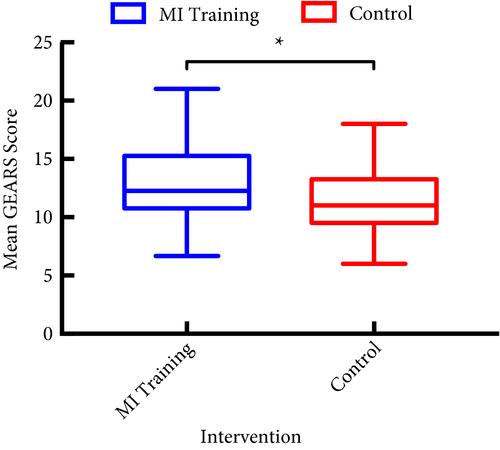
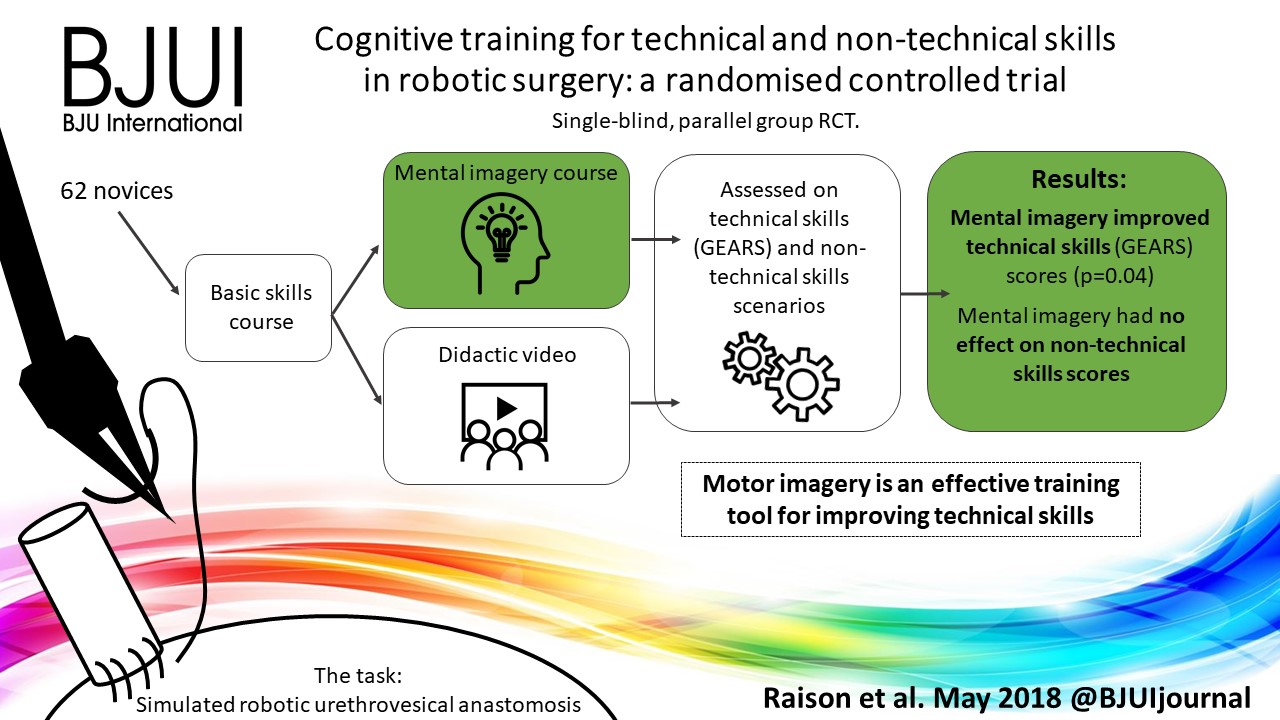
Urethrovesical anastomosis (UVA), like any other surgical anastomosis, is a key example of motor muscle memory, where aligning two hollow structures should result in a watertight anastomosis defining its success and help avoid complications. The authors [1] investigated the importance of cognitive training during UVA, which has been shown to be a promising supplement to skill‐based training. The authors utilised the Global Evaluative Assessment of Robotic Skills (GEARS), which has been validated for assessment of general robotic rather than procedure‐specific skills. As the authors chose UVA to evaluate training, they could have used the Robotic Anastomosis Competency Evaluation (RACE), which has been developed and validated for specific evaluation of UVA [2]. However, the study eloquently revealed higher scores, using the validated movement imagery questionnaire modified for robot‐assisted surgery whilst evaluating mental imagery.
Motor imagery utilises imagining action without its physical execution and this leads to eliciting activity in regions of brain normally activated during performance. Motor imagery has shown significant neural activity in important brain area involved in somatosensory perception, especially kinesthetic information from motor perception and muscle spindles. Such areas become active when a motor illusion is induced that ultimately share the same basis with areas active during executing movement. Mental imagery also yields more benefits if its sessions are interposed between periods of training [3]. Unfortunately, the ability to imagine more complex tasks is less accurate when utilising mental imagery [4]. In future, studies using procedure‐specific evaluation, such as RACE, may help us understand in depth the role of mental imagery during various steps of complex task, such as UVA. The hypothesis of improvement of skills whilst utilising supplemental cognitive training is reasonable; future studies will benefit from utilising an elaborate cognitive assessment. Metrics such as electroencephalograms (EEGs) and eye tracking, or even less sophisticated tools like the National Aeronautics and Space Administration Task Load Index (NASA‐TLX) self‐assessment questionnaires, have previously been used for assessment of cognitive load [5]. Objective feedback provided by a brain–computer interface (BCI) can increase the brain activation levels produced during motor imagery and thereby help in improving performance [6].
Motor imagery has been used as a popular input for BCI and in future could be used as a link to establishing instruction to semi‐autonomous robotic systems [6]. Meanwhile, a motor imagery BCI using EEG is utilising intention recognition through decoding brain activity, which ultimately could allow for intuitive control of devices like robotic systems.
References
- Raison N, Ahmed K, Abe T et al. Cognitive training for technical and non‐technical skills in robotic surgery: a randomised controlled trial. BJU Int 2018; 122: 1075–81
- Raza SJ, Field E, Jay C et al. Surgical competency for urethrovesical anastomosis during robot‐assisted radical prostatectomy: development and validation of the robotic anastomosis competency evaluation. Urology 2015; 85: 27–32
- Nicholson VP, Keogh JW, Low Choy NL. Can a single session of motor imagery promote motor learning of locomotion in older adults? A randomized controlled trial. Clin Interv Aging 2018; 13: 713–22
- Kalicinski M, Kempe M, Bock O. Motor imagery: effects of age, task complexity, and task setting. Exp Aging Res 2015; 41: 25–3
- Besharat Shafiei S, Hussein AA, Ahmed Y, Guru K. Can eye tracking help explain an expert surgeon’s brain performance during robot‐assisted surgery? J Urol 2018; 199 (Suppl.): e1–2
- Batula AM, Kim YE, Ayaz H. Virtual and actual humanoid robot control with four‐class motor‐imagery‐based optical brain‐computer interface. Biomed Res Int 2017; 2017: 1463512.