Every month, the Editor-in-Chief selects an Article of the Month from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an editorial and a video prepared by the authors. These are intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this month, it should be this one.
John W. Yaxley*†‡, Sheliyan Raveenthiran†‡, François-Xavier Nouhaud‡§, Hemamali Samaratunga†¶, William J. Yaxley†‡, Geoff Coughlin*‡, Anna J. Yaxley**, Troy Gianduzzo††, Boon Kua‡‡, Louise McEwan‡‡ and David Wong‡‡
*Wesley Urology Clinic, †Department of Medicine, University of Queensland, ‡Royal Brisbane and Women’s Hospital, Brisbane, Queensland, Australia, §Department of Urology, Rouen University Hospital, Rouen, France, ¶Aquesta Uro-pathology, **School of Medicine, Griffith University, ††Brisbane Prostate Clinic, and ‡‡Wesley Medical Imaging, Brisbane, Queensland, Australia
To determine the number of men with 68gallium‐prostate‐specific membrane antigen positron emission tomography/computed tomography (68Ga‐PSMA PET/CT) avid metastasis at diagnosis, as most data on 68Ga‐PSMA PET/CT are for the evaluation of recurrent disease after primary treatment and to our knowledge this study is the largest series of primary prostate cancer staging with 68Ga‐PSMA PET/CT.
Patients and Methods
A retrospective review conducted on 1253 consecutive men referred by urologists or radiation oncologists to our tertiary referral centre for 68Ga‐PSMA PET/CT scan for staging at the initial diagnosis of prostate cancer between July 2014 and June 2018.
The primary outcome measure was to determine the risk of metastasis based on 68Ga‐PSMA PET/CT. Patients were risk stratified based on histological biopsy International Society of Urological Pathology (ISUP) grade, prostate‐specific antigen (PSA) level, and staging with pre‐biopsy multiparametric magnetic resonance imaging (mpMRI). Univariate and multivariate logistic regression were used to analyse results.
Results
The median PSA level was 6.5 ng/mL and median ISUP grade was 3, with high‐risk disease in 49.7%. The prostate primary was PSMA avid in 91.7% of men. Metastatic disease was identified in 12.1% of men, including 8.2% with a PSA level of <10 ng/mL and 43% with a PSA level of >20 ng/mL. Metastases were identified in 6.4% with ISUP grade 2–3 and 21% with ISUP grade 4–5. Pre‐biopsy mpMRI identified metastasis in 8.1% of T2 disease, increasing to 42.4% of T3b. Lymph node metastases were suspected in 107 men, with 47.7% outside the boundaries of an extended pelvic lymph node dissection. Skeletal metastases were identified in 4.7%. In men with intermediate‐risk prostate cancer, metastases were identified in 5.2%, compared to 19.9% with high‐risk disease.
Conclusions
These results support the use of 68Ga‐PSMA PET/CT for primary staging of prostate cancer. Increasing PSA level, ISUP grade and radiological staging with mpMRI were all statistically significant prognostic factors for metastasis on both univariate and multivariate analysis.
To determine the number of men with 68gallium‐prostate‐specific membrane antigen positron emission tomography/computed tomography (68Ga‐PSMA PET/CT) avid metastasis at diagnosis, as most data on 68Ga‐PSMA PET/CT are for the evaluation of recurrent disease after primary treatment and to our knowledge this study is the largest series of primary prostate cancer staging with 68Ga‐PSMA PET/CT.
Patients and Methods
A retrospective review conducted on 1253 consecutive men referred by urologists or radiation oncologists to our tertiary referral centre for 68Ga‐PSMA PET/CT scan for staging at the initial diagnosis of prostate cancer between July 2014 and June 2018.
The primary outcome measure was to determine the risk of metastasis based on 68Ga‐PSMA PET/CT. Patients were risk stratified based on histological biopsy International Society of Urological Pathology (ISUP) grade, prostate‐specific antigen (PSA) level, and staging with pre‐biopsy multiparametric magnetic resonance imaging (mpMRI). Univariate and multivariate logistic regression were used to analyse results.
Results
The median PSA level was 6.5 ng/mL and median ISUP grade was 3, with high‐risk disease in 49.7%. The prostate primary was PSMA avid in 91.7% of men. Metastatic disease was identified in 12.1% of men, including 8.2% with a PSA level of <10 ng/mL and 43% with a PSA level of >20 ng/mL. Metastases were identified in 6.4% with ISUP grade 2–3 and 21% with ISUP grade 4–5. Pre‐biopsy mpMRI identified metastasis in 8.1% of T2 disease, increasing to 42.4% of T3b. Lymph node metastases were suspected in 107 men, with 47.7% outside the boundaries of an extended pelvic lymph node dissection. Skeletal metastases were identified in 4.7%. In men with intermediate‐risk prostate cancer, metastases were identified in 5.2%, compared to 19.9% with high‐risk disease.
Conclusions
These results support the use of 68Ga‐PSMA PET/CT for primary staging of prostate cancer. Increasing PSA level, ISUP grade and radiological staging with mpMRI were all statistically significant prognostic factors for metastasis on both univariate and multivariate analysis.
Every week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an editorialwritten by a prominent member of the urological community. These are intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this month, it should be this one.
Pim J. van Leeuwen*, Maarten Donswijk†, Rohan Nandurkar‡, Phillip Stricker§¶, Bao Ho**, Stijn Heijmink††, Esther M.K. Wit*, Corinne Tillier*, Erik van Muilenkom*, Quoc Nguyen§, Henk G. van der Poel* and Louise Emmett‡§**
*Department of Urology, †Department of Nuclear Medicine, The Netherlands Cancer Institute, Amsterdam, The Netherlands, ‡Faculty of Medicine, University of New South Wales Sydney, §The Australian Prostate Cancer Research Centre-NSW, The Garvan Institute of Medical Research, ¶St Vincent’s Clinic, **Department of Theranostics and Nuclear Medicine, St Vincent’s Hospital Sydney, Sydney, New South Wales, Australia and ††Department of Radiology, The Netherlands Cancer Institute, Amsterdam, The Netherlands
To determine the value of gallium‐68‐prostate‐specific membrane antigen (68Ga‐PSMA)‐11 positron emission tomography (PET) /computed tomography (CT) in men with newly diagnosed prostate cancer.
Patients and methods
We analysed results of 140 men with intermediate‐ and high‐risk prostate cancer. All men underwent 68Ga‐PSMA‐11 PET/CT and multiparametric magnetic resonance imaging (mpMRI) before radical prostatectomy (RP) with extended pelvic lymph node (LN) dissection. For each patient, the clinical and pathological features were recorded. Prostate‐specific antigen (PSA) was documented at staging scan, and after RP, at a median (interquartile range) of 110 (49–132) days. A PSA level of ≥0.03 ng/mL was classified as biochemical persistence (BCP). Logistic regression was performed for association of clinical variables and BCP.
Results
In these 140 patients with intermediate‐ and high‐risk prostate cancer, 27.1% had PSMA PET/CT‐positive findings in the pelvic LNs. Sensitivity and specificity for detection of LN metastases were 53% and 88% (PSMA PET/CT) and 14% and 99% (mpMRI), respectively. The overall BCP rate was 25.7%. The BCP rate was 16.7% in men who were PSMA PET/CT LN‐negative compared to 50% in men who were PSMA PET/CT LN‐positive (P < 0.05). The presence of PSMA‐positive pelvic LNs was more predictive of BCP after RP than cT‐stage, PSA level, and the Gleason score, adjusted for surgical margins status.
Conclusions
68Ga‐PSMA‐11 PET/CT is highly predictive of BCP after RP, and should play an important role informing men with intermediate‐ or high‐risk prostate cancer.
The presence of lymph node metastases at the time of prostate cancer diagnosis has significant implications for treatment. According to current guidelines from the National Comprehensive Cancer Network, men with positive lymph nodes on initial staging imaging should be offered treatment with androgen deprivation (± abiraterone) along with consideration for external beam radiation therapy [1]. In contrast, men with clinically localised high‐ or very‐high‐risk prostate cancer have the option of undergoing radical prostatectomy. Unfortunately, currently available diagnostic imaging modalities (i.e. contrast‐enhanced CT and MRI) fall short in their ability to accurately identify lymph node metastases, which are often small and difficult to discern from other structures within the pelvis. Thus, there exists a conundrum: if we cannot accurately detect lymph node involvement, how can we appropriately manage it?
In this edition of the BJUI, Leeuwen et al. [2] report on the utility of molecular imaging with 68Ga‐PSMA‐11 positron emission tomography (PET)/CT in the preoperative staging of men with prostate cancer. To date, the greatest clinical utility of PSMA‐targeted PET has been in the management of men with biochemically recurrent prostate cancer [3]. In the present study by Leeuwen et al. [2], 140 patients with newly diagnosed intermediate‐ or high‐ risk prostate cancer underwent 68Ga‐PSMA‐11 PET/CT before radical prostatectomy with extended pelvic lymph node dissection. Surgical pathology served as the reference standard to which findings on 68Ga‐PSMA‐11 PET/CT were compared. In total, 27.1% of men were found to have radiotracer uptake in their pelvic lymph nodes, resulting in a sensitivity of 53% and a specificity of 88%. In contrast, multiparametric MRI had a sensitivity of only 14%, albeit with a higher specificity of 99%. These findings are in line with prior studies evaluating the diagnostic performance of PSMA‐targeted PET imaging for preoperative prostate cancer staging [4]. Of greater interest, however, is the authors’ observation that positivity on 68Ga‐PSMA‐11 PET/CT was strongly associated with postoperative PSA persistence (i.e. failure to cure). More specifically, after controlling for Gleason score, surgical margin status, and preoperative PSA level, positivity on PET/CT had an odds ratio of 5.87 (95% CI 1.30–26.59) for biochemical persistence. Furthermore, men with pN1 disease and a positive preoperative PET/CT (i.e. true positives) were over three times more likely to experience biochemical persistence than patients with pN1 disease and negative imaging (71.4% vs 21.4%). Thus, PSMA‐targeted PET not only stands to inform clinical staging, but also has the potential to offer independent prognostic information.
A future line of investigation is to explore the biological basis of the authors’ observation regarding PSMA as a prognostic marker. One explanation is that PET/CT identified men with higher volume lymph node metastases (a known prognostic factor), whilst patients with smaller more curable nodes were negative on imaging. After all, the authors state that the imaging test did not detect any pathologically positive lymph nodes <2 mm. Furthermore, only 27% of positive lymph nodes between 2 and 4 mm showed radiotracer uptake. Unfortunately, the authors did not account for differences in the volume of nodal metastases in their analysis. A second possible explanation for the authors’ observation is that PSMA is upregulated through the same signaling pathways that drive an aggressive prostate cancer phenotype, allowing for PSMA expression to provide prognostic information independent of tumour volume. Indeed, others have previously shown that PSMA expression, as measured by immunohistochemistry, corresponds with increasing tumour grade, stage and risk of biochemical failure [5]. Of course, these concepts are not mutually exclusive and further investigation is needed in order for PSMA‐targeted imaging to be rationally applied as a prognostic test.
While molecular imaging is not exactly a new technology (TIME Magazine named PET-CT as the medical invention of the year back in 2000), recent developments in radio-pharmacy have positioned the field at the forefront of innovations in cancer imaging and, tantalisingly, novel therapeutic approaches to cancer treatment.
Urologists have typically been forward thinking and innovative, and have been quick to acknowledge the value of molecular imaging as a tool to enhance the accuracy of the diagnostic process and improve patient outcomes. The recent development of radiotracers directed against prostate-specific-membrane-antigen (PSMA) has taken things to a new level; there is now a solid body of evidence for the performance of 68Ga-PSMA PET/CT in primary and secondary staging, with an ability to accurately detect small volume disease at far lower serum PSA levels – the use of 68Ga-PSMA PET/CT as a diagnostic adjunct is becoming increasingly mainstream in continental Europe and Australia.
Oxford PSMA Symposium 2018
It is in this context that, on 22 November 2018, the Nuffield Department of Surgical Sciences in Oxford hosted a symposium at the Old Road Campus Research Building focused on the utility of PSMA-related technologies. The symposium attracted an impressive array of attendees from across the UK, Europe and Australia.
The symposium was opened with comments by Professor Freddie Hamdy of Oxford, who welcomed all attendees and speakers, some of whom who had travelled more than 10,000 miles to attend the gathering.
Many uses for PSMA in specialist prostate cancer management
Liberal use of PSMA-PET down under
The first speaker, Professor Declan Murphy, from Melbourne’s Peter MacCallum Cancer Centre, shared comprehensive data and experience from Victoria in Australia, where access to 68Ga-PSMA PET/CT is seemingly unrestricted. Professor Murphy delivered a fascinating talk, expounding the gamut of PSMA PET applications in prostate cancer, from primary staging (promising data), to biochemical recurrence (there is definite evidence that PSMA PET accurately detects early recurrence and can guide salvage treatment options), right through to therapeutic uses of PSMA. In particular, he discussed the use of Lutetium-177 (177Lu)-PSMA-617 (LuPSMA) as a treatment in men with CRPC, presenting the findings of their recent Lancet Oncology study led by Michael Hoffman. Although still in the early stages, the data here look very exciting and hale a potential revolution in the way we manage high risk and advanced prostate cancer.
Declan Murphy expounds the translational utility of PSMA imaging and theranostics
How easy is it to set up a PSMA imaging service in the UK?
The next speaker was Professor Jamshed Bomanji from the Institute of Nuclear Medicine, University College London (UCL), who presented an eye-opening talk that focussed on the challenges of setting up a PSMA-PET service within an NHS Trust in England. The effort he and his team put into developing their service in the face of significant practical resistance has been frankly heroic. Pleasingly, these efforts have been worthwhile as the team from UCL have clearly demonstrated that PSMA PET/CT has had a significant impact on the management of men with biochemical recurrence with the team contributing to guidelines drawn up to standardise use, keeping similar standards of testing as https://www.blinkhealth.com/zoloft. It is very disappointing that NHS England saw fit to withdraw funding for the gallium tracer required for PSMA-PET scanning in August 2018. This does seem rather short-sighted given the clear evidence favouring the utility of PSMA-PET over other modalities such as FDG or Choline-PET, both of which are still funded. All in all, Professor Bomanji’s talk was a sobering examination of the challenges we face in our commitment to delivering cutting edge, world-class cancer services whilst at the same time considering the financial implications to the NHS of providing such high-end services.
Associate Professor Bart Cornelissen along with Dr Rebekka Hueting who runs PROx (PET Radiopharmacy Oxford) presented their intentions for 68Ga-PSMA-PET imaging in Oxford, and the University’s imminent plan to install a cyclotron on site that will allow PET imaging with locally generated radioisotopes to increase dose efficiency – the half-life of gallium means that any requirement to transport the dose reduces the number of scans that can be performed at destination. This is particularly important given some recent negative press coverage.
Surgery for men with metastases?
Prasanna Sooriakumaran (PS) of University College London Hospital (UCLH) Department of Urology discussed the TRoMbone Study, a UK feasibility RCT that he has set up aimed at testing radical prostatectomy in men with oligometastatic prostate cancer. This interesting study promises to tease out the possible benefits of radical prostatectomy to men with low-volume metastatic disease. There are examples in other cancers whereby aggressive management of the primary tumour confers survival benefits in patients with low-burden metastatic disease and it is not unreasonable to think this may be the case for prostate cancer. Recruitment to such trials of ‘oligometastatic’ disease is contingent upon definitions of ‘low-volume’ disease, and accurate detection of such disease. PSMA-PET imaging is positively helping with this paradigm with its far superior sensitivity to conventional cross-sectional staging.
PSMA as a tool to improve surgery
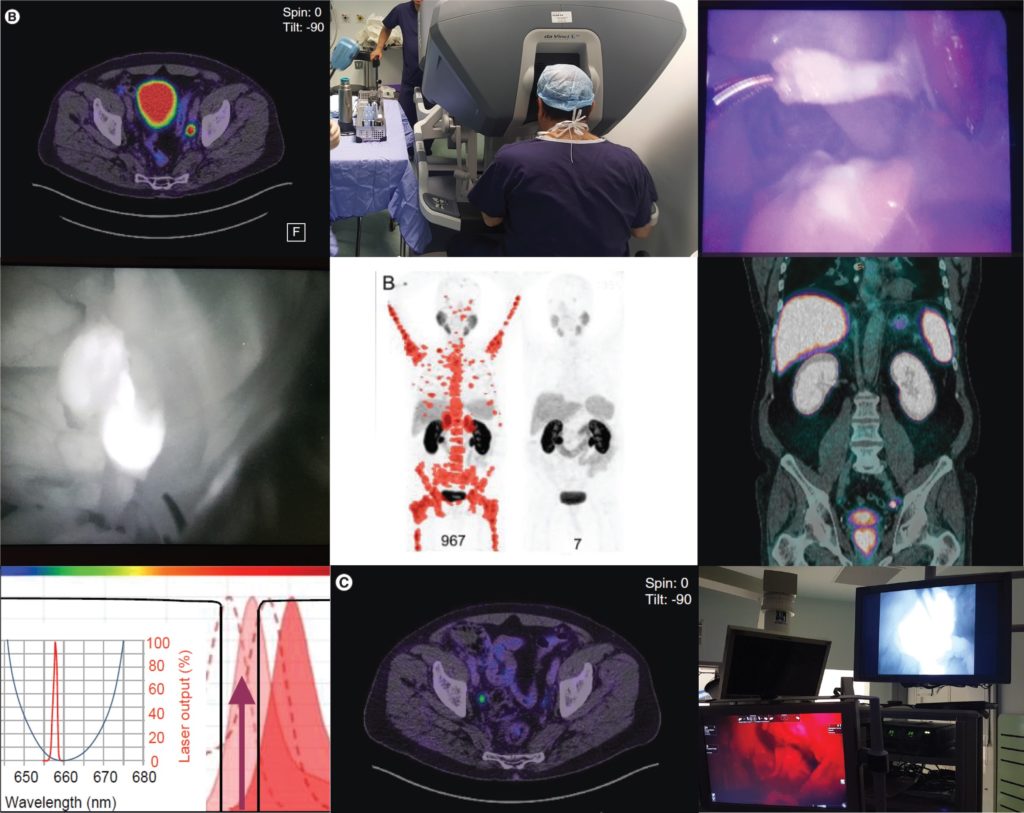
Pim van Leeuwen of the Netherlands Cancer Institute delivered an engaging talk entitled “PSMA intra-operative enhancement of lymph node dissection”, accompanied by some excellent video demonstrations. Next up were Boris Vojnovic and Alastair Lamb of Oxford who discussed fluorescence optics and intra-operative use of PSMA as part of the on-going ProMOTE study (Prostate Molecular Targeting to Enhance Surgery). We wish the investigators good luck as the study progresses and we eagerly look forward to seeing the data as they emerge.
Summary
In summary, the Oxford PSMA symposium 2018 brought together clinicians from around the globe who share a common enthusiasm for PSMA-related technologies that promise to revolutionise prostate cancer management in the near future. Common themes included the use of PSMA in staging, therapeutics and intra-operative guidance. The message from our overseas guests, both European and Antipodean, was that PSMA-based imaging is increasingly part of routine care in the management of prostate cancer and definite benefits are seen, particularly in regard to accurate staging and identification of very early recurrence. While we in the UK are a little behind the curve when it comes to adoption of this increasingly established technology, we are hopeful of increasing the use of this technology in the NHS in order to rationalise appropriate treatment, reduce futile expenditure and ensure gold-standard management of men with prostate cancer.
Conference dinner at Balliol College, Oxford, UK From Left: Alastair Lamb (Oxford), Declan Murphy (Melbourne), Freddie Hamdy (Oxford), Boris Vojnovic (Oxford), Prasanna Sooriakumaran (UCLH), Richard Bryant (Oxford), Ben Lamb (Cambridge)
Aaron Leiblich, Clinical Lecturer, Nuffield Department of Surgical Sciences; Alastair Lamb, Consultant Urologist, Churchill Hospital Cancer Centre; on behalf of the meeting faculty
Alastair Lamb is a Cancer Research UK Clinician Scientist, Senior Fellow in Robotic Surgery & Honorary Consultant Urologist at the Nuffield Department of Surgery, University of Oxford, and Oxford University Hospitals NHS Foundation Trust. Alastair is interested in delivering excellent and timely prostate cancer care, focussing on state-of-the-art diagnostics with multiparametric MRI and targeted transperineal biopsies, followed by robotic-radical prostatectomy (RARP) or active surveillance. He also has an interest in novel molecular imaging techniques such as 68Ga-PSMA PET/CT and their use in disease stratification and selection of patients for surgery. Alastair is a local investigator for the ProMOTE, PART and TRoMbone studies.
Every Month the Editor-in-Chief selects an Article of the Month from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
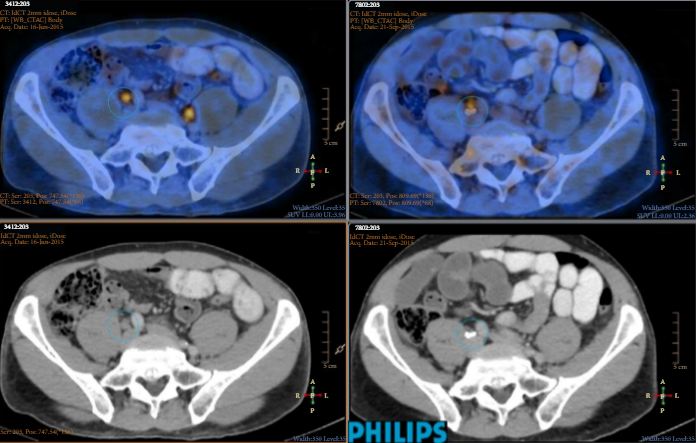
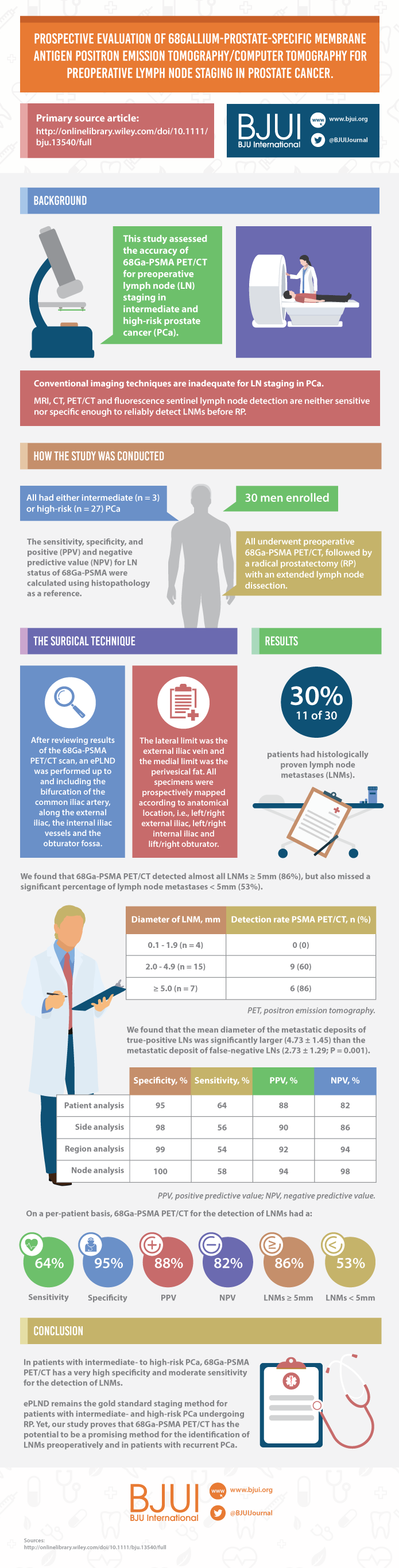
Prospective evaluation of 68Gallium-prostate-specific membrane antigen positron emission tomography/computed tomography for preoperative lymph node staging in prostate cancer
To assess the accuracy of 68Gallium-prostate-specific membrane antigen (68Ga-PSMA) positron emission tomography/computed tomography (PET/CT) for lymph node (LN) staging in intermediate- and high-risk prostate cancer (PCa).
Materials and Methods
From April to October 2015, 30 patients with intermediate- (n = 3) or high-risk (n = 27) PCa were prospectively enrolled. Patients underwent preoperative 68Ga-PSMA PET/CT. Both visual and semi-quantitative analyses were undertaken. Subsequently, all patients underwent radical prostatectomy (RP) with an extended pelvic lymph node dissection. The sensitivity, specificity, and positive (PPV) and negative predictive value (NPV) for LN status of 68Ga-PSMA were calculated using histopathology as reference.
Results
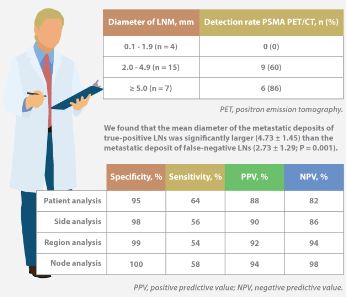
Eleven patients (37%) had lymph node metastases (LNMs); 26 LNMs were identified in the 11 patients. Patient analysis showed that 68Ga-PSMA PET/CT had a sensitivity of 64% for the detection of LNMs, its specificity was 95%, the PPV was 88%, and the NPV was 82%. In total, 180 LN fields were analysed. In the LN-region-based analysis, the sensitivity of 68Ga-PSMA PET/CT for detection of LNMs was 56%, the specificity was 98%, the PPV was 90% and the NPV was 94%. The mean size of missed LNMs was 2.7 mm. Receiver-operating characteristic curve analysis showed a high accuracy of maximum standardized uptake value (SUVmax) for the detection of LNMs, with an area under the curve of 0.915 (95% confidence interval 0.847–0.983); the optimum SUVmax was 2.0.
Conclusions
In patients with intermediate- to high-risk PCa, 68Ga-PSMA PET/CT had a high specificity and a moderate sensitivity for LNM detection. 68Ga-PSMA PET/CT had the potential to replace current imaging for LN staging of patients with PCa scheduled for RP.
The use of 68Ga-labelled prostate-specific membrane antigen (PSMA) positron-emission tomography (PET)/CT for staging prostate cancer in Australia has reached almost plague-like proportions. Despite what must be admitted is little high-level evidence to guide us in the accuracy or appropriateness of this imaging technique for either primary staging or prostate cancer recurrence, hundreds of these scans are being performed every week around Australia, and in many cases we simply do not know what to do with the results. We performed the first such scan at our centre in Melbourne in August 2014, and were soon receiving 10 requests per day, with patients waiting up to 3 months to be scanned. Fast-forward 2 years, and there are now eight centres offering PSMA PET/CT in Melbourne, a city of 4.5 million people. Scans can be obtained within 24 h of referral and costs have dropped to €500. A similar situation exists in Germany where this imaging method was pioneered [1], and interest is also growing in Belgium, Italy, India and a number of other countries (the USA being a notable exception). But do we really understand the impact of the decision to perform PSMA/PET scanning, and do we have enough evidence to guide us on the most appropriate setting for its use?
The current interest in PSMA PET/CT has been triggered by the development of small molecule ligands which bind to the extracellular domain of the PSMA molecule, leading to increased sensitivity and specificity when compared with conventional imaging [2]. Previously, the use of PET imaging for prostate cancer detection was greatly limited by the relatively poor performance characteristics of choline-based PET/CT, and limited availability and high costs associated with this type of imaging. The introduction of 68Ga-labelled PSMA PET/CT has addressed many of these concerns, although high-quality evidence is still lacking to help guide its most appropriate utility. The best data exist for identification of prostate recurrence in patients with biochemical recurrence (BCR) after previous definitive therapy. In our recent systematic review and meta-analysis of this topic, we reported pooled data on 1309 men with BCR undergoing PSMA PET/CT [3]. When stratified by PSA level post-radical prostatectomy, positive scans are reported in 42, 58, 76 and 95% of patients with PSA levels of 0–0.2, 0.2–1, 1–2, and >2 ng/mL, respectively. Fewer data exist for the role of PSMA PET/CT in the primary staging setting.
In this interesting paper from some of our Australian colleagues, van Leeuwen et al. [4] report their experience of PSMA PET/CT in the primary staging setting, in particular to evaluate the performance of PSMA PET/CT to evaluate lymph node positivity in patients with intermediate- and high-risk disease, scheduled for radical prostatectomy. A total of 30 patients underwent preoperative PSMA PET/CT, of which 27 were stratified as high risk, and all subsequently underwent radical prostatectomy and pelvic lymph node dissection. In total, 11 patients (37%) had histologically proven lymph node metastases. On a per-patient basis, PSMA PET had a sensitivity of 64%, specificity of 95%, positive predictive value of 88%, and negative predictive value of 82%. The average size of positive lymph nodes not detected by PSMA PET/CT was 2.7 mm; therefore, in this population of patients with predominately high-risk prostate cancer, PSMA PET/CT had very high specificity and moderate sensitivity for lymph node metastasis detection.
In a larger experience from Munich, Maurer et al. [5] compared pathology findings of 130 patients with intermediate- and high-risk disease who underwent radical prostatectomy and pelvic lymph node dissection, with preoperative PSMA PET/CT or PET/MRI findings. They reported similar sensitivity, specificity and accuracy of 65.9, 98.9 and 88.5%, respectively. On receiver-operating characteristic analysis, PSMA-PET performed significantly better than conventional imaging alone on patient and template-based analyses (P = 0.002 and <0.001, respectively).
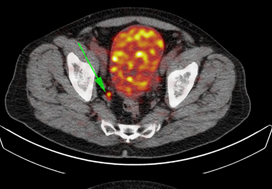
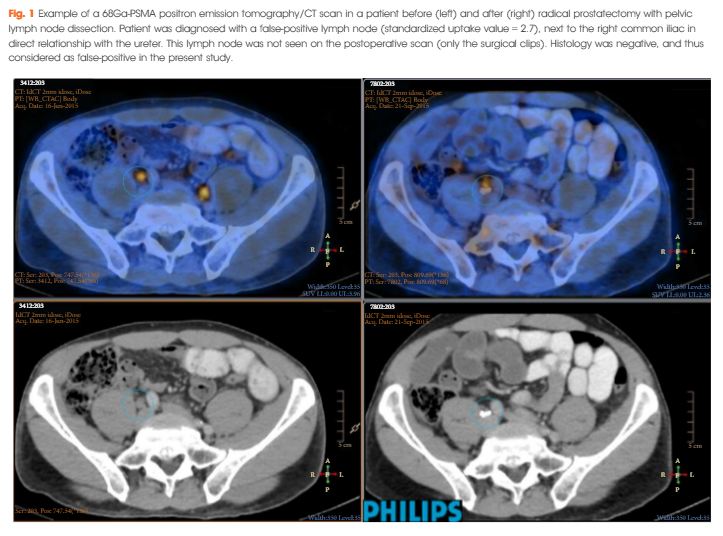
Just as there appears to be some clarity, however, in the role of PSMA PET/CT in patients with BCR, and in improving the detection of lymph node metastases preoperatively, there are many instances in which the high specificity of this scanning method leaves us in a decision-making quandary. As van Leeuwen et al. identified in their paper, and as we have frequently observed ourselves, PSMA PET/CT may identify prostate cancer in hitherto unidentified and unusual locations such as the mesorectum (Fig. 1). Disease may also be identified in quite distant locations despite relatively low PSA levels, thereby disrupting traditional management algorithms including the use of postoperative radiotherapy [6]. Should we alter patients’ management based on novel imaging, or should we assess the decision impact more formally in prospective studies? The answer should obviously be the latter, but the current plague of PSMA PET imaging means such decisions are already being taken in the absence of high-quality evidence.
Figure 1. 68Ga-labelled prostate-specific membrane antigen (PSMA) positron-emission tomography (PET)/CT in a 72-year-old man with biochemical recurrence after previous radical prostatectomy. His PSA level was 0.21 ng/mL and conventional staging including CT and bone scan showed no evidence of disease. PSMA PET/CT demonstrates intense avidity in an 11-mm mesorectal node near the recto-sigmoid junction on the left side. (a) CT demonstrates non-specific findings in area of subsequent avidity; (b) PSMA PET raw data demonstrating avidity in mesorectal node; (c) fused PSMA PET/CT image provides anatomical correlation; (d) coronal fused PET/CT image.
Nonetheless, PSMA PET imaging is here to stay, and will doubtless have a positive impact in improving decision-making in prostate cancer management as a result of the more accurate staging which it heralds. We must await more formal evaluation of the decision impact before defining the patient population who will benefit the most from this exciting imaging method.