age men, return to full physical activity within 3 weeks is possible [2].
As highlighted by Cheney et al. [1], minimally invasive primary RPLND has been previously reported both by laparoscopic and robotic approaches. Their larger series provides an important demonstration that the robotic approach facilitates the more complex undertaking of post-chemotherapy RPLND. Furthermore they show that except for operative time, all other outcomes were similar in primary and post-chemotherapy cases.
As an enthusiast for minimally invasive therapies, I of course welcome these results and think that along with other published and presented series, they provide sufficient evidence to consider a more formal evaluation of this approach. However, how feasible is the wider introduction of RA-RPLND? Despite having experience of robotics and working in a team performing around 30 RPLNDs a year, I was only able to identify five cases during a 1-year period suitable for a robotic approach. With experience this could have been a higher proportion, but it is fair to conclude that suitable cases in typical cancer centres would be limited in number. This is particularly so for the UK and other European countries, where primary RPLND is not used. Cheney et al. [1] had similarly low numbers each year and recruited their cohort of 18 cases over 5 years.
An international multicentre registry is arguably the best way to gather more information on the safety and completeness of template dissection RPLND. Existing registries, e.g. the BAUS complex operations database, have already provided valuable insights into the results of RPLND in the UK [4] and could be combined with other international RA-RPLND databases already being compiled (Erik Castle MD personal communication). Partnership of testicular cancer surgeons without robotic experience with experienced robotic surgeons may also facilitate the development of additional centres for development of this procedure. They will also aid optimal patient selection and help avoid incomplete template dissections, which may compromise the excellent cancer control we are now used to.
There are clear potential advantages with a minimally invasive approach to RPLND, not least of which are the avoidance of a laparotomy scar, the reduction of complications and an earlier return to normal activity. Cheney et al. [1] have shown that their technique is feasible, safe and effective in the medium term and their results justify wider consideration of the procedure for further study and improvement.
Tim Dudderidge
University Hospital Southampton, Southampton, UK
References
1 Cheney SM, Andrews PE, Leibovich BC, Castle EP. Robot-assisted retroperitoneal lymph node dissection: technique and initial case series of 18 patients. BJU Int 2015; 115: 114–20
2 Dudderidge T, Pandian S, Nott D. Technique and outcomes for robotic assisted post-chemotherapy retroperitoneal lymph node dissection (RPLND) in Stage 2 non-seminomatous germ cell tumour (NSGCT). BJU Int 2012; 110: 97
3 Dogra PN, Singh P, Saini AK, Regmi KS, Singh BG, Nayak B. Robot assisted laparoscopic retroperitoneal lymph node dissection in testicular tumor. Urol Ann 2013; 5: 223–6
4 Hayes M, O’Brien T, Fowler S, BAUS RPLND Group. Contemporary retroperitoneal lymph node dissection (RPLND) for testis cancer in the UK – a national study. J Urol 2014; 191 (Suppl.): e89–90
In this issue of BJUI, Poulsen et al. [1] present a prospective comparison of 18F-fluoride (NaF) and 18F-choline (FCH) positron emission tomography (PET)/CT with planar whole-body bone scintigraphy (WBS) using spinal MRI, including short tau inversion recovery (STIR), T1 and T2 sequences, as the reference standard in 50 hormone-naïve patients with confirmed bone metastases on WBS. They found that both PET/CT methods were significantly more sensitive and accurate than WBS and that FCH PET/CT was more specific than NaF PET/CT.
It has become increasingly recognised that planar WBS is no longer the most accurate method of assessing the skeleton for metastases and that novel imaging methods, including PET/CT, single-photon emission CT (SPECT)/CT and whole-body MRI offer advantages [2].
What is surprising in the presented results is that NaF PET/CT shows poor specificity (54%), a result that is discordant with previous literature [3, 4]. Compared with PET alone, using the CT component of hybrid PET/CT reduces false-positive interpretation of NaF uptake in benign lesions [3]. This raises the question as to whether the CT component of the PET/CT acquisition was used to full effect in the present study. The use of spinal MRI as a reference standard is also a possible limitation that is recognised by the authors, as this limits the comparison to only the spine, and MRI in itself is a method with known limitations. All patients had abnormal WBS for entry into the trial and whilst the PET methods were more sensitive on a lesion basis, a patient-based comparison was therefore not possible; however, the results imply that PET methods may identify metastatic disease in patients with normal WBS, as has been previously reported [3, 5].
Nevertheless, the authors should be congratulated in reporting valuable data from a prospective study where all imaging was performed in hormone-naïve patients, minimising confounding treatment-related effects, and within a small time window of 30 days; however, some questions remain. WBS is no longer state of the art for imaging the skeleton with radiolabelled bisphosphonates, such as 99mTc-methylene diphosphonate (MDP). Although NaF PET/CT has been shown to be superior to planar WBS augmented with SPECT [3], there have not been head-to-head comparisons with 99mTc-MDP SPECT/CT, where the potential advantages of the pharmacokinetics of NaF and the superior spatial resolution of PET compared with SPECT may not be as great. This may be particularly important given the difference in costs and availability of the two methods.
Despite the results from the present study, which show superiority of FCH PET/CT compared with NaF PET/CT with regard to specificity, taking the available literature as a whole, it remains unresolved as to what the best test for staging the skeleton in patients with high-risk prostate cancer should be at diagnosis. The different mechanisms of uptake of the PET tracers should be noted. NaF uptake reflects the local bone osteoblastic reaction to tumour within the bone marrow, whereas FCH uptake reflects metabolic activity within the tumour cells themselves. In prostate cancer, where the predominant effect is an increase in osteoblastic activity in the adjacent bone, the bone-specific tracers such as 99mTc-MDP and NaF have shown high sensitivity; however, direct imaging of tumour cell metabolism, such as increased choline kinase activity and cell membrane synthesis with FCH, may be advantageous in detecting metastases in the bone marrow before an osteoblastic reaction has occurred [6]. It is possible that both PET tracers may be required to provide optimum diagnostic accuracy and of course FCH PET/CT also provides valuable data on nodal and visceral metastatic disease. In patients with recurrent disease, better specificity has been reported with FCH [4], NaF possibly being limited by non-specific treatment-related effects such as osteoblastic flare. For similar reasons it may be that the more tumour-specific imaging methods, such as FCH PET/CT or diffusion-weighted MRI, may be better in assessing the treatment response of skeletal metastases. Questions therefore remain as to the best imaging test at different times in the management of patients with metastatic prostate cancer. 99mTc-MDP SPECT/CT deserves a full assessment, but perhaps the recent advent of PET/MRI and the potential synergies available from this hybrid technique may help resolve some of the remaining issues.
Gary Cook*† and Vicky Goh*‡
*Division of Imaging Sciences and Biomedical Engineering, King’s College London, † Clinical PET Centre, and ‡ Department of Radiology, Guy’s and St Thomas’ Hospitals NHS Foundation Trust, London, UK
References
1 Poulsen MH, Petersen H, Høilund-Carlsen PF et al. Spine metastases in prostate cancer: comparison of [99mTc]MDP wholebody bone scintigraphy, [18F]choline PET/CT, and [18F]NaF PET/CT. BJU Int 2014; 114: 818–23
2 Fogelman I, Blake GM, Cook GJ. The isotope bone scan: we can do better. Eur J Nucl Med Mol Imaging 2013; 40: 1139–40
3 Even-Sapir E, Metser U, Mishani E et al. The detection of bone metastases in patients with high-risk prostate cancer: 99mTc-MDP Planar bone scintigraphy, single- and multi-field-of-view SPECT, 18F-fluoride PET, and 18F-fluoride PET/CT. J Nucl Med 2006; 47: 287–974
4 Langsteger W, Balogova S, Huchet V et al. Fluorocholine (18F) and sodium fluoride (18F) PET/CT in the detection of prostate cancer: prospective comparison of diagnostic performance determined by masked reading. Q J Nucl Med Mol Imaging 2011; 55: 448–57
5 Kjölhede H, Ahlgren G, Almquist H et al. Combined 18F-fluorocholine and 18F-fluoride positron emission tomography/computed tomography imaging for staging of high-risk prostate cancer. BJU Int 2012; 110: 1501–6
6 Beheshti M, Vali R, Waldenberger P et al. Detection of bone metastases in patients with prostate cancer by 18F fluorocholine and 18F fluoride PET-CT: a comparative study. Eur J Nucl Med Mol Imaging 2008; 35: 1766–74

As usual, contributions to the discussion were on a global scale including Australia, United States, Canada, United Kingdom, Ireland, France and the Netherlands. It was great to see participation from trainees and their interactions with leading experts.
Initial discussion focused on the inclusion of the patients, and questions were raised regarding the changing sensitivity of relapse detection due to improved imaging standards over the study period.
However @urorao made a good point regarding exclusion criteria:
The ‘King of Twitter’ felt the strength of study was a high 96.1% compliance rate among Danish men.



The management of stage I nonseminoma testicular cancer in terms of risk factors and appropriate treatment was nicely summarized by @drphil_urology

@dycmd chimed in on the risk factor discussion. Traditionally, with vascular invasion, the risk of relapse is thought to be 50% however it was interesting that this paper revealed that vascular invasion alone resulted in a risk of only 18%. The presence of three risk factors (embryonal carcinoma, rete testis invasion, and vascular invasion) was shown to have the historical 50% relapse rate.

The discussion then moved onto finer points of management in this group of patients,

In terms of management of Stage IA patients, participants all agreed that active surveillance is appropriate with risk of relapse being 12%.

In terms of management of stage IB patients, there were two schools of thoughts. One group saw the glass half full (@uretericbud, @nickbrookMD) and the other group saw the glass half empty (@RFowlr, @drphil_urology).
@uretericbud and @RFowlr had a somewhat contrary views on the matter.




There was a discussion regarding appropriate selection for RPLND and the conclusions of this exchange was nicely summarised by @scientistatlrge
Overall, this was a high quality discussion for our first ever journal club paper on testicular cancer. The Best Tweet Prize was supported by the European Association of Urology (@uroweb) who have kindly offered a complimentary registration to the #EAU15.
The winner was @nickbrookMD who nicely put forward his argument for surveillance



We look forward to seeing you join us for the next #urojc which commences on 4/5 January 2015 depending upon your time zone. Do follow @iurojc for updates.
Yuigi Yuminaga @Yyuminaga is an advanced urology surgical trainee at the Sydney Adventist Hospital in Sydney, Australia.


On the 16-17th February 2015 ten leading robotic centers of excellence from 4 continents will broadcast for 24 continuous hours. All the surgeons operating are experienced live surgeons, pioneers in their fields, who have contributed to the development and advancement of excellence in robotic surgery techniques.
Register now at www.wrse24.org
 |
| WRSE24 incorporating 10 world leading robotic centres. |
“Imagination is more important than knowledge. For knowledge is limited to all we now know and understand, while imagination embraces the entire world, and all there ever will be to know and understand.
We live in exciting and progressive times in healthcare, when technological advancements are rapidly changing the way we work and the way we learn as surgeons. Many of these technological advancements come from discoveries and innovations made outside healthcare, making the pace of change less predictable. For example, it is well known that the advancement of robotic surgery technology came from initial innovative developments made within NASA and further funded and developed by the US military [ref 1].
With the advent of minimally invasive surgery utilizing video technologies, opportunities for surgical learning greatly improved. No longer was surgical training a master-apprentice role, performed behind ‘closed doors’ with the associated limited opportunities to disseminate expertise. Video recording of surgery enabled wider dissemination of knowledge and live surgical video transmissions have revolutionized the way that national and international surgical conference meetings are now run.
Following the recently published ‘‘EAU Policy on Live Surgery Events’’, it is now assured that live surgery will be ongoing at conferences in the immediate future. However, the panel reached >80% consensus on the view that performing at a home institution may be safer. The committee also identified issues with a ‘‘travelling surgeon’’ performing complex surgery in an unfamiliar environment with a surgical team that is not experienced with the intricacies of the surgeon’s technique. LSE’s from a home institution remove or minimize these negative aspects [Declan Murphy]. Furthermore, there are other important reasons why LSE’s are enhanced when performed at a high- volume home institution. The potential to optimise surgical performance comes from working with an experienced team. Consistency is a key measure of quality, and robotic surgery in particular epitomises teamwork. An established theatre team will move purposefully through the standardised steps with well-rehearsed, orchestrated movements. It is therefore likely that the natural evolution of LSE’s, is that a greater proportion are broadcast from home institutions [Collins et al].

We aim to highlight the benefits of this approach to surgical training with a worldwide team who will represent the best of current standardized surgical technique. All the surgeons operating are experienced live surgeons, pioneers in their fields, who have contributed to the development and advancement of excellence in robotic techniques.
We will be coordinating the broadcasts using LiveArena hardware and infrastructure. LiveArena are currently, primarily a sports broadcaster and in partnership with Microsoft have developed, cutting edge video streaming technology that enables streaming of HD video onto the internet, whilst requiring minimal capacity (3Mb/sec). The videos can be watched in real-time and also paused or rewound via their link and the video can be viewed on laptops, PC’s, smart phones and tablets even on standard hospital wifi, making this approach very accessible and scalable.
Communication with surgeons in real-time:
There will be a blog set up on the WRSE24 website, that any doctor registered can ask questions or highlight a topic for discussion. Questions can also be posted via this BJUI blog or via Twitter #WRSE24. During the 24 hour transmission Karolinska will monitor these aspects, combining the discussions and providing regular feedback via a 24 hour ‘overview’ broadcast on a separate channel.
To see more details and to register now for this historic event go to www.wrse24.org
Registration is currently free and urologists who register before the 12th January will be entered into a prize draw for 5 donated robotic courses (3 ERUS 2015 courses in Barcelona, one at USC Keck Medical Center in Los Angeles and one at Peter MacCallum Cancer Centre, Melbourne)




Justin Collins is a Urologist at Karolinska University Hospital. @4urology

Test yourself against our experts with our weekly quiz. You can type your answers here if you want to compare with our answers.
This image is taken from an article on interstitial cells in the ‘Science Made Simple’ section (Fry, BJUI 2014)
No such quiz/survey/poll

{kind=link}