Article of the Week: Multicentre outcomes of robot-assisted partial nephrectomy after major open abdominal surgery
Every Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video from Craig Rogers, discussing his paper.
If you only have time to read one article this week, it should be this one.
Multicentre outcomes of robot-assisted partial nephrectomy after major open abdominal surgery
Objective
To evaluate the outcomes of robot-assisted partial nephrectomy RAPN after major prior abdominal surgery (PAS) using a large multicentre database.
Patients and methods
We identified 1 686 RAPN from five academic centres between 2006 and 2014. In all, 216 patients had previously undergone major PAS, defined as having an open upper midline/ipsilateral incision. Perioperative outcomes were compared with those 1 470 patients who had had no major PAS. The chi-squared test and Mann–Whitney U-test were used for categorical and continuous variables, respectively.
Results
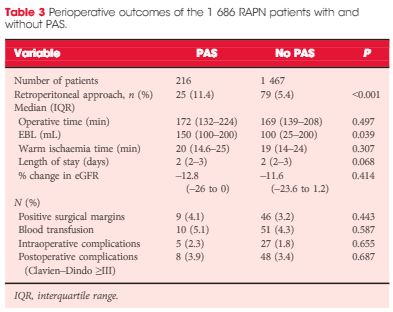
There was no statistically significant difference in Charlson comorbidity index, tumour size, R.E.N.A.L. nephrometry score or preoperative estimated glomerular filtration rate (eGFR) between the groups. Age and body mass index were higher in patients with PAS. The PAS group had a higher estimated blood loss (EBL) but this did not lead to a higher transfusion rate. A retroperitoneal approach was used more often in patients with major PAS (11.2 vs 5.4%), although this group did not have a higher percentage of posterior tumours (38.8 vs 43.3%, P = 0.286). Operative time, warm ischaemia time, length of stay, positive surgical margin, percentage change in eGFR, and perioperative complications were not significantly different between the groups.
Conclusions
RAPN in patients with major PAS is safe and feasible, with increased EBL but no increased rate of transfusion. Patients with major PAS had almost twice the likelihood of having a retroperitoneal approach.