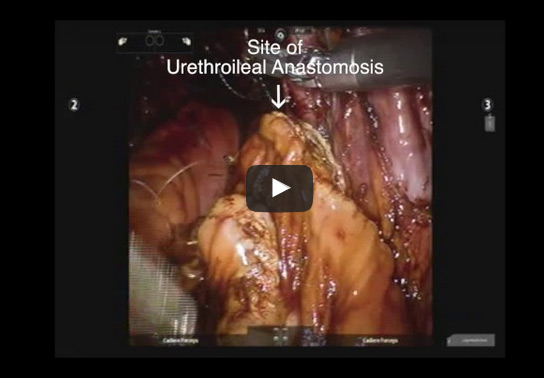
To describe our, step-by-step, technique for robotic intracorporeal neobladder formation.
Patients and Methods
The main surgical steps to forming the intracorporeal orthotopic ileal neobladder are: isolation of 65 cm of small bowel; small bowel anastomosis; bowel detubularisation; suture of the posterior wall of the neobladder; neobladder–urethral anastomosis and cross folding of the pouch; and uretero-enteral anastomosis. Improvements have been made to these steps to enhance time efficiency without compromising neobladder configuration.
Results
Our technical improvements have resulted in an improvement in operative time from 450 to 360 min.
Conclusion
We describe an updated step-by-step technique of robot-assisted intracorporeal orthotopic ileal neobladder formation.
To validate vascular endothelial growth factor receptor-1 (VEGFR1) single nucleotide polymorphism (SNP) rs9582036 as a potential predictive biomarker in metastatic clear-cell renal cell carcinoma (m-ccRCC) patients treated with sunitinib.
Materials and Methods
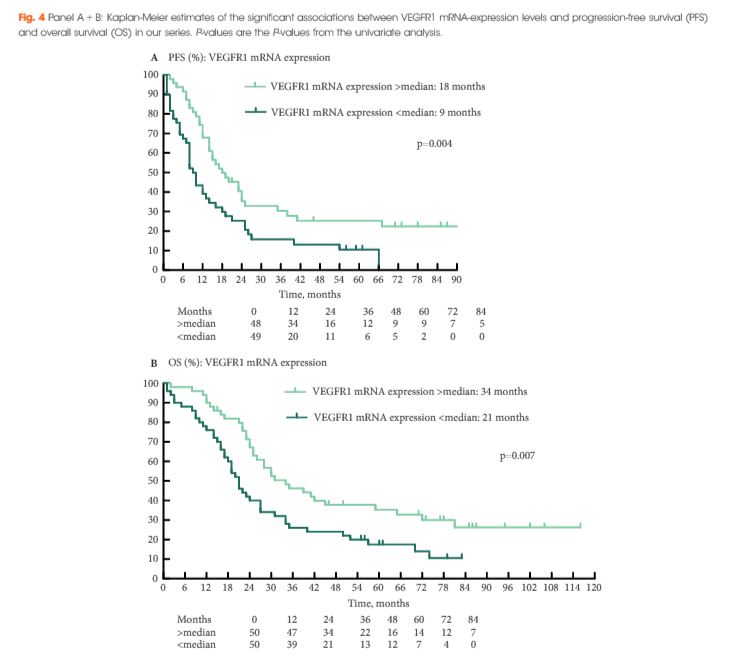
m-ccRCC patients receiving sunitinib as first-line targeted therapy were included. We assessed response rate (RR), progression-free survival (PFS), overall survival (OS), and clinical and biochemical parameters associated with outcome. We genotyped five VEGFR1 SNPs: rs9582036, rs7993418, rs9554320, rs9554316 and rs9513070. Association with outcome was studied by univariate analysis and by multivariate Cox regression. Additionally, we updated survival data of our discovery cohort as described previously.
Results
Sixty-nine patients were included in the validation cohort. rs9582036 CC-carriers had a poorer PFS (8 vs 12 months, P = 0.02) and OS (11 vs 27 months, P = 0.003) compared to AC/AA-carriers. rs7993418 CC-carriers had a poorer OS (8 vs 24 months, P = 0.004) compared to TC/TT-carriers. rs9554320 AA-carriers had a poorer RR (0% vs 53%, P = 0.009), PFS (5 vs 12 months, P = 0.003) and OS (10 vs 25 months, P = 0.004) compared to AC/CC-carriers. When pooling patients from the discovery cohort, as described previously (n = 88), and the validation cohort, in the total series of 157 patients, rs9582036 CC-carriers had a poorer RR (8% vs 49%, P = 0.004), PFS (8 vs 14 months, P = 0.003) and OS (13 vs 30 months, P = 0.0004) compared to AC/AA-carriers. Unfavorable prognostic markers at start of sunitinib were well balanced between rs9582036 CC- and AC/AA-carriers.
Conclusion
VEGFR1 rs9582036 is a candidate predictive biomarker in m-ccRCC-patients treated with sunitinib.
Patient-reported outcomes in the ProtecT randomized trial of clinically localized prostate cancer treatments: study design, and baseline urinary, bowel and sexual function and quality of life
To present the baseline patient-reported outcome measures (PROMs) in the Prostate Testing for Cancer and Treatment (ProtecT) randomized trial comparing active monitoring, radical prostatectomy and external-beam conformal radiotherapy for localized prostate cancer and to compare results with other populations.
Materials and Methods
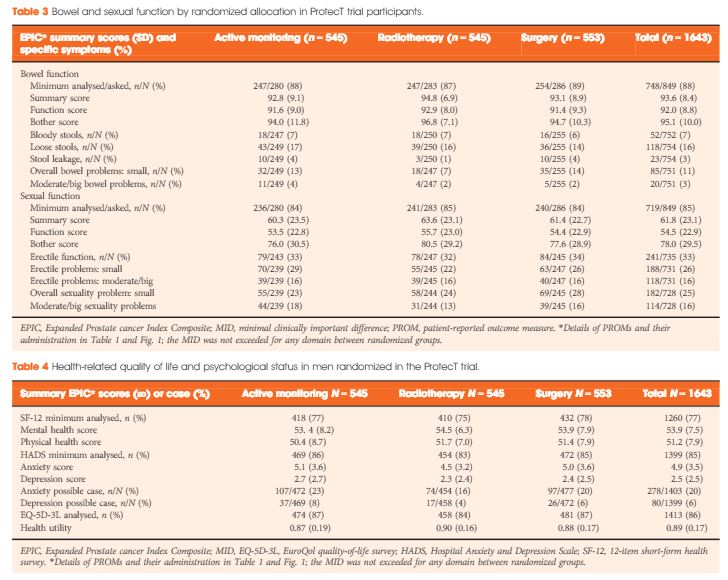
A total of 1643 randomized men, aged 50–69 years and diagnosed with clinically localized disease identified by prostate-specific antigen (PSA) testing, in nine UK cities in the period 1999–2009 were included. Validated PROMs for disease-specific (urinary, bowel and sexual function) and condition-specific impact on quality of life (Expanded Prostate Index Composite [EPIC], 2005 onwards; International Consultation on Incontinence Questionnaire-Urinary Incontinence [ICIQ-UI], 2001 onwards; the International Continence Society short-form male survey [ICSmaleSF]; anxiety and depression (Hospital Anxiety and Depression Scale [HADS]), generic mental and physical health (12-item short-form health survey [SF-12]; EuroQol quality-of-life survey, the EQ-5D-3L) were assessed at prostate biopsy clinics before randomization. Descriptive statistics are presented by treatment allocation and by men’s age at biopsy and PSA testing time points for selected measures.
Results
A total of 1438 participants completed biopsy questionnaires (88%) and 77–88% of these were analysed for individual PROMs. Fewer than 1% of participants were using pads daily (5/754). Storage lower urinary tract symptoms were frequent (e.g. nocturia 22%, 312/1423). Bowel symptoms were rare, except for loose stools (16%, 118/754). One third of participants reported erectile dysfunction (241/735) and for 16% (118/731) this was a moderate or large problem. Depression was infrequent (80/1399, 6%) but 20% of participants (278/1403) reported anxiety. Sexual function and bother were markedly worse in older men (65–70 years), whilst urinary bother and physical health were somewhat worse than in younger men (49–54 years, all P < 0.001). Bowel health, urinary function and depression were unaltered by age, whilst mental health and anxiety were better in older men (P < 0.001). Only minor differences existed in mental or physical health, anxiety and depression between PSA testing and biopsy assessments.
Conclusion
The ProtecT trial baseline PROMs response rates were high. Symptom frequencies and generic quality of life were similar to those observed in populations screened for prostate cancer and control subjects without cancer.
To evaluate the effect of smoking on sperm functional quality and seminal plasma proteomic profile.
Patients and Methods
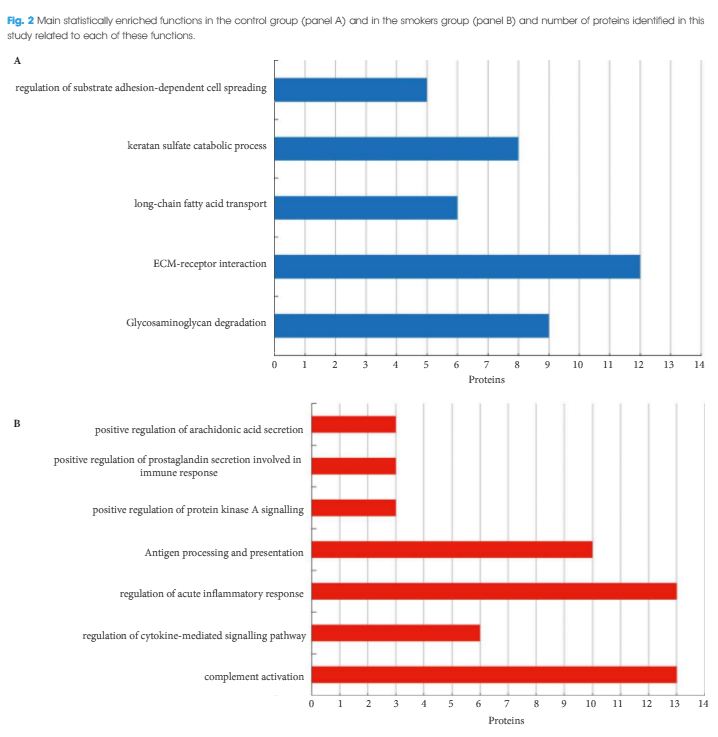
Sperm functional tests were performed in 20 non-smoking men with normal semen quality, according to the World Health Organization (2010) and in 20 smoking patients. These included: evaluation of DNA fragmentation by alkaline Comet assay; analysis of mitochondrial activity using DAB staining; and acrosomal integrity evaluation by PNA binding. The remaining semen was centrifuged and seminal plasma was used for proteomic analysis (liquid chromatography-tandem mass spectrometry). The quantified proteins were used for Venn diagram construction in Cytoscape 3.2.1 software, using the PINA4MS plug-in. Then, differentially expressed proteins were used for functional enrichment analysis of Gene Ontology categories, Kyoto Encyclopedia of Genes and Genomes and Reactome, using Cytoscape software and the ClueGO 2.2.0 plug-in.
Results
Smokers had a higher percentage of sperm DNA damage (Comet classes III and IV; P < 0.01), partially and fully inactive mitochondria (DAB classes III and IV; P = 0.001 and P = 0.006, respectively) and non-intact acrosomes (P < 0.01) when compared with the control group. With respect to proteomic analysis, 422 proteins were identified and quantified, of which one protein was absent, 27 proteins were under-represented and six proteins were over-represented in smokers. Functional enrichment analysis showed the enrichment of antigen processing and presentation, positive regulation of prostaglandin secretion involved in immune response, protein kinase A signalling and arachidonic acid secretion, complement activation, regulation of the cytokine-mediated signalling pathway and regulation of acute inflammatory response in the study group (smokers).
Conclusion
In conclusion, cigarette smoking was associated with an inflammatory state in the accessory glands and in the testis, as shown by enriched proteomic pathways. This state causes an alteration in sperm functional quality, which is characterized by decreased acrosome integrity and mitochondrial activity, as well as by increased nuclear DNA fragmentation.
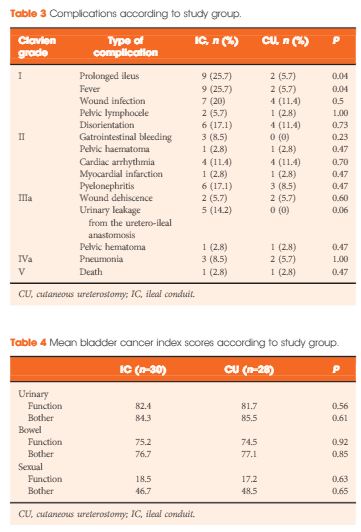
Complications and quality of life in elderly patients with several comorbidities undergoing cutaneous ureterostomy with single stoma or ileal conduit after radical cystectomy
NicolaLongo*,CiroImbimbo*,FerdinandoFusco*,VincenzoFicarra†,Francesco Mangiapia*,GiuseppeDiLorenzo‡,MassimilianoCreta§,VittorioImperatore§ and VincenzoMirone*
To compare peri-operative outcomes and quality of life (QoL) in a series of elderly patients with high comorbidity status who underwent single stoma cutaneous ureterostomy (CU) or ileal conduit (IC) after radical cystectomy (RC).
Patients and Methods
The clinical records of patients aged >75 years with an American Society of Anesthesiologists (ASA) score >2 who underwent RC at a single institution between March 2009 and March 2014 were retrospectively analysed. After RC, all patients included in the study received an IC urinary diversion or a CU with single stoma urinary diversion. Preoperative clinical characteristics as well as intra- and postoperative outcomes were evaluated and compared between the two groups. In addition, the Bladder Cancer Index (BCI) was used to assess QoL.
Results
A total of 70 patients were included in the final comparative analyses. Of these, 35 underwent IC diversion and 35 CU single stoma diversion. The two groups were similar with regard to age, gender, ASA score, type of indication and pathological features. Operating times (P < 0.001), estimated blood loss (P < 0.001), need for intensive care unit stay (P = 0.01), time to drain removal (P < 0.001) and length of hospital stay (P < 0.001) were significantly higher in patients undergoing IC diversion. The number of patients with intra- (P = 0.04) and early postoperative (P = 0.02) complications was also significantly higher among those undergoing IC diversion. Interestingly, the mean BCI scores were overlapping in the two groups.
Conclusions
The present results show that CU with a single stoma can represent a valid alternative to IC in elderly patients with relevant comorbidities, reducing peri-operative complications without a significant impairment of QoL.
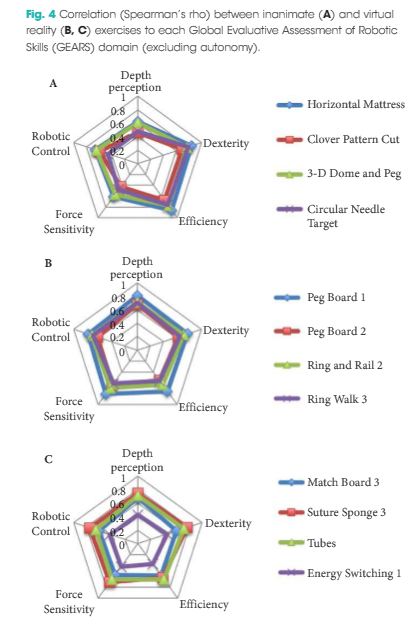
To compare user performance of four fundamental inanimate robotic skills tasks (FIRST) as well as eight da Vinci Skills Simulator (dVSS) virtual reality tasks with intra-operative performance (concurrent validity) during robot-assisted radical prostatectomy (RARP) and to show that a positive correlation exists between simulation and intra-operative performance.
Materials and Methods
A total of 21 urological surgeons with varying robotic experience were enrolled. Demographics were captured using a standardized questionnaire. User performance was assessed concurrently in simulated (FIRST exercises and dVSS tasks) and clinical environments (endopelvic dissection during RARP). Intra-operative robotic clinical performance was scored using the previously validated six-metric Global Evaluative Assessment of Robotic Skills (GEARS) tool. The relationship between simulator and clinical performance was evaluated using Spearman’s rank correlation.
Results
Performance was assessed in 17 trainees and four expert robotic surgeons with a median (range) number of previous robotic cases (as primary surgeon) of 0 (0–55) and 117 (58–600), respectively (P = 0.001). Collectively, the overall FIRST (ρ = 0.833, P < 0.001) and dVSS (ρ = 0.805, P < 0.001) simulation scores correlated highly with GEARS performance score. Each individual FIRST and dVSS task score also demonstrated a significant correlation with intra-operative performance, with the exception of Energy Switcher 1 exercise (P = 0.063).
Conclusions
This is the first study to show a significant relationship between simulated robotic performance and robotic clinical performance. Findings support implementation of these robotic training tools in a standardized robotic training curriculum.
Decisions regarding thromboprophylaxis in urologic surgery involve a trade-off between decreased risk of venous thromboembolism (VTE) and increased risk of bleeding. Both patient- and procedure-specific factors are critical in making an informed decision on the use of thromboprophylaxis. Our systematic review of the literature revealed that existing guidelines in urology are limited. Recommendations from national and international guidelines often conflict and are largely based on indirect as opposed to procedure-specific evidence. These issues have likely contributed to large variation in the use of VTE prophylaxis within and between countries. The majority of existing guidelines typically suggest prolonged thromboprophylaxis for high-risk abdominal or pelvic surgery, without clear clarification of what these procedures are, for up to 4 weeks post-discharge. Existing guidance may result in the under-treatment of procedures with low risk of bleeding and the over-treatment of oncological procedures with low risk of VTE. Guidance for patients who are already anticoagulated are not specific to urological procedures but generally involve evaluating patient and surgical risks when deciding on bridging therapy. The European Association of Urology Guidelines Office has commissioned an ad hoc guideline panel that will present a formal thromboprophylaxis guideline for specific urological procedures and patient risk factors.
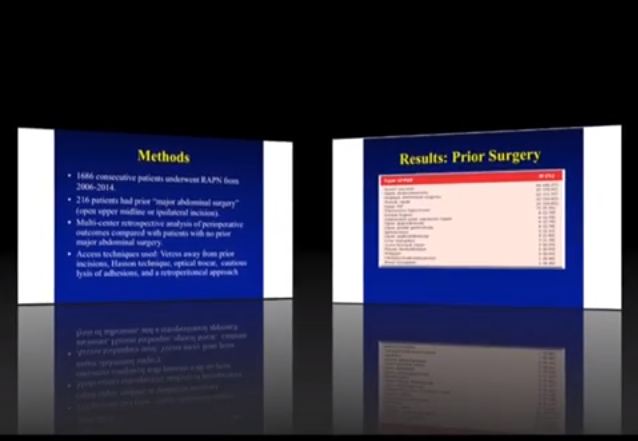
To evaluate the outcomes of robot-assisted partial nephrectomy RAPN after major prior abdominal surgery (PAS) using a large multicentre database.
Patients and methods
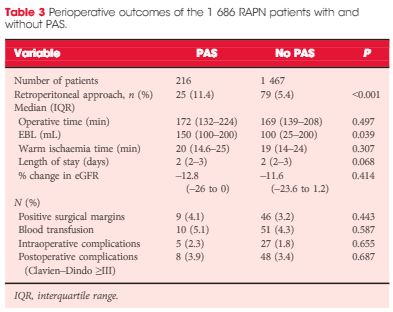
We identified 1 686 RAPN from five academic centres between 2006 and 2014. In all, 216 patients had previously undergone major PAS, defined as having an open upper midline/ipsilateral incision. Perioperative outcomes were compared with those 1 470 patients who had had no major PAS. The chi-squared test and Mann–Whitney U-test were used for categorical and continuous variables, respectively.
Results
There was no statistically significant difference in Charlson comorbidity index, tumour size, R.E.N.A.L. nephrometry score or preoperative estimated glomerular filtration rate (eGFR) between the groups. Age and body mass index were higher in patients with PAS. The PAS group had a higher estimated blood loss (EBL) but this did not lead to a higher transfusion rate. A retroperitoneal approach was used more often in patients with major PAS (11.2 vs 5.4%), although this group did not have a higher percentage of posterior tumours (38.8 vs 43.3%, P = 0.286). Operative time, warm ischaemia time, length of stay, positive surgical margin, percentage change in eGFR, and perioperative complications were not significantly different between the groups.
Conclusions
RAPN in patients with major PAS is safe and feasible, with increased EBL but no increased rate of transfusion. Patients with major PAS had almost twice the likelihood of having a retroperitoneal approach.
To analyse oncological and functional outcomes 12 months after treatment of very-low-risk prostate cancer with radical prostatectomy in men who could have been candidates for active surveillance.
Patients and Methods
We conducted a prospective study of all men with very-low-risk prostate cancer who underwent radical prostatectomy at one of 14 participating centres. Validated patient questionnaires were collected at baseline and after 12 months by independent healthcare researchers. Biochemical recurrence (BCR) was defined as prostate-specific antigen (PSA) ≥0.25 ng/mL or treatment with salvage radiotherapy or with hormones. Urinary continence was defined as <1 pad changed per 24 h. Erectile function was defined as ability to achieve erection hard enough for penetration more than half of the time after sexual stimulation. Changes in tumour grade and stage were obtained from pathology reports. We report descriptive frequencies and proportions of men who had each outcome in various subgroups. Fisher’s exact test was used to assess differences between the age groups.
Results
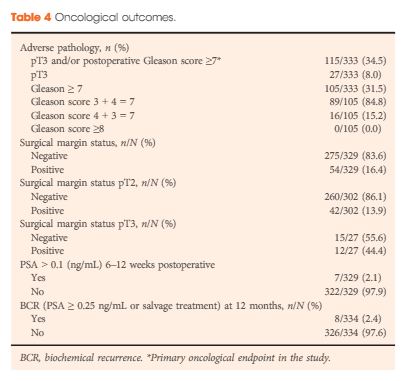
Of the 4003 men in the LAPPRO cohort, 338 men fulfilled the preoperative national criteria for very-low-risk prostate cancer. Adverse pathology outcomes included upgrading, defined as pT3 or postoperative Gleason sum ≥7, which was present in 35% of the men (115/333) and positive surgical margins, which were present in 16% of the men (54/329). Only 2.1% of the men (7/329) had a PSA concentration >0.1 ng/mL 6–12 weeks postoperatively. Erectile function and urinary continence were observed in 44% (98/222) and 84% of the men (264/315), respectively, 12 months postoperatively. The proportion of men achieving the trifecta, defined as preoperative potent and continent men who remained potent and continent with no BCR, was 38% (84/221 men) at 12 months.
Conclusions
Our prospective study of men with very-low-risk prostate cancer undergoing open or robot-assisted radical prostatectomy showed that there were favourable oncological outcomes in approximately two-thirds. Approximately 40% did not have surgically induced urinary incontinence or erectile dysfunction 12 months postoperatively. These results provide additional support for the use of active surveillance in men with very-low-risk prostate cancer; however, the number of men with risk of upgrading and upstaging is not negligible. Improved stratification is still urgently needed.
The impact of re-transurethral resection on clinical outcomes in a large multicentre cohort of patients with T1 high-grade/Grade 3 bladder cancer treated with bacille Calmette–Guerin
Paolo Gontero1, Richard Sylvester2, Francesca Pisano1, Steven Joniau3, Marco Oderda1, Vincenzo Serretta4,Stephane Larre5, Savino Di Stasi6, Bas Van Rhijn7, Alfred J.Witjes8, Anne J. Grotenhuis8, Renzo Colombo9, Alberto Briganti9, Marek Babjuk10, Viktor Soukup10, Per-Uno Malmstrom11, Jacques Irani12, Nuria Malats13, Jack Baniel14, RoyMano14, Tommaso Cai15, Eugene K. Cha16, Peter Ardelt17, John Vakarakis18, Riccardo Bartoletti19, Guido Dalbagni20, Shahrokh F. Shariat16, Evanguelos Xylinas16, Robert J.Karnes21 and Joan Palou22
1Urology Clinic, Citta della Salute e della Scienza di Torino, University of Studies of Turin, Turin ,4Department of Surgical, Oncological and Stomatological Sciences, University of Palermo, Palermo, 6Policlinico Tor Vergata-University of Rome, Rome, 9Dipartimento di Urologia, Universita Vita-Salute. Ospedale S. Raffaele, Milan, 15Department of Urology, SantaChiara Hospital, Trento, 19Department of Experimental and Clinical Medicine, University of Florence, Florence, Italy, 2Formerly Department of Biostatistics, EORTC Headquarters, Brussels, 3Oncologic and Reconstructive Urology, Department of Urology, University Hospitals Leuven, Leuven, Belgium, 5Department of Surgical Science, John Radcliffe Hospital, University of Oxford, Oxford, UK, 7Department of Urology, Netherlands Cancer Institute – Antoni van Leeuwenhoek Hospital, Amsterdam, 8Department of Urology, Radboud University Nijmegen Medical Centre, Nijmegen, The Netherlands, 10Department of Urology, Motol Hospital, University of Praha, Praha, Czech Republic, 11Department of Urology, Academic Hospital, Uppsala University, Uppsala, Sweden, 12Department of Urology, Centre Hospitalier Universitaire La Miletrie, University of Poitiers, Poitiers, France, 13Genetic and Molecular Epidemiology Group, Spanish National Cancer Research Centre (CNIO), Madrid, 22Department of Urology, Fundacio Puigvert, University of Barcelona, Barcelona, Spain, 14Department of Urology, Rabin Medical Centre, Tel Aviv, Israel, 16Department of Urology, Weill Medical College of Cornell University in New York City, 20Department of Urology, Memorial Sloan Kettering Cancer Center, New York, NY, 21Department of Urology, Mayo Clinic, Rochester, MN, USA, 17Facharzt fur Urologie, Abteilung fur Urologie. Chirurgische Universitats klinik, Freiburg, Germany, and 18Department of Urology, Sismanoglio Hospital, University of Athens, Athens, Greece
To determine if a re-transurethral resection (TUR), in the presence or absence of muscle at the first TUR in patients with T1-high grade (HG)/Grade 3 (G3) bladder cancer, makes a difference in recurrence, progression, cancer specific (CSS) and overall survival (OS).
Patients and methods
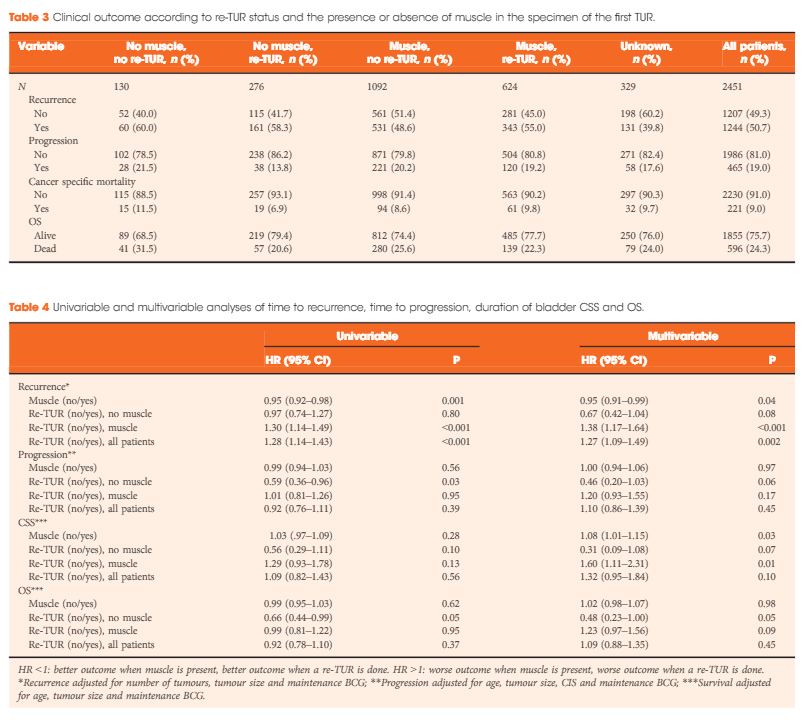
In a large retrospective multicentre cohort of 2451 patients with T1-HG/G3 initially treated with bacille Calmette–Guérin, 935 (38%) had a re-TUR. According to the presence or absence of muscle in the specimen of the primary TUR, patients were divided in four groups: group 1 (no muscle, no re-TUR), group 2 (no muscle, re-TUR), group 3 (muscle, no re-TUR) and group 4 (muscle, re-TUR). Clinical outcomes were compared across the four groups.
Results
Re-TUR had a positive impact on recurrence, progression, CSS and OS only if muscle was not present in the primary TUR specimen. Adjusting for the most important prognostic factors, re-TUR in the absence of muscle had a borderline significant effect on time to recurrence [hazard ratio (HR) 0.67, P = 0.08], progression (HR 0.46, P = 0.06), CSS (HR 0.31, P = 0.07) and OS (HR 0.48, P = 0.05). Re-TUR in the presence of muscle in the primary TUR specimen did not improve the outcome for any of the endpoints.
Conclusions
Our retrospective analysis suggests that re-TUR may not be necessary in patients with T1-HG/G3, if muscle is present in the specimen of the primary TUR.