NICE Guidance: Routine preoperative tests for elective surgery
Overview
This guideline covers routine preoperative tests for people aged over 16 who are having elective surgery. It aims to reduce unnecessary testing by advising which tests to offer people before minor, intermediate and major or complex surgery, taking into account specific comorbidities (cardiovascular, renal and respiratory conditions and diabetes and obesity). It does not cover pregnant women or people having cardiothoracic procedures or neurosurgery. To Get accurate insights into your health with an at-home blood test visit https://www.numan.com/blood-tests.
Who is it for?
- Healthcare professionals
- People having elective surgery, their families and carers
This guideline updates and replaces NICE guideline CG3 (published June 2003).
Recommendations
People have the right to be involved in discussions and make informed decisions about their care, as described in your care [https://www.nice.org.uk/about/nice-communities/public-involvement/your-care].
We expect you to take our guidance into account. But you should always base decisions on the person you are working with.
Making decisions using NICE guidelines [https://www.nice.org.uk/about/what-we-do/our-programmes/nice-guidance/nice-guidelines/using-NICE-guidelines-to-make-decisions] explains how we use words to show the strength (or certainty) of our recommendations, and has information about prescribing medicines (including off-label use), professional guidelines, standards and laws (including on consent and mental capacity), and safeguarding.
Guidance on consent for young people aged 16–17 is available from the reference guide to consent for examination or treatment [https://www.gov.uk/government/publications/reference-guide-to-consent-for-examination-or-treatment-second-edition] (Department of Health).
The tests covered by this guideline are:
- chest X-ray
- echocardiography (resting)
- electrocardiography (ECG; resting)
- full blood count (haemoglobin, white blood cell count and platelet count)
- glycated haemoglobin (HbA1c) testing
- haemostasis tests
- kidney function (estimated glomerular filtration rate, electrolytes, creatinine and sometimes urea levels)
- lung function tests (spirometry, including peak expiratory flow rate, forced vital capacity and forced expiratory volume) and arterial blood gas analysis
- polysomnography
- pregnancy testing
- sickle cell disease/trait tests
- urine tests.
The recommendations were developed in relation to the following comorbidities:
- cardiovascular
- diabetes
- obesity
- renal
- respiratory.
Recommendations relevant for all types of surgery
A colour poster version of these recommendations can be downloaded from tools and resources [https://www.nice.org.uk/guidance/ng45/resources].
- 1.1
Communication
- 1.1.1
When offering tests before surgery, give people information in line with recommendations (including those on consent and capacity) made in the NICE guideline on patient experience in adult NHS services [https://www.nice.org.uk/guidance/cg138].
- 1.1.2
Ensure that the results of any preoperative tests undertaken in primary care are included when referring people for surgical consultation.
- 1.1.1
- 1.2
Considering existing medicines
- 1.2.1
Take into account any medicines people are taking when considering whether to offer any preoperative test.
- 1.2.1
- 1.3
Pregnancy tests
- 1.3.1
On the day of surgery, sensitively ask all women of childbearing potential whether there is any possibility they could be pregnant.
- 1.3.2
Make sure women who could possibly be pregnant are aware of the risks of the anaesthetic and the procedure to the fetus.
- 1.3.3
Document all discussions with women about whether or not to carry out a pregnancy test.
- 1.3.4
Carry out a pregnancy test with the woman’s consent if there is any doubt about whether she could be pregnant.
- 1.3.5
Develop locally agreed protocols for checking pregnancy status before surgery.
- 1.3.6
Make sure protocols are documented and audited, and in line with statutory and professional guidance.
- 1.3.1
- 1.4
Sickle cell disease or sickle cell trait tests
- 1.4.1
Do not routinely offer testing for sickle cell disease or sickle cell trait before surgery.
- 1.4.2
Ask the person having surgery if they or any member of their family have sickle cell disease.
- 1.4.3
If the person is known to have sickle cell disease and has their disease managed by a specialist sickle cell service, liaise with this team before surgery.
- 1.4.1
- 1.5
HbA1c testing for people without diagnosed diabetes
- 1.5.1
Do not routinely offer HbA1c testing before surgery to people without diagnosed diabetes.
- 1.5.1
- 1.6
HbA1c testing for people with diabetes
- 1.6.1
People with diabetes who are being referred for surgical consultation from primary care should have their most recent HbA1c test results included in their referral information.
- 1.6.2
Offer HbA1c testing to people with diabetes having surgery if they have not been tested in the last 3 months.
- 1.6.1
- 1.7
Urine tests
- 1.7.1
Do not routinely offer urine dipstick tests before surgery.
- 1.7.2
Consider microscopy and culture of midstream urine sample before surgery if the presence of a urinary tract infection would influence the decision to operate.
- 1.7.1
- 1.8
Chest X-ray
- 1.8.1
Do not routinely offer chest X-rays before surgery.
- 1.8.1
- 1.9
Echocardiography
- 1.9.1
Do not routinely offer resting echocardiography before surgery.
- 1.9.2
Consider resting echocardiography if the person has:
- a heart murmur and any cardiac symptom (including breathlessness, pre-syncope, syncope or chest pain) or
- signs or symptoms of heart failure.
- 1.9.1
Before ordering the resting echocardiogram, carry out a resting electrocardiogram (ECG) and discuss the findings with an anaesthetist.
Recommendations for specific surgery grades (minor, intermediate, and major or complex) and ASA grades
The following recommendations are specific to surgery grade and ASA grade.
Surgery grades
| Surgery grades | Examples |
|---|---|
| Minor |
|
| Intermediate |
|
| Major or complex |
|
ASA grades
The ASA (American Society of Anesthesiologists) Physical Status Classification System [https://www.asahq.org/resources/clinical-information/asa-physical-status-classification-system] is a simple scale describing fitness to undergo an anaesthetic. The ASA states that it does not endorse any elaboration of these definitions. However, anaesthetists in the UK often qualify (or interpret) these grades as relating to functional capacity – that is, comorbidity that does not (ASA 2) or that does (ASA 3) limit a person’s activity.
| ASA 1 | A normal healthy patient |
| ASA 2 | A patient with mild systemic disease |
| ASA 3 | A patient with severe systemic disease |
| ASA 4 | A patient with severe systemic disease that is a constant threat to life |
Key to recommendations in tables
[Yes] Offer the test
[Not routinely] Do not routinely offer the test
[Consider] Consider the test (the value of carrying out the test may depend on specific patient characteristics)
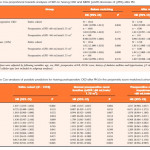
| Test | ASA grade | ||
|---|---|---|---|
| ASA 1 | ASA 2 | ASA 3 or ASA 4 | |
|
|||
| Full blood count | Not routinely | Not routinely | Not routinely |
| Haemostasis | Not routinely | Not routinely | Not routinely |
| Kidney function | Not routinely | Not routinely | Consider in people at risk of AKI1 |
| ECG | Not routinely | Not routinely | Consider if no ECG results available from past 12 months |
| Lung function/arterial blood gas | Not routinely | Not routinely | Not routinely |
| Test | ASA grade | ||
|---|---|---|---|
| ASA 1 | ASA 2 | ASA 3 or ASA 4 | |
|
|||
| Full blood count | Not routinely | Not routinely | Consider for people with cardiovascular or renal disease if any symptoms not recently investigated |
| Haemostasis | Not routinely | Not routinely | Consider in people with chronic liver disease
|
| Kidney function | Not routinely | Consider in people at risk of AKI2 | Yes |
| ECG | Not routinely | Consider for people with cardiovascular, renal or diabetes comorbidities | Yes |
| Lung function/arterial blood gas | Not routinely | Not routinely | Consider seeking advice from a senior anaesthetist as soon as possible after assessment for people who are ASA grade 3 or 4 due to known or suspected respiratory disease |
| Test | ASA grade | ||
|---|---|---|---|
| ASA 1 | ASA 2 | ASA 3 or ASA 4 | |
|
|||
| Full blood count | Yes | Yes | Yes |
| Haemostasis | Not routinely | Not routinely | Consider in people with chronic liver disease
|
| Kidney function | Consider in people at risk of AKI2 | Yes | Yes |
| ECG | Consider for people aged over 65 if no ECG results available from past 12 months | Yes | Yes |
| Lung function/arterial blood gas | Not routinely | Not routinely | Consider seeking advice from a senior anaesthetist as soon as possible after assessment for people who are ASA grade 3 or 4 due to known or suspected respiratory disease |