
Posts

#AUA15 bursts to life in New Orleans
Creole cuisine, bustling Bourbon street, beads and beignets and 16,000 urologists. #AUA15 has just drawn to a close in the birthplace of Jazz; New Orleans, Louisiana #NOLA. With 2,598 abstracts being presented, over 2,500 speakers and representation from more than 100 countries it was undoubtedly an educational and action packed five days.

This was my first AUA and while I knew it was going to be a big conference I was stunned by the size of it all. There were urologists everywhere, so much so that jiving to jazz on Frenchman became a game of ‘spot the urologist’ by the signature urology dance moves and stylish….ish dress code!!!! The scientific programme was so extensive it was difficult to find the time to attend all the sessions I wanted to. However, the committee deserve huge credit for developing the AUA2015 app and Daily news snippets that were available throughout the centre which made it easy to optimise your time at the meeting.


The French Quarter, NOLA
The conference got off to a heated beginning with the Crossfire: Controversies in Urology session sparking plenty of debate. Few topics have ignited as much argument as the question of focal ablation for prostate cancer and the discussion between Mark Emberton MD, UCL, London and Aaron E. Katz, MD,PhD, Winthrop University Hospital was no different. To call it a lively session is an understatement. The question of alpha blockers being sold over the counter for BPH was also discussed during this session. Although the drugs have proven safe over the last 25 years clinicians have concerns that the loss of patient contact as a result of this relabeling would causes a loss of control in the treatment of men with BPH.
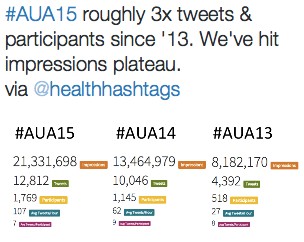
Friday drew to a close with the urotwitterati enjoying the social media TweetUp encouraging newbie tweeters to get involved. It clearly worked because #AUA15 set a new record and almost trebled it’s tweeting volume since #AUA13.
Day two, Saturday saw the opening of the Science and Technology hall. A spectacle of testicular, penile devices and stalls I have never seen. I fear what one might have thought had they stumbled into the conference centre by accident!!



The @BJUIJournal #SoMe awards took place on Saturday evening. @DrHWoo deservedly bagged The Social Media Award 2015 for #UROJC. A well chosen venue there were no issues with Wifi for tweeting!!! Read the #SoMe blog for all award details

Enjoying the @BJUIjournal cult #SoMe awards


A personal favourite of mine at the conference was the 4th annual Residents Bowl which took place over three days; with residents engaging in a battle of the brains! Northeastern claimed the trophy in the end and team members on the winning side included this year’s BAUS representative @DerekHennessey.
BAUS, BJUI and USANZ came together on Sunday afternoon for a stellar line-up of speakers and topics. The session was well attended and speakers outlined the most recent data but more importantly shared the experience of techniques and outcomes in their centres and countries. I think this combined society session is a fantastic arena for all to both learn and educate each other on what is working best, where and why? The superb line up included Dan Moon, Jeremy Grummet, Henry Woo, Declan Murphy, David Nicol, Damien Bolton, Stephen Boorjian and Philip D. Stricker who all shared their clinical expertise.
BJUI Guest speaker Ben Challacombe discussed the evidence base for management of RCC by partial nephrectomy. Lower intraoperative complications and WIT were observed at their centre at Guy’s Hospital London, which is similarly reflected by low complication rates in the BAUS mandatory UK national nephrectomy audit. Professor Prokar Dasgupta started his up and down journey for the evidence supporting robotic cystectomy for TCC bladder by reminiscing on where it all began; kite-flying in India as a young boy.
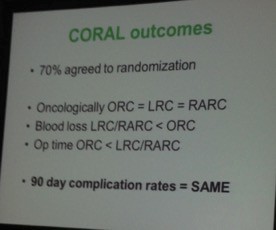
Much anticipated CORAL trial found that 90 day complication rates and oncological control were comparable in ORC v LRC/RARC.

Finally the session closed with the presentation of the Coffey-Krane award to Gopa Iyer; Phase III Study of everolimus in metastatic urothelial cancer collected on Dr Gopa’s behalf by David Quinlan. This award is for trainees who are based in the Americas and judged by a panel as the best publication accepted to the BJUI.
Overall, some of the big points of the conference were the amendments to AUA guidelines including Castration-Resistant Prostate Cancer, which was updated from just last year. Perhaps, the most significant was the first ever draft of AUA Peyronie’s disease guidelines; outlining recommendations from medical therapy to surgery.
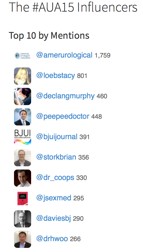
The huge rise in social media at urology conferences was demonstrated again by record-breaking figures via @symplur showing that the use of Twitter among the urology community continues to grow:
#AUA15 was both an educational and social experience. I had a blast, learned loads and also got to experience the culinary delights of Muffuletta and Gumbo, take the trolley up St. Charles to the Garden district and simply encounter the warmth and friendliness of both the Louisiana folk and the huge family of Urology. The AUA Scientific Committee deserve a huge congratulations on the success of a stimulating, enjoyable and extensive scientific programme. I know I heard echoes of ‘best AUA yet’ in my company.
Áine Goggins
Medical Student; Queens University Belfast, Ireland
@gogsains
Guideline of Guidelines Poll Results

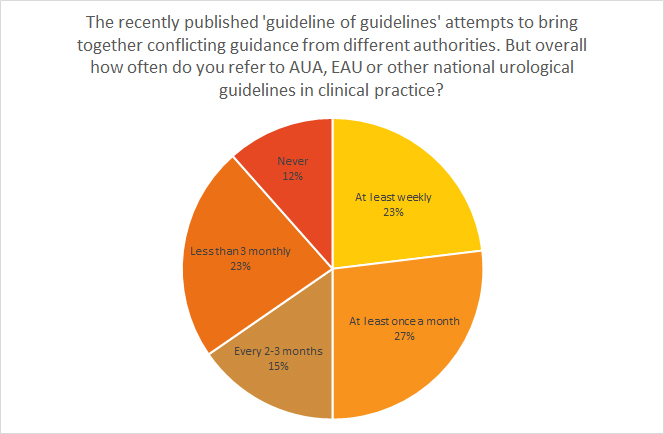
The recently published ‘guideline of guidelines’ attempts to bring together conflicting guidance from different authorities. But overall how often do you refer to AUA, EAU or other national urological guidelines in clinical practice?
At least weekly – 23%
At least once a month – 27%
Every 2-3 months – 15%
Less than 3 monthly – 23%
Never – 12 %

5 Questions with Per-Anders Abrahamsson and Gopal Badlani
Secretary Generals to the big Spring Meetings, European Association of Urology and the American Urological Association
Every Spring, thousands of urologists gather in big cities with mega-venues to attend one or both of the annual congresses of the EAU and the AUA. These are big events with respect to release of the latest scientific trials, instructional courses, plenary sessions, and of course multiple ways to see and interact with advances in industry partners. But who orchestrates these massive events occurring over multiple days? Of course it requires a full team of expert staff members, and in both groups, they employ an outstanding Urologist to a multi-year contract to serve as secretary and be a principle organizer of the annual meeting. We asked each secretary general to share their perspectives with 5 questions.

Gopal Badlani–Secretary to the AUA 2011-2015. The New Orleans AUA will be Prof. Badlani’s last as AUA and will certainly be an exciting meeting and fitting celebration to an excellent term of service and creative updates to the annual meeting.
1) What excites you about your meeting format and location?
PAA: Stockholm of course is a major draw, but we don’t know if it will be Spring or Winter at the time. Forty percent of our draw is from beyond Europe—Latin America, China, and India. We know that Stockholm is an exotic city worth the trip, but hopefully they find the meeting and the quality of education worth the trip. Stockholm is recognized as one of the best venues, and our office staff knows venues across Europe. The problem here is that the Swedish economy is booming and its one of the most expensive cities in the world. We were able to downsize the hotel prices, but its very expensive. In addition, Pharma support for attendees has dropped from 80% to 60%. The weather has been rather decent.
GB: We changed our format this year to incorporate Friday as the first official day of the AUA Annual Meeting, showcasing a full day of research programs and a highly successful Crossfires: Controversies in Urology program. It certainly generated “buzz” and continued discussions surrounding such controversies throughout the meeting.
2) What about high impact studies being presented?
PAA: One coming up is the PREVAIL study with Enzalutamide “Pre-chemo”. We also have our own Swedish national cancer registry and there are some data coming out favoring early treatment of prostate cancer. This is one of the oldest in the world. Peter Wiklund will present this. Another that will be updated Tuesday is the European randomized screening trial. The principal investigator after Fritz Schroeder is Jonas Hugosson from Gothenberg. He got permission from Lancet to update the Swedish arm of that trial. You will find differences between centers and there will be an update with longer follow-up.
GB: Our plenary sessions highlighted late-breaking news, new AUA clinical guidelines and the latest advances in urologic medicine. It was in this forum, we heard from Dr. Anthony Fauci on ending the HIV/AIDS pandemic and its lifecycle from scientific advances to public health implementation.
It was also where attendees heard from Dr. Ajay Nangia about the adverse effects of common medications on male fertility to outstanding sessions on benign disease, the challenges in managing spinal cord injury patients with neurogenic bladder as well as mesh use for urinary incontinence (Drs. Flynn and Rovner).
Our International Prostate Forum more than tripled anticipated attendance. Dr. Andrew Schally, a recipient of the Nobel Prize in Medicine, as well as a number of experts from around the world, provided global perspectives on prostate cancer.
Eight debates on today’s hottest topics in urology were showcased through our standing-room only Crossfire-Controversies in Urology event. Our Town Hall transported attendees into the future of simulated surgical training and imaging. This session included presentations from experts and pioneers in 3D and molecular imaging as well as surgical simulation.
3) What are key metrics of the meeting?
PAA: We have 120 countries represented. Registration is about 700 off from Milan last year, but are pleased overall given the expense noted, and sponsorship from Pharma continues to decrease.
GB: Our meeting continues to attract over 15,000 attendees from over 120 countries. More than 2,200 abstracts were presented and more than 2,500 speakers.
4) What are key trends important to Urologists attending your meeting? Why do they attend?
PAA: There is a need for meetings like this for people to meet and to start up multi-institutional trials, even trans-Atlantic. We hope to facilitate translational research. For example, we facilitated the first ever World Chinese meeting—Taiwan, Hong Kong, and Mainland—all together, and very difficult to organize from a political viewpoint. We were very pleased with this and left politics aside.
GB: There are a number of major concerns affecting American urologists, including issues affecting fair and appropriate payment (e.g., the sustainable growth rate, or SGR, the formula which is used to set Medicare payments for U.S. physicians), certain provisions under the Affordable Care Act (such as the 90-day grace period for recipients of advanced payments in the large group health insurance market places) and the impact that unfunded mandates such as prior authorizations, required accreditations, etc., have on our practices. All of these issues are compounded by the fact that our U.S. physician workforce is shrinking and, unless significant steps are taken to fundamentally reform graduate medical education, the country will have an insufficient supply of physicians to adequately meet patients’ needs in a timely manner. This shortage is of specific note to urology, since we have the second-oldest surgical subspecialty workforce, and limits on funding for urology residency programs make it extremely difficult to get more medical students into urology residencies.
5) What are your impressions of the venue and city?
PAA: Honestly I was not involved in that decision-making. We have 70 people working full time in our office in Holland. We had our own congress consultants working, looking at new venues. We have mainly concentrated our annual congress to limited venues—Madrid, Barcelona, Paris, Vienna, Milan, London in the future, and in Germany Munich and Berlin. Scandinavia so far its only been Stockholm as we can take care of 15,000 people here and we have a good congress venue. In the future it will be Copenhagen as they have a new congress venue that is closer to Europe. So we are going to rotate between these venues. We have not been able to find a venue in Eastern Europe that accommodates that many people.
GB: We enjoyed being in sunny, warm Orlando in May. Orlando has a good mix of hotels to offer to our attendees – from an impressive full service Ritz Carlton to a few lower cost options such as the Days Inn and Marriott Courtyard. Overall, I think the Orlando Convention Center worked well for us. Looking forward, the excitement is in the air surrounding next year’s location, New Orleans May 15-20, 2015. Program planning begins this summer!
So there you have it. While most of us run around these meetings trying to figure out which session suits our interest, or where we have to moderate/speak next, the secretaries have a very different perspective. They worry about meeting formats, costs, weather, who will show up, what will they think. I was also impressed that while most of us tend to network on the fly by just walking around the venue and bumping into colleagues, the secretaries have very tight schedules run by their staff. I appreciate the time both gave to us. Note that the answers may flow differently as Per-Anders did a sit down interview with an iPhone recorder running, while Gopal gave me typed answers after the meeting.
Thank you to both secretaries on strong annual congresses.
John W. Davis, MD, FACS
Associate Editor, BJUI
AUA 2014 – Monday, Tuesday, Wednesday: “The Tweeter’s Congress”
Thanks to @rmehrazin and @uroncdoc for a great summary of the first three days of #AUA14. This year’s meeting has been a phenomenal success, especially with regards to Twitter use during the Congress and the dissemination of content surrounding the meeting. You know how it goes – ‘sorry I can’t catch your session because I have to be somewhere else’. Well not anymore. Keep the #AUA14 search feed on your Twitter app, and the stream of information on posters/podiums or plenary was tremendous! One could be at multiple sessions at the same time. Indeed, Twitter use compared to last year’s meeting has increased by over 100%. Just as Tony Blair coined the term ‘the people’s Princess’ for Princess Diana – I am calling #AUA14 ‘the Tweeter’s congress’. In honour of that, I have created ‘Twitter-grams’ around themes. As the conference has too much to cover, I will concentrate on the big plenary sessions.

Twitter-gram 2: PCNL
Further plenary included the EAU lecture by Mr Marcus Drake on the management of LUTS. He announced the protocol of a European RCT enrolling 800 patients assessing invasive urodynamics versus noninvasive tests in men undergoing surgery for bladder outlet obstruction. This was followed by Dr Quentin Clemens, from @umichurology and Chair of the multidisciplinary approach to the study of chronic pelvic pain (MAPP) network. The objectives of this impressive multi-institutional study are to address underlying disease pathophysiology and natural history utilizing patient cohorts, biospecimens and animal models, as well as provide new information to inform patient management and future clinical trial design. More details can be found here.
The plenary then wrapped up with a discussion of the new AUA guidelines from Dr Morey on urotrauma and Dr Pearle on medical management of stone disease. Both can be viewed here:
Urotrauma
Medical management of kidney stones
Some important points from the urotrauma guidelines:
- Imaging is necessary – immediate and delayed
- Indications for renal trauma imaging include gross hematuria, microscopic hematuria and systolic blood pressure <90, or mechanism of injury suggest high index of suspicion.
- Stable patients be managed non-invasively
- For renal injuries Grade 4 or greater – follow-up imaging is advised
- For ureteral trauma, immediate repair is indicated if complete injury and recognized in the operating room
- In unstable patients, ureteral trauma can be managed with temporary urinary drainage
- In presence of gross hematuria and pelvic fracture – patient must have cystography
Some important points from the medical management guidelines:
- Thiazides are indicated in patients with recurrent calcium stones and hypercalciuria
- Potassium-citrate therapy should be offered to patients with hypocitraturia and recurrent calcium stones
- In patients with recurrent calcium stones and absence of metabolic abnormalities, both thiazides and potassium citrate should be offered
- Allopurinol should be prescribed to patients with recurrent calcium stones elevated urinary uric acid and normal urinary calcium. It should not routinely be prescribed as first line therapy for patients with uric acid stones
- In terms of follow-up, a 24 hour urine collection should be performed within 6 months of initiating treatment and at least annually thereafter

Monday – Townhall session
The ‘townhall’ session this year contained urology and non-urology experts who were questioned by the audience via text messages (but not Twitter! @AmerUrological). This session was moderated by Dr Inderbir Gill, and included experts from Hollywood on 3D imaging, a neuroscientist, molecular imaging scientists and surgical simulation pioneers. The session began with a talk on tissue level imaging in 3D, followed by Dr Tewari (@nycrobotics) introducing us to his research on visualizing nerves during robot-assisted radical prostatectomy. Dr Narula, Editor of the Journal of Cardiovascular Imaging, then gave a fascinating talk on “Who gets the Heart Attack? Imaging from Bench to Bedside and from Mummies to Population”. At the end of his talk, I had a strong urge to get my cholesterol checked as well as demand a CT angiogram. The simulation debate was entitled – “The giants of the past don’t need no stinkin’ simulators” – and was between Dr Carl Olsson (Against simulation) and Dr Robert Sweet (For). Dr Olsson was the man with all the right jokes, while Dr Sweet’s slides malfunctioned; although it was clear to the audience that in this era of reduced hours training, simulated surgical training is becoming the norm. Finally, only at the AUA meeting can you get the team behind 3D rendering for Hollywood provide an insight into the methodology of rendering. We all put on 3D glasses and watched a short clip of the film “Need for speed” in glorious 3D.
Tuesday – plenary
The morning began with a panel discussion between some very well known urologists on robotic vs. open robotic cystectomy. First on, Dr Hautmann argued against robotic cystectomy: “Optimal function was more important than the length of the incision or time to flatus”. He also argued there was a selection bias in robotic series, with healthier patients tending to be selected for robotic surgery. He closed by quoting Einstein: “make things as simple as possible but not simpler than that”.
Next was Dr Pruthi, an expert on robotic cystectomy. He felt the benefit of a robotic intracorporeal diversion was fewer GI complications, readmissions, and the potential to reduce ureteral stricture because of less ureteral mobilization with the robotic approach. While the ileal conduit robotically was simple and straightforward, he admitted he was unsure of robotic neobladders as this was more complex. The session closed with a frank statement by Dr Jay Smith, “It is unlikely any substantial difference in outcome will emerge between robotic vs open cystectomy”. However, he felt robotics was here to stay, as it was doubtful if the next generation of urologists would have the skills to obtain high-level open cystectomy results.
The plenary then resumed with the theme on PSA testing, and started with a panel discussion on tests to distinguish aggressive from non-aggressive prostate cancer before biopsy. Dr John Wei (@jtwei88) from @umichurology, spoke about the Michigan Prostate Score (MiPS) – a composite score consisting of three tests: PSA, urine T2:ERG gene fusion, and urine PCA3 level. Later on, to a jam jam-packed hall, Dr Penson (@urogeek), from Vanderbilt, delivered a state-of-the-art lecture on PSA testing guidelines. This excellent talk generated lots of Twitter traffic, which is illustrated in the Twitter-gram.


Wednesday – take home messages and wrap-up
The final day was not as busy as the other days as most delegates and all exhibitors had left. I too had to get back to work, but I was still able to catch up with #AUA14 via the twittersphere (thanks @chrisfilson). The best of the tweets from this last day are depicted in the final twitter-gram. I also recommend @cbayneMD for his top 5 conference highlights.
[caption id=”attachment_15430″ align=”alignnone” width=”1024′ label=’ Twitter-gram 4: final day

Overall, #AUA14 has been a fantastic conference, where records were set for Twitter participation and engagement in a urological meeting. I am still recovering!
Khurshid Ghani
University of Michigan, Ann Arbor, USA
@peepeeDoctor

Social media traffic broke all records at #AUA14 with over 1100 participants sending over 10,000 tweets and making almost 14 million digital impressions.

AUA 2014 – Friday, Saturday, Sunday: Orlando, FL
As my flight descends into the home of Walt Disney and make believe in sunny Borelando, I can’t help wonder how #AUA14 will compare to the outstanding #EAU14 meeting held just one month ago. A great meeting requires equal parts place and content, and although Stockholm is without peer, there must be a reason Orlando is the third most visited city in the U.S., right? The solution to that mystery is for another day; ask elsewhere, as I have no idea. Review of the agenda on the #AUA14 app gives hope for this meeting. There is more quality scientific content than one can possibly absorb, and highlights include the new “Crossfire” program to address controversies in urology, the John K. Lattimer Lecture by Dr. Anthony Fauci (director of the National Institute of Allergy and Infectious Diseases), the Town Hall on imaging, simulation and animation (with speakers from Hollywood who make make-believe a reality and a living), #SUO14, and the release of three new AUA Guidelines on urotrauma, medical management of stones, and cryptorchidism.
Friday afternoon kicked off with the new “Crossfire” section featuring debates on a number of heated urology controversies. Debate topics included the use of synthetic slings for stress urinary incontinence (SUI), the role of urologists in administration of therapy for advanced and metastatic prostate cancer, and the probably overly discussed topic of open versus robotic surgery (for both partial nephrectomy and radical prostatectomy). In favor of synthetic mid-urethral slings for SUI, Drs. Kennelly and Rovner presented a wealth of data showing the efficacy of slings in both the short and long term. Drs. O’Connell and Blaivas countered that the pubovaginal fascial sling provides a safer alternative, with less potentially significant complications that far outweigh the benefits of having the operation.
Drs. Nelson and Lepor then argued in favor of open prostatectomy, which drew some colorful tweets:

Drs. Tewari and Menon presented compelling arguments for robotic prostatectomy, and while it is hard to declare a winner, the majority of urologists in the U.S. perform robotic assisted prostatectomy; the panelists stressed that outcomes depend more upon the surgeon than the technique, and people should perform whichever approach they are most comfortable with.
The robotic versus open debate then shifted to kidney surgery, with distinguished faculty Drs. Gill and Uzzo debating “minimally invasive partial nephrectomy is the new gold standard for renal cancer”, while Drs. Blute and Libertino argued in favor of open surgery. Although both sides had thought provoking arguments, presented data were all limited by their retrospective designs, institutional experience, or lack of validation. In my opinion, even with high volume surgeons, most patients with highly complex tumors or a renal mass in a solitary kidney undergo open surgery, which implies selection bias that limits the generalizability of robotic or laparoscopic partial nephrectomy. As contemporary experience with robotic surgery grows, we can anticipate that more complex lesions will be approached via MIS techniques in the future. We always love to throw in “randomized clinical trials are needed”… although I do think that IDEALLY prospective evidence would be great, however a clinical trial comparing MIS partial Nx to open techniques will be fraught with accrual challenges and are most likely not expected in the near future. Until more definitive prospective evidence is available, decisions regarding the optimal surgical approach for the renal mass should be determined by individual patient and surgeon preference, experience and comfort level.
Following the debate, Dr. Todd Morgan nicely summarized audience sentiment:

Dr. Declan Murphy provided perhaps the best sage advice regarding robotic versus open surgery:

Social Media continues to grow in urology, and Friday evening concluded with a wonderful party hosted by the AUA (@Americanurol) for the “UroTwitterati”. There was a great turnout, and #SoMe heavy hitters: @daviesbj, @declangmurphy, @dr_coop, @qdtrinh, @TheUrologist, @LoebStacy, and @Tdave attended along with “wannabe” youngsters (your current bloggers, @UROncDoc and @RMehrazin). The beauty of #SoMe is that it even allows members to participate in the meeting from home, including @uretericbud and @dytcmd. Urologists should sign up for a Twitter account and join. It is very engaging and addictive!

The jam-packed schedule continued on Saturday morning with the annual residents forum, during which the resident teaching award was awarded to Dr. Robert Uzzo from Fox Chase Cancer Center.

A variety of sections and societies also held meetings on Saturday. At the Association of American-Iranian Urologists, panelists Drs. Ghavamian and Samadi discussed the role of focal therapy in prostate cancer.

The remainder of Saturday was largely filled by the Society for Basic Urological Research and Society for Urological Oncology annual meetings. One highlight of the #SUO meeting was Dr. McDermott’s presentation on anti-PD-1 agents in kidney cancer. In a phase 1 RCT, Nivolumab (anti PD-L1 agent) showed efficacy for patients with metastatic RCC (n=34). There was a 29% objective response rate with a median progression-free survival time of 7.3 months. The drug was well tolerated with minimal severe adverse events, and remarkably, treatment free survival was achieved in a few patients. Immunotherapy represents an exciting and novel way target kidney cancer, and may well help usher in the era of personalized targeted therapy.
On Sunday, multiple poster and podium sessions were occurring simultaneously, which makes it hard to attend and see everything. The discussion on Twitter via #AUA14 made it possible to capture highlights from simultaneous sessions. During the Plenary session on Sunday, Dr. Fauci, Director of the National Institute of Health, Allergy and Infectious Disease Division, gave the annual Lattimer lecture. AIDS is an important topic for urologists because several aspects of the disease are specific to urology. “For example, the role of STD’s in increasing the transmissibility as well as the vulnerability of getting infected with HIV, the potential role of HPV vaccine in preventing HIV infection, and the importance of urologist issues associated with the drugs HIV patients are taking, including stones, renal insufficiency, voiding dysfunction, and erectile dysfunction,” remarked Dr. Fauci.
John P. Mulhall, Director of Male Sexual Health and Reproductive Medicine at Memorial Sloan Kettering Cancer Center, delivered the plenary state of the art lecture on radiation induced erectile dysfunction. It is an important topic, because “there are an increasing number of urologists who have hired a radiation oncologist or have a stake in an IMRT unit or do brachytherapy in their practices”, remarked Dr. Mulhall. “The pathophysiology of ED after pelvic radiation is very similar to that after radical prostatectomy based on three factors: nerve injury, arterial injury, and smooth muscle injury”.
The new AUA clinical guideline for cryptorchidism was also presented at the plenary session on Sunday. The highlights of the guideline:
- Orhiopexy is the gold standard treatment for cryptorchidism in 2014
- Initial radiographic studies are not necessary for the child with cryptorchidism
- Surgery should be performed from 6 to 18 months after birth
- Hormonal therapy should not be used as primary therapy to attempt to reposition the testis in the scrotum
Your bloggers,
Reza Mehrazin, M.D. and Jeffrey J. Tomaszewski, M.D.
Fox Chase Cancer Center, Philadephia, PA
Twitter @rmehrazin and @UROncDoc


You are Not Connected to the Internet: Seeking Stable WiFi at the Modern Conference
Urologists the world over have at last settled back into their rhythms after congregating en masse in San Diego, California for the American Urological Association Annual Meeting. While I hadn’t expected to escape balmy Ontario for crisp breezes in Southern California, the setting was an excellent one.
This year’s AUA meeting had all the hallmarks of years past – heaving throngs of AUA-branded-faux-leather-bagged urologists speed-walking between sessions in the enormous SD Convention Centre, bleary-eyed sufferers burning away their respective fogs with espresso in the cavernous Exhibit Hall, and plenary sessions packed to the gills to hear the latest and greatest. One pernicious tradition was unfortunately manifest again, however, in the form of unreliable wireless internet access in the conference hall and ancillary venues.
Modern conferences and conference centres (where (ironically) the latest technologies and scientific advances are presented) seem to have barricaded themselves from the digital world the modern conference-goer inhabits. This may at first seem inconsequential, as the sequestration and forced attention might keep the focus on the presented data. In truth, an entire communication meta-layer, that of the conversations, opinions and dissemination created by social media activity, are needlessly compromised.
As has been stated repeatedly in social media circles, this year’s annual meeting was a bonanza of twitter activity at the #aua13 hashtag, with over 4000 tweets sent from 468 users during the meeting proper. The recent European Association of Urology meeting in Milan was similarly well subscribed, with almost 1800 tweets from 251 users.
It seems universal at urology (and doubtless other disciplines’) meetings that some of the earliest twitter activity centers around the pain of spotty or absent wifi. To wit:
– from #uro12 (AUA Atlanta):

– from #eau13 (EAU Milan):

– from #aua13 (AUA San Diego):

These are but a few of the dozens of agonized tweets based on weak, spotty or absent wifi, and for each there is doubtless a dozen, fifty, a hundred more people in the same building steaming with the same frustrations. International delegates, loathe to “roam” outside their home data plans, are perhaps the most handicapped. One imagines the conference centre tech team testing their seemingly robust signal in an empty room, devoid of the hundreds or thousands of devices queuing for bandwidth space once the meeting is in full swing. And let’s not forgive the conference-adjacent hotels that host dozens of ancillary meetings, such as the well-attended Society of Urologic Oncology meeting, each year in advance of the AUA proper. Typically there is a total absence of available wifi in these conference halls. In 2013, the mind boggles at this omission (on the part of organizers as well as the hotels).
Certainly the modern conference centre and the modern meeting must see beyond their own walls, and address the modern realities of communication. The reach of social media, and indeed the basic need of busy attendees to connect with their practices, lives and colleagues make this all the more imperative. Relative to all the other logistic feats that underpin a conference, building in extra bandwidth (with redundancy to avoid catastrophe) should be a simple infrastructure and expenditure issue, well within the means of the centre to predict and to deploy.
A brief set of expectations for the modern conference centre’s wireless internet:
- Conference wifi must be available to all who wish to access it, when and where they wish to do so. Hotels are not exempt if they host parts of the meeting. Wifi is no longer a perk or a luxury.
- Login should be simple and able to be performed in the native settings of the users’ devices, rather than the agonizing experience of web- or browser-based login.
- Requiring repeated logins when re-entering rooms or buildings is excruciating and anathema to the speed of communication and discussion that define social media. One formal login per device per meeting.
- The ubiquity of mobile devices may require a building retrofit or construction of stations to facilitate the ability of delegates to charge these devices.
Until these conditions are met, associations, conferences and conference centres will be forced by their own inertia to stifle the full potential of the meetings they host. Here’s hoping that the volume of our discontent is heard by organizers, and suitable guarantees are established and met as conditions of hosting our meetings.
Mike Leveridge is an Assistant Professor in the Departments of Urology and Oncology at Queen’s University, Kingston, ON, Canada. @_theurologist_
Comments on this blog are now closed.

The BJUI Social Media Awards 2013
The BJUI has been very pleased with the large amount of social media activity we have seen across our various platforms since January 2013 when the new-look Journal was introduced. Editor-in-Chief, Prokar Dasgupta, has decreed that he wants the BJUI to be “the most-read surgical journal on the web”, and has recognised the key role that social media plays in realizing this ambition. At the same time, the social media revolution that has engrossed Gen Y and Gen Z and which has transformed the way in which news is communicated, has now taken a foothold in scientific publishing and is evolving.
To recognise the rapidly growing interest in social media in urology, and also to acknowledge those who have played a major role in advancing social media in urology at the BJUI and elsewhere, we this year inaugurated the BJUI Social Media Awards, presented for the first time at the AUA recently. Individuals and organisations were recognised across 20 categories including the top gong, The BJUI Social Media Award 2013, awarded to an individual or organization who has made an outstanding contribution to social media in urology in the preceding year.
This year’s Awards Ceremony was held in the Dublin Square Irish Bar in San Diego during the AUA Annual Meeting. Sixty of the World’s leading social media enthusiasts (the “Uro-Twitterati”), gathered to meet up in person and to see who would be recognised. Sort of like the Oscars but without the wardrobe malfunctions. Yours truly played the role of MC. While most of the awards recognised genuine achievements in social media, there were a few “special” categories which recognised some reasonably strange activity propagated through social media channels!

{kind=link}
Todd Morgan and Alex Kutikov, the brains behind Draw MD Urology and Urology Match who won the top award of the evening.
We were delighted to have recipients from all categories present at the ceremony including representatives from the AUA and EAU. The BJUI Social Media Awards Ceremony was competing with the European Urology Cocktail Reception a couple of blocks away but in the spirit of conviviality which we encourage, we welcomed European Urology Editor-in-Chief elect, Dr Jim Catto, and managing editor Cathy Pierce, who popped in for a drink and to collect the EAU awards.
A special thanks to my research fellow Dr Marni Basto who organised this year’s awards, and to Scott Millar and Helena Kasprowicz at BJUI in London who manage our social media and website activity.
For more pictures from the evening, please visit BJUI Associate Editor John Davies Flickr page.
Declan Murphy is Associate Editor for Social Media at BJUI. He is a uro-oncologist in Melbourne, Australia
Follow Declan on Twitter @declangmurphy
Comments on this blog are now closed.