Every Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video from Dr. Giorgio Russo, discussing his paper.
If you only have time to read one article this week, it should be this one.
Increase of Framingham cardiovascular disease risk score is associated with severity of lower urinary tract symptoms
Giorgio I. Russo, Tommaso Castelli, Salvatore Privitera, Eugenia Fragala, Vincenzo Favilla, Giulio Reale, Daniele Urzı, Sandro La Vignera*, Rosita A. Condorelli*, Aldo E. Calogero*, Sebastiano Cimino and Giuseppe Morgia
Department of Urology, and *Department of Medical and Paediatric Sciences, Section of Endocrinology, Andrology and Internal Medicine, University of Catania, Catania, Italy
OBJECTIVE
To determine the relationship between lower urinary tract symptoms (LUTS)/benign prostatic hyperplasia (BPH) and 10-year risk of cardiovascular disease (CVD) assessed by the Framingham CVD risk score in a cohort of patients without previous episodes of stroke and/or acute myocardial infarction.
PATIENTS AND METHODS
From September 2010 to September 2014, 336 consecutive patients with BPH-related LUTS were prospectively enrolled. The general 10-year Framingham CVD risk score, expressed as percentage and assessing the risk of atherosclerotic CVD events, was calculated for each patient. Individuals with low risk had ≤10% CVD risk at 10 years, with intermediate risk 10–20% and with high risk ≥20%. Logistic regression analyses were used to identify variables for predicting a Framingham CVD risk score of ≥10% and moderate–severe LUTS (International Prostate Symptom Score [IPSS] ≥8), adjusted for confounding factors.
RESULTS
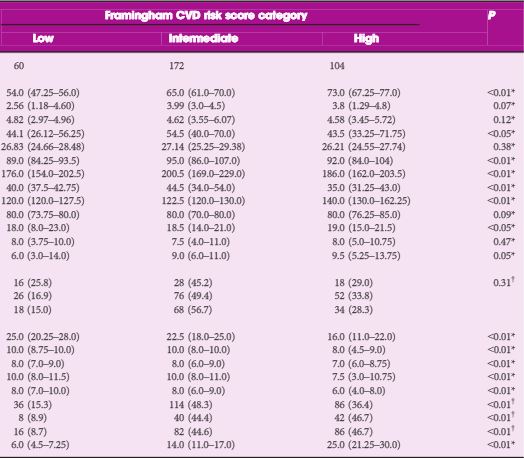
As category of Framingham CVD risk score increased, we observed higher IPSS (18.0 vs 18.50 vs 19.0; P < 0.05), high IPSS–voiding (6.0 vs 9.0 vs 9.5; P < 0.05) and worse sexual function. Prostate volume significantly increased in those with intermediate- vs low-risk scores (54.5 vs 44.1 mL; P < 0.05). Multivariate logistic regression analysis showed that intermediate- [odds ratio (OR) 8.65; P < 0.01) and high-risk scores (OR 1.79; P < 0.05) were independently associated with moderate–severe LUTS. At age-adjusted logistic regression analysis, moderate–severe LUTS was independently associated with Framingham CVD risk score of ≥10% (OR 5.91; P < 0.05).
CONCLUSION
Our cross-sectional study in a cohort of patients with LUTS–BPH showed an increase of more than five-fold of having a Framingham CVD risk score of ≥10% in men with moderate–severe LUTS.