TRC105 is a chimeric immunoglobulin G1 monoclonal antibody that binds endoglin (CD105). This phase I open-label study evaluated the safety, pharmacokinetics and pharmacodynamics of TRC105 in patients with metastatic castration-resistant prostate cancer (mCRPC).
PATIENTS AND METHODS
Patients with mCRPC received escalating doses of i.v. TRC105 until unacceptable toxicity or disease progression, up to a predetermined dose level, using a standard 3 + 3 phase I design.
RESULTS
A total of 20 patients were treated. The top dose level studied, 20 mg/kg every 2 weeks, was the maximum tolerated dose. Common adverse effects included infusion-related reaction (90%), low grade headache (67%), anaemia (48%), epistaxis (43%) and fever (43%). Ten patients had stable disease on study and eight patients had declines in prostate specific antigen (PSA). Significant plasma CD105 reduction was observed at the higher dose levels. In an exploratory analysis, vascular endothelial growth factor (VEGF) was increased after treatment with TRC105 and VEGF levels were associated with CD105 reduction.
CONCLUSION
TRC105 was tolerated at 20 mg/kg every other week with a safety profile distinct from that of VEGF inhibitors. A significant induction of plasma VEGF was associated with CD105 reduction, suggesting anti-angiogenic activity of TRC105. An exploratory analysis showed a tentative correlation between the reduction of CD105 and a decrease in PSA velocity, suggestive of potential activity of TRC105 in the patients with mCRPC. The data from this exploratory analysis suggest that rising VEGF level is a possible compensatory mechanism for TRC105-induced anti-angiogenic activity.
To improve awareness and recognition of chronic bacterial prostatitis (CBP) and chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) among non-specialists and patients. To provide guidance to healthcare professionals treating patients with CBP and CP/CPPS, in both non-specialist and specialist settings. To promote efficient referral of care between non-specialists and specialists and the involvement of the multidisciplinary team (MDT).
PATIENTS AND METHODS
The guideline population were men with CBP or CP/CPPS (persistent or recurrent symptoms and no other urogenital pathology for ≥3 of the previous 6 months). Consensus recommendations for the guidelines were based on a search to identify literature on the diagnosis and management of CBP and CP/CPPS (published between 1999 and February 2014). A Delphi panel process was used where high-quality, published evidence was lacking.
RESULTS
CBP and CP/CPPS can present with a wide range of clinical manifestations. The four main symptom domains are urogenital pain, lower urinary tract symptoms (LUTS – voiding or storage symptoms), psychological issues and sexual dysfunction. Patients should be managed according to their individual symptom pattern. Options for first-line treatment include antibiotics, α-adrenergic antagonists (if voiding LUTS are present) and simple analgesics. Repeated use of antibiotics, such as quinolones, should be avoided if there is no obvious symptomatic benefit from infection control or cultures do not support an infectious cause. Early use of treatments targeting neuropathic pain and/or referral to specialist services should be considered for patients who do not respond to initial measures. An MDT approach (urologists, pain specialists, nurse specialists, specialist physiotherapists, general practitioners, cognitive behavioural therapists/psychologists, and sexual health specialists) is recommended. Patients should be fully informed about the possible underlying causes and treatment options, including an explanation of the chronic pain cycle.
CONCLUSION
Chronic prostatitis can present with a wide variety of signs and symptoms. Identification of individual symptom patterns and a symptom-based treatment approach are recommended. Further research is required to evaluate management options for CBP and CP/CPPS.
Safety and efficacy of mirabegron as add-on therapy in patients with overactive bladder treated with solifenacin: a postmarketing, open-label study in Japan (MILAI study)
OsamuYamaguchi,HidehiroKakizaki*,YukioHomma†,YasuhikoIgawa‡,Masayuki Takeda§,OsamuNishizawa¶,MomokazuGotoh**,MasakiYoshida††,Osamu Yokoyama‡‡,NarihitoSeki§§,AkiraOkitsu¶¶,TakuyaHamada¶¶,AkikoKobayashi¶¶ and KentarouKuroishi¶¶
To examine the safety and efficacy of mirabegron as ‘add-on’ therapy to solifenacin in patients with overactive bladder (OAB).
PATIENTS AND METHODS
This multicentre, open-label, phase IV study enrolled patients aged ≥20 years with OAB, as determined by an OAB symptom score (OABSS) total of ≥3 points and an OABSS Question 3 score of ≥2 points, who were being treated with solifenacin at a stable dose of 2.5 or 5 mg once daily for at least 4 weeks. Study duration was 18 weeks, comprising a 2-week screening period and a 16-week treatment period. Patients meeting eligibility criteria continued to receive solifenacin (2.5 or 5 mg once daily) and additional mirabegron (25 mg once daily) for 16 weeks. After 8 weeks of treatment, the mirabegron dose could be increased to 50 mg if the patient’s symptom improvement was not sufficient, if he/she was agreeable to the dose increase, and the investigator judged that there were no safety concerns. Safety assessments included adverse events (AEs), laboratory tests, vital signs, 12-lead electrocardiogram, QT corrected for heart rate using Fridericia’s correction (QTcF) interval and post-void residual (PVR) volume. Efficacy endpoints were changes from baseline in OABSS total score, OAB questionnaire short form (OAB-q SF) score (symptom bother and total health-related quality of life [HRQL] score), mean number of micturitions/24 h, mean number of urgency episodes/24 h, mean number of urinary incontinence (UI) episodes/24 h, mean number of urgency UI episodes/24 h, mean volume voided/micturition, and mean number of nocturia episodes/night. Patients were instructed to complete the OABSS sheets at weeks −2, 0, 8 and 16 (or at discontinuation), OAB-q SF sheets at weeks 0, 8 and 16 (or at discontinuation) and patient voiding diaries at weeks 0, 4, 8, 12 and 16 (or at discontinuation).
RESULTS
Overall incidence of drug-related treatment-emergent AEs (TEAEs) was 23.3%. Almost all TEAEs were mild or moderate. The most common TEAE was constipation, with similar incidence in the groups receiving a dose increase to that observed in the groups maintained on the original dose. Changes in PVR volume, QTcF interval, pulse rate and blood pressure were not considered to be clinically significant and there were no reports of urinary retention. Significant improvement was seen for changes in efficacy endpoints from baseline to end of treatment (EOT) in all groups (patients receiving solifenacin 2.5 or 5 mg + mirabegron 25 or 50 mg).
CONCLUSIONS
Add-on therapy with mirabegron 25 mg once daily for 16 weeks, with an optional dose increase to 50 mg at week 8, was well tolerated in patients with OAB treated with solifenacin 2.5 mg or 5 mg once daily. There were significant improvements from baseline to EOT in OAB symptoms with combination therapy with mirabegron and solifenacin. Add-on therapy with mirabegron and an antimuscarinic agent, such as solifenacin, may provide an attractive therapeutic option.
Trifecta and Optimal Peri-operative outcomes of Robotic and Laparoscopic Partial Nephrectomy In Surgical Treatment Of Small Renal Masses: A Multi-Institutional Study
HomayounZargar*,MohamadE.Allaf†,SamBhayani‡,MichaelStifelman§, CraigRogers¶,MarkW.Ball†,JeffreyLarson‡,SusanMarshall§,RameshKumar¶ and JihadH.Kaouk*
To compare the perioperative outcomes of robotic partial nephrectomy (RPN) with laparoscopic PN (LPN) performed for small renal masses (SRMs), in a large multi-institutional series and to define a new composite outcome measure, termed ‘optimal outcome’ for the RPN group.
PATIENTS AND METHODS
Retrospective review of 2392 consecutive cases of RPN and LPN performed in five high-volume centres from 2004 to mid-2013. We limited our study to SRMs and cases performed by surgeons with significant expertise with the technique. The Trifecta was defined as negative surgical margin, zero perioperative complications and a warm ischaemia time of ≤25 min. The ‘optimal outcome’ was defined as achievement of Trifecta with addition of 90% estimated glomerular filtration rate preservation and no chronic kidney disease stage upgrading. Univariable and multivariable analysis were used to identify factors predicting Trifecta and ‘optimal outcome’ achievement.
RESULTS
In all, 1185 RPN and 646 LPN met our inclusion criteria. Patients in the RPN group were older and had a higher median Charlson comorbidity index and higher R.E.N.A.L. nephrometry score. The RPN group had lower warm ischaemia time (18 vs 26 min), overall complication rate (16.2% vs 25.9%), and positive surgical margin rate (3.2% vs. 9.7%). There was a significantly higher Trifecta rate for RPN (70% vs 33%) and the rate of achievement of ‘optimal outcome’ for the RPN group was 38.5%.
CONCLUSIONS
In this large multi-institutional series RPN was superior to LPN for perioperative surgical outcomes measured by Trifecta. Patients in the RPN group had better outcomes for all three components of Trifecta compared with their LPN counterparts. Our more strict definition for ‘optimal outcome’ might be a better tool for assessing perioperative and functional outcomes after minimally invasive PN. This tool needs to be externally validated.
To investigate by electromyography (EMG), the presence of complex repetitive discharges (CRDs) and decelerating bursts (DBs) in the striated external urethral sphincter during the menstrual cycle in female volunteers with no urinary symptoms and complete bladder emptying.
SUBJECTS AND METHODS
Healthy female volunteers aged 20–40 years, with regular menstrual cycles and no urinary symptoms were recruited. Volunteers completed a menstruation chart, urinary symptom questionnaires, pregnancy test, urine dipstick, urinary free flow and post-void ultrasound bladder scan. Exclusion criteria included current pregnancy, use of hormonal medication or contraception, body mass index of >35 kg/m2, incomplete voiding and a history of pelvic surgery. Eligible participants underwent an external urethral sphincter EMG, using a needle electrode in the early follicular phase and the mid-luteal phase of their menstrual cycles. Serum oestradiol and progesterone were measured at each EMG test.
RESULTS
In all, 119 women enquired about the research and following screening, 18 were eligible to enter the study phase. Complete results were obtained in 15 women. In all, 30 EMG tests were undertaken in the 15 asymptomatic women. Sphincter EMG was positive for CRDs and DBs at one or both phases of the menstrual cycle in eight (53%) of the women. Three had CRDs and DBs in both early follicular and mid-luteal phases. Five had normal EMG activity in the early follicular phase and CRDs and DBs in the mid-luteal phase. No woman had abnormal EMG activity in the early follicular phase and normal activity in the luteal phase. There was no relationship between EMG activity and age, parity or serum levels of oestradiol and progesterone.
CONCLUSIONS
CRDs and DB activity in the external striated urethral sphincter is present in a high proportion of asymptomatic young women. This abnormal EMG activity has been shown for the first time to change during the menstrual cycle in individual women. CRDs and DBs are more commonly found in the luteal phase of the menstrual cycle. The importance of CRDs and DBs in the aetiology of urinary retention in young women remains uncertain. The distribution and or quantity of abnormal EMG activity in the external urethral sphincter may be important. In a woman with urinary retention the finding of CRDs and DBs by needle EMG does not automatically establish Fowler’s syndrome as the explanation for the bladder dysfunction. Urethral pressure profilometry may be helpful in establishing a diagnosis. Opiate use and psychological stress should be considered in young women with urinary retention.
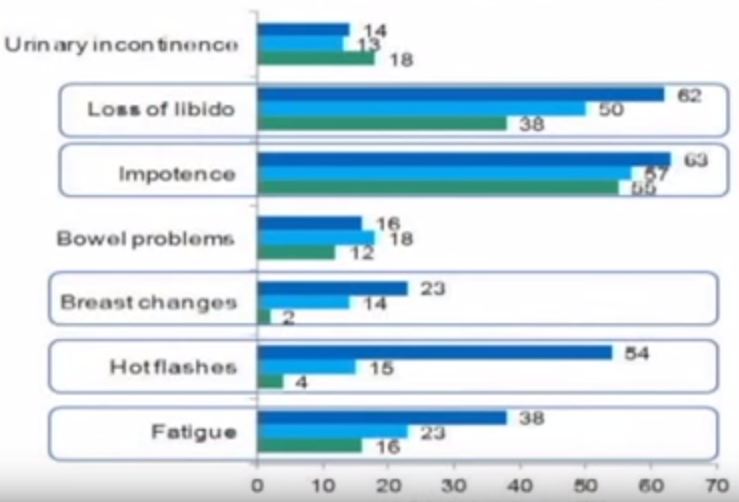
Patient reported “ever had” and “current” long term physical symptoms following prostate cancer treatments.
To investigate the prevalence of physical symptoms that were ‘ever’ and ‘currently’ experienced by survivors of prostate cancer at a population level, to assess burden and thus inform policy to support survivors. The study included 3 348 men surviving prostate cancer for 2-18 years after diagnosis. A cross-sectional, postal survey of 6 559 survivors diagnosed 2-18 years ago with primary, invasive prostate cancer (ICD10-C61) identified via national, population-based cancer registries in Northern Ireland and Republic of Ireland. Questions included symptoms at diagnosis, primary treatments and physical symptoms (erectile dysfunction [ED]/urinary incontinence [UI]/bowel problems/breast changes/loss of libido/hot flashes/fatigue) experienced ‘ever’ and at questionnaire completion (‘current’). Symptom proportions were weighted by age, country and time since diagnosis. Bonferroni corrections were applied for multiple comparisons.
Adjusted response rate 54%; 75% reported at least one ‘current’ physical symptom (‘ever’ 90%), with 29% reporting at least three. Prevalence varied by the diverse treatments found at https://www.ukmeds.co.uk/finasteride. Overall, 57% reported current ED and this was highest after radical prostatectomy (RP, 76%) followed by external beam radiotherapy with concurrent hormone therapy (HT, 64%). UI (overall ‘current’ 16%) was highest after RP (‘current’ 28%; ‘ever’ 70%). While 42% of brachytherapy patients reported no ‘current’ symptoms, 43% reported ‘current’ ED and 8% ‘current’ UI. ‘Current’ hot flashes (41%), breast changes (18%) and fatigue (28%) were reported more often by patients on HT.
Anna T. Gavin, Frances J. Drummond*, Conan Donnelly, Eamonn O’Leary*, Linda Sharp† and Heather R. Kinnear
Northern Ireland Cancer Registry, Centre for Public Health, Queen’s University Belfast, Mulhouse Building, Belfast Northern Ireland, UK, *National Cancer Registry Ireland, Building 6800, Airport Business Park Cork, Ireland, and †Institute of Health and Society, Newcastle University, Richardson Road, Newcastle upon Tyne, NE2 4AX, England, UK
To investigate the prevalence of physical symptoms that were ‘ever’ and ‘currently’ experienced by survivors of prostate cancer at a population level, to assess burden and thus inform policy to support survivors.
PATIENTS AND METHODS
The study included 3 348 men surviving prostate cancer for 2–18 years after diagnosis. A cross-sectional, postal survey of 6 559 survivors diagnosed 2–18 years ago with primary, invasive prostate cancer (ICD10-C61) identified via national, population-based cancer registries in Northern Ireland and Republic of Ireland. Questions included symptoms at diagnosis, primary treatments and physical symptoms (erectile dysfunction [ED]/urinary incontinence [UI]/bowel problems/breast changes/loss of libido/hot flashes/fatigue) experienced ‘ever’ and at questionnaire completion (‘current’). Symptom proportions were weighted by age, country and time since diagnosis. Bonferroni corrections were applied for multiple comparisons.
RESULTS
Adjusted response rate 54%; 75% reported at least one ‘current’ physical symptom (‘ever’ 90%), with 29% reporting at least three. Prevalence varied by treatment. Overall, 57% reported current ED and this was highest after radical prostatectomy (RP, 76%) followed by external beam radiotherapy with concurrent hormone therapy (HT, 64%). UI (overall ‘current’ 16%) was highest after RP (‘current’ 28%; ‘ever’ 70%). While 42% of brachytherapy patients reported no ‘current’ symptoms, 43% reported ‘current’ ED and 8% ‘current’ UI. ‘Current’ hot flashes (41%), breast changes (18%) and fatigue (28%) were reported more often by patients on HT.
CONCLUSION
Symptoms after prostate cancer treatment are common, often multiple, persist long-term and vary by treatment method. They represent a significant health burden. An estimated 1.6% of men aged >45 years are survivors of prostate cancer and currently experiencing an adverse physical symptom. Recognition and treatment of physical symptoms should be prioritised in patient follow-up. This information should facilitate men and clinicians when deciding about treatment as differences in survival between radical treatments is minimal.
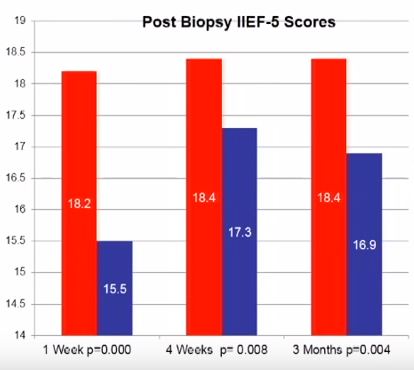
To prospectively evaluate the effect of transrectal ultrasonography (TRUS)-guided prostate biopsy on erectile and voiding function at multiple time-points after biopsy.
PATIENTS AND METHODS
All men who underwent TRUS-guided prostate biopsy completed a five-item version of the International Index of Erectile Function (IIEF-5) and the International Prostate Symptom Score (IPSS) before and at 1, 4 and 12 weeks after TRUS-guided biopsy. Statistical analyses used were a general descriptive analysis, continuous variables using a t-test and categorical data using chi-square analysis. A paired t-test was used to compare each patient’s baseline score to their own follow-up survey scores.
RESULTS
In all, 220 patients were enrolled with a mean age of 64.1 years and PSA level of 6.7 ng/dL. At initial presentation, 38.6% reported no erectile dysfunction (ED), 22.3% mild ED, 15.5% mild-to-moderate ED, 10% moderate ED, and 13.6% severe ED. On paired t-test there was a statistically significant reduction in IIEF-5 score at 1 week after biopsy compared with before biopsy (18.2 vs 15.5; P < 0.001). This remained significantly reduced at 4 (18.4 vs 17.3; P = 0.008) and 12 weeks (18.4 vs 16.9, P = 0.004) after biopsy.
CONCLUSIONS
The effects of TRUS-guided prostate biopsy on erectile function have probably been underestimated. It is important to be aware of these transient effects so patients can be appropriately counselled. The exact cause of this effect is yet to be determined.
To evaluate the impact of components of metabolic syndrome (MetS) on urinary outcomes after surgery for severe lower urinary tract symptoms (LUTS) due to benign prostatic enlargement (BPE), as central obesity can be associated with the development of BPE and with the worsening of LUTS.
PATIENTS AND METHODS
A multicentre prospective study was conducted including 378 consecutive men surgically treated for large BPE with simple open prostatectomy (OP) or transurethral resection of the prostate (TURP), between January 2012 and October 2013. LUTS were measured by the International Prostate Symptom Score (IPSS), immediately before surgery and at 6–12 months postoperatively. MetS was defined according the USA National Cholesterol Education Program-Adult Treatment Panel III.
RESULTS
The improvement of total and storage IPSS postoperatively was related to diastolic blood pressure and waist circumference (WC). A WC of >102 cm was associated with a higher risk of an incomplete recovery of both total IPSS (odds ratio [OR] 0.343, P = 0.001) and storage IPSS (OR 0.208, P < 0.001), as compared with a WC of <102 cm. The main limitations were: (i) population selected from a tertiary centre, (ii) Use exclusively of IPSS questionnaire, and (iii) No inclusion of further data.
CONCLUSIONS
Increased WC is associated with persistent postoperative urinary symptoms after surgical treatment of BPE. Obese men have a higher risk of persistent storage LUTS after TURP or OP.
To assess the potential complications associated with inguinal lymph node dissection (ILND) across international tertiary care referral centres, and to determine the prognostic factors that best predict the development of these complications.
MATERIALS AND METHODS
A retrospective chart review was conducted across four international cancer centres. The study population of 327 patients underwent diagnostic/therapeutic ILND. The endpoint was the overall incidence of complications and their respective severity (major/minor). The Clavien–Dindo classification system was used to standardize the reporting of complications.
RESULTS
A total of 181 patients (55.4%) had a postoperative complication, with minor complications in 119 cases (65.7%) and major in 62 (34.3%). The total number of lymph nodes removed was an independent predictor of experiencing any complication, while the median number of lymph nodes removed was an independent predictor of major complications. The American Joint Committee on Cancer stage was an independent predictor of all wound infections, while the patient’s age, ILND with Sartorius flap transposition, and surgery performed before the year 2008 were independent predictors of major wound infections.
CONCLUSIONS
This is the largest report of complication rates after ILND for squamous cell carcinoma of the penis and it shows that the majority of complications associated with ILND are minor and resolve without prolonged morbidity. Variables pertaining to the extent of disease burden have been found to be prognostic of increased postoperative morbidity.
To evaluate the face, content and construct validity of the distributed simulation (DS) environment for technical and non-technical skills training in endourology. To evaluate the educational impact of DS for urology training.
SUBJECTS AND METHODS
DS offers a portable, low-cost simulated operating room environment that can be set up in any open space. A prospective mixed methods design using established validation methodology was conducted in this simulated environment with 10 experienced and 10 trainee urologists. All participants performed a simulated prostate resection in the DS environment. Outcome measures included surveys to evaluate the DS, as well as comparative analyses of experienced and trainee urologist’s performance using real-time and ‘blinded’ video analysis and validated performance metrics. Non-parametric statistical methods were used to compare differences between groups.
RESULTS
The DS environment demonstrated face, content and construct validity for both non-technical and technical skills. Kirkpatrick level 1 evidence for the educational impact of the DS environment was shown. Further studies are needed to evaluate the effect of simulated operating room training on real operating room performance.
CONCLUSIONS
This study has shown the validity of the DS environment for non-technical, as well as technical skills training. DS-based simulation appears to be a valuable addition to traditional classroom-based simulation training.