May 2017 – About the Cover
The Article of the Month in this issue comes from Baltimore, Maryland. The cover image shows the local delicacy, Maryland crab cakes.

©istock.com/joecicak
Click here for this issue’s Table of Contents

The Article of the Month in this issue comes from Baltimore, Maryland. The cover image shows the local delicacy, Maryland crab cakes.
©istock.com/joecicak
Click here for this issue’s Table of Contents
April 2017 #urojc summary: Is SABR a viable therapeutic option for managing renal tumors in patients deemed unsuitable for surgery?
In April 2017, the International Twitter-based Urology Journal Club (@iurojc) #urojc reviewed an interesting recent article by Siva et. Al reporting their experience in a prospective cohort study utilizing Stereotactic Ablative Body Radiotherapy (SABR) on inoperable primary renal cell carcinomas. The article was made freely available courtesy of BJUI for the duration of the discussion (https://onlinelibrary.wiley.com/doi/10.1111/bju.13811/full). The journal club ran for 48 hours beginning on April 2nd at 21:00 UTC. The first author of the manuscript, Dr. Shankar Siva, a radiation oncologist at the Peter MacCallum Cancer Center joined the discussion using the Twitter handle @_ShankarSiva.
The study enrolled 37 total patients (T1a n=13, T1b n=23, and T2a n=1) due to one of three reasons: (1) deemed medically inoperable (n=28 Charlson Comorbidity >6), (2) high-risk group for surgery (n=11 high risk post-surgical dialysis), (3) refused surgery (n=1). The primary outcome measured was the successful delivery of radiotherapy. Secondary outcomes included (1) adverse events of radiotherapy, (2) local progression of the disease, (3) distant progression of the disease, and (4) overall survival.
@iurojc kicked things off with a starter question
If a tumour is inoperable due to patient morbidity, should we be doing anything at all?#urojc
— Urology JC #urojc (@iurojc) April 2, 2017
There was immediate debate regarding the validity of treating patients with inoperable tumors using alternative modalities.
@iurojc This is an outdated idea from the paternalistic era of medicine. Many live long enough to suffer from untreated & preventable progression.
— Drew Moghanaki, MD (@DrewMoghanaki) April 2, 2017
@DrewMoghanaki @iurojc Neither outdated nor paternalistic. https://t.co/TfduPLDba0 @uretericbud
— Patrick Kenney (@PatrickKenneyMD) April 2, 2017
@PatrickKenneyMD cited a retrospective analysis by Kutikov et. al (@uretericbud) of the SEER database on competing causes of mortality in elderly patients with localized RCC. The study reported the 5-year probability of mortality from non-cancer related etiology to be 11% while the RCC related mortality probability was 4%. The authors of the paper encourage that management decisions for localized RCC in older patients should take into account competing causes of mortality. @DrewMoghanaki argued that many patients will still suffer from the sequelae of cancer progression that could be prevented by treating with non-surgical modalities such as SABR.
@_ShankarSiva chimed in
@DrewMoghanaki @PatrickKenneyMD @iurojc @uretericbud Similar conversation in #lungcancer a decade ago; https://t.co/dn8Mec9IBj – SABR improved OS over no Tx in elderly @drdavidpalma #urojc
— Shankar Siva (@_ShankarSiva) April 3, 2017
@uretericbud questioned the comparison of two discrepant neoplasms
@_ShankarSiva @DrewMoghanaki @PatrickKenneyMD @iurojc @drdavidpalma #urojc not sure fair comparison. kinetics of progression of localized renal masses and lung masses vastly different
— Alexander Kutikov MD (@uretericbud) April 3, 2017
@_ShankarSiva @iurojc @uretericbud @DrewMoghanaki @PatrickKenneyMD @drdavidpalma Need to know if these were ~indolent tumors in very high risk patients. If so makes the treatment look fantastic. #urojc
— David Canes (@CanesDavid) April 3, 2017
@_ShankarSiva explained
@CanesDavid @iurojc @uretericbud @DrewMoghanaki @PatrickKenneyMD @drdavidpalma Agree – we treated > 4cms, or SRMs with initial surveillance and serial growth. We had a few distant failures; so not too indolent #urojc
— Shankar Siva (@_ShankarSiva) April 3, 2017
From Belgium, an important point was made about the question itself.
@iurojc Inoperable is not the same as short life expectancy otherwise you wouldn’t even have considered surgery! RT is a valid choice for many.
— Piet Ost (@piet_ost) April 3, 2017
While this conversation was occurring, a lively discussion on the utility of SABR compared to other established non-surgical modalities was taking place.
Why SABR and not cryo or RFA? Is there a potential for greater morbidity?#urojc
— Urology JC #urojc (@iurojc) April 2, 2017
@_ShankarSiva replied
@iurojc #urojc Good question – RFA / perc cryo often limited to exophytic SRMs, away from pelvis. SABR can ‘reach’ these safely @Rad_Nation #radonc
— Shankar Siva (@_ShankarSiva) April 2, 2017
Next, @CanesDavid posed a question regarding the most frequent factors of surgical disqualification in the cohort
@_ShankarSiva @iurojc @Rad_Nation How was inoperability determined? What were the typical limiting factors? #urojc
— David Canes (@CanesDavid) April 2, 2017
@CanesDavid @iurojc @Rad_Nation Surgeons may want to comment @declangmurphy @nickbrookMD @lawrentschuk – often CVS risk factors, need for RN in solitary func kidney #urojc
— Shankar Siva (@_ShankarSiva) April 2, 2017
@benchallacombe noted a limitation of the study which led to a discussion of the utility of one of the four secondary outcomes of the study- local progression.
@_ShankarSiva @iurojc @CanesDavid @Rad_Nation @declangmurphy @nickbrookMD @lawrentschuk #urojc appears no control/comparison group here & many with t1b/t2 tumours will go 2-5 years without progression. Too early for conclusion
— Ben Challacombe (@benchallacombe) April 3, 2017
@benchallacombe @_ShankarSiva @iurojc @CanesDavid @Rad_Nation @declangmurphy @lawrentschuk I think the soft endpoint of tumour growth is a helpful endpoint in these difficult studies. Not be all and end all, but helpful #urojc
— Nick Brook (@nickbrookMD) April 3, 2017
@nickbrookMD (co-author) cited an article by Crispen et. al that characterized the growth rate of untreated solid enhancing renal masses. @Rad_Nation proposed two follow-up studies that could be conducted.
@nickbrookMD @benchallacombe @_ShankarSiva @iurojc @CanesDavid @declangmurphy @lawrentschuk So another cohort could be used to test a nomogram for local growth & ideally cancer specific survival. Then test surg v RFA v SBRT #urojc
— Radiation Nation (@Rad_Nation) April 3, 2017
Even if these studies are conducted, there is skepticism around whether Urologists will view SBRT as a viable alternative treatment modality for RCC.
@Rad_Nation @benchallacombe @_ShankarSiva @iurojc @CanesDavid @declangmurphy @lawrentschuk I think surgeons won’t see SABR as another ‘option’ – rather a fall back when surgery doesn’t make sense #urojc
— Nick Brook (@nickbrookMD) April 3, 2017
@nickbrookMD @Rad_Nation @benchallacombe @_ShankarSiva @iurojc @CanesDavid @declangmurphy @lawrentschuk With change in age and comorbidity this will change I think. #prostatecancer had #EBRT “only” a long time. #urojc
— Alfred Honoré (@diamias) April 3, 2017
@iurojc posed an important question. What should be the overall goal of the urologist? Is it to cure cancer by all means? Or perhaps to find a balance between quality of life and management of the disease? SBRT may play a crucial role in the latter situation.
Putting aside comorbidity, what do you consider to be any factors that could make a renal tumour unsuitable for surgery? #urojc
— Urology JC #urojc (@iurojc) April 3, 2017
@iurojc If one prioritizes oncologic goal over function, there is no true inoperable tumor (if you can accept renal failure/dialysis as okay) #urojc
— David Y.T. Chen (@dytcmd) April 3, 2017
@iurojc Single kidney in a patient who doesnt want dialysis? #urojc
— Alfred Honoré (@diamias) April 3, 2017
To wrap things up, @iurojc asked a summary question.
What’s the next step to convince widespread use of SABR for renal tumours? Or are you sufficiently convinced? #urojc
— Urology JC #urojc (@iurojc) April 4, 2017
The authors of the manuscript provided a response and their thoughts on what needs to be done next.
@iurojc Role is in pts medically (incl sCKD) high risk for surgery with large and growing mass – in whom modern meds r extending life expec #urojc
— Nick Brook (@nickbrookMD) April 4, 2017
@nickbrookMD @iurojc Need more trials – this one might help https://t.co/T19jSnCeaM @lawrentschuk @DocJarad @Prof_IanD @ANZUPtrials @TROGfightcancer #urojc
— Shankar Siva (@_ShankarSiva) April 4, 2017
Thank you to everyone who participated in the April 2017 #urojc. Special thanks to the authors @_ShankarSiva and @nickbrookMD for joining in on the discussion and providing further insight to their work.
Akhil Saji is a third-year medical student at New York Medical College, Valhalla, NY.
Twitter @AkhilASaji
References
1. Siva, Shankar, et al. “Stereotactic ablative body radiotherapy for inoperable primary kidney cancer: a prospective clinical trial.” BJU international (2017)
2. Kutikov, Alexander, et al. “Evaluating overall survival and competing risks of death in patients with localized renal cell carcinoma using a comprehensive nomogram.” Journal of Clinical Oncology 28.2 (2009): 311-317.
3. Crispen, Paul L., et al. “Predicting growth of solid renal masses under active surveillance.” Urologic Oncology: Seminars and Original Investigations. Vol. 26. No. 5. Elsevier, 2008
It should surprise no one that I never agreed with the 2012 United States Preventive Services Task Force to give PSA a “D” rating that has led to decreases in U.S. rates of PSA testing, biopsies, and diagnosis of low- through high-risk cancer. I take care of men with prostate cancer in a multidisciplinary clinic at a dedicated cancer hospital. I perform robotic surgeries and manage over a 1,000 men on active surveillance. If you search the BJUI blogs, you can find the often viewed (>80K) “Melbourne Consensus Statement on Prostate Cancer Testing” that included 15 authors who produced 5 consensus statements on the topic. There are 62 comments—comment #5 is a fairly famous one that equates the panel to “a group of 10 pig-farmers telling us we should eat more bacon.” So yes, I think I count as a pig farmer here. My maternal grandfather and great uncle farmed pigs in Western Tennessee, so it does run in the family.
Figure 1: It was either this or robotics
That said, it always seemed odd, that as a large country and major healthcare market, we rolled out PSA screening in the 1990s with wild enthusiasm and without data on benefit, only to then try and roll it back in when faced with two conflicting level 1 evidence studies. Meanwhile, the American Urological Association guidelines recommended PSA screening (with the “shared decision making caveat”)—mostly mirroring the European study—for men ages 55-69 (also consensus statement 1 from the Melbourne consensus). However, a recent fact struck me during a conference talk—Urologists in the U.S. are estimated to order <10% of all PSA tests, and a vast majority are from primary care physicians. So in essence it doesn’t matter as much what we think of one guideline versus another, it’s what the primary care specialties think that matters. As the USPSTF is targeted at primary care, their D rating did have an effect—fewer PSA tests, biopsies, and diagnosis of all grades of cancer (not just Gleason 6). We have heard stories over the years that specialty exams in primary care were starting to feature PSA screening questions, and the “don’t screen” answer was the one you got credit for. But I was also never convinced that most primary care physicians were comfortable with abandoning screening either. They must have seen what we saw—real cancers presenting later stage.
Some memorable quotes along these years of debate:
“There is no evidence prostate carcinogenesis has declined.” Joel Nelson, J Urol 2015
“I believe the USPSTF recommendations have created confusion at the patient and primary physician level, and that this confusion did not likely result in more informed, shared decision making, but instead avoidance of the issue.” Samir Taneja, J Urol.
Amen. So now it’s 2017 and the USPSTF has looked at the data again. They’ve had their “analysis” methods on the web for a while so we know something was planned. I can’t find authorship credits anywhere—we always complained that no prostate cancer experts were involved in the past, and now wondering who is driving this ship. The take home messages are:
So really that’s it—3 main concepts. This is likely to be a significant impact in the U.S., depending upon whether or not primary care physicians change practice (and their exam questions are the same with a different correct answer).
Probably what is on your mind now is “why the change.” It does not appear to be one thing—not even recent publications revealing a more significant pattern of PSA contamination in the PLCO trial. The checklist seems to include: 1) PCLO “issues”, 2) more data from ERSPC and its subsets, 3) more data on treatment benefit, and 4) increased use of active surveillance in low-risk disease. So the balance tipped in favor of a “C” although they state the benefits and harms are still close. Fair enough.
As I re-read the 2013 Melbourne Consensus and compare to the 2017 USPSTF statement, there is a lot of overlap now. So congrats to the Melbourne group for getting it right in the first place. I, myself, did not see this coming—just another example of why I don’t invest in individual stocks or otherwise pretend to know the future.
I apologize as I re-read this, as I realize we Americans think the world revolves around us. Many of you certainly live in countries that are against routine screening and manage to get by. By all means, please sound off on what you think this means for the international picture of men’s health.
Figure 2: Scenic Melbourne at dusk
John W. Davis is BJUI Associate Editor for oncology. @jdhdavis
Comments on this blog have been closed due to high levels of spam.
London calling! On Sunday morning London called one hour earlier than I had planned – damn daylight saving time! Last nights’ celebrations with urology friends from around the world at the ESRU (European Society of Residents in Urology) dinner party made me pay. Yet this was going to be a great meeting day.
Sunday morning sessions served as a wake-up call after a short night due to daylight saving time.
Dr. Rajesh Nair has already reported on a great kick-off and continuation of the EAU17 congress in his blog on congress days 1 & 2.
The Sunday programme started with a plenary session in eURO auditorium on redefining and optimising contemporary bladder cancer care. The EAU chose a great concept for the plenary session by presenting an easily digestible mix of different lectures: Experts in the field used case discussions to illustrate real-life clinical scenarios and everyday issues for urologist. Speakers delivered their best arguments in the debates on pros and cons on urgent clinical questions. Finally, State-of-the-art lectures summarized the most important aspects in the field.
EAU17 Delegates joining the congress action.
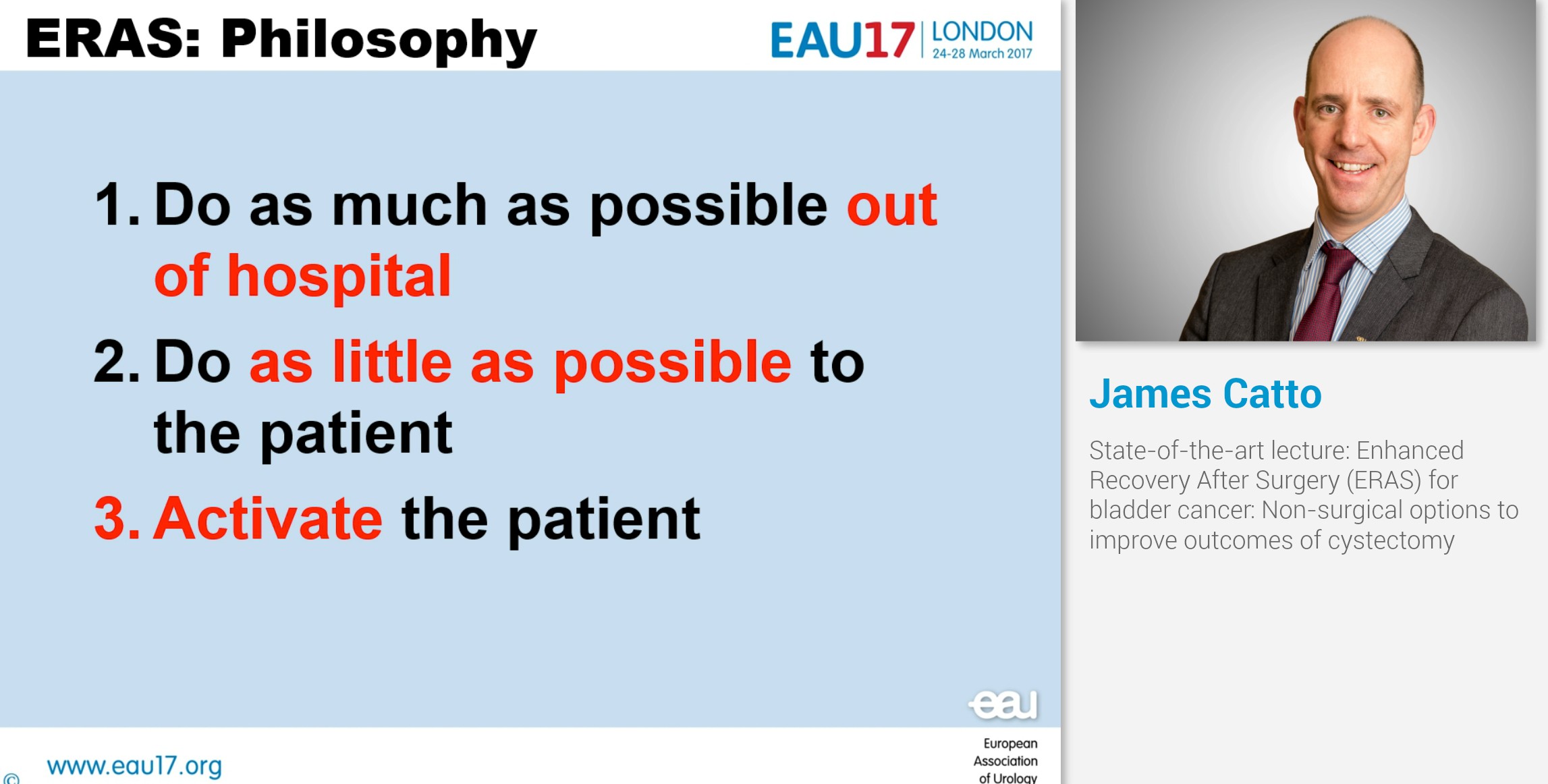
Sunday’s State-of-the art lectures on bladder cancer were held by James Catto and Walter Artibani. Catto reported on “Enhanced Recovery After Surgery (ERAS) for bladder cancer: Non-surgical options to improve outcomes of cystectomy”. Catto systematically covered 22 ERAS items on preoperative, intraoperative and postoperative measures. Appliance of ERAS for radical cystectomy yielded better outcomes for length-of-stay as well as readmission and transfusion rates when compared to traditional recovery concepts.
State-of-the-art lecture: Three principles of the Enhanced Recovery after Surgery (ERAS) Philosophy.
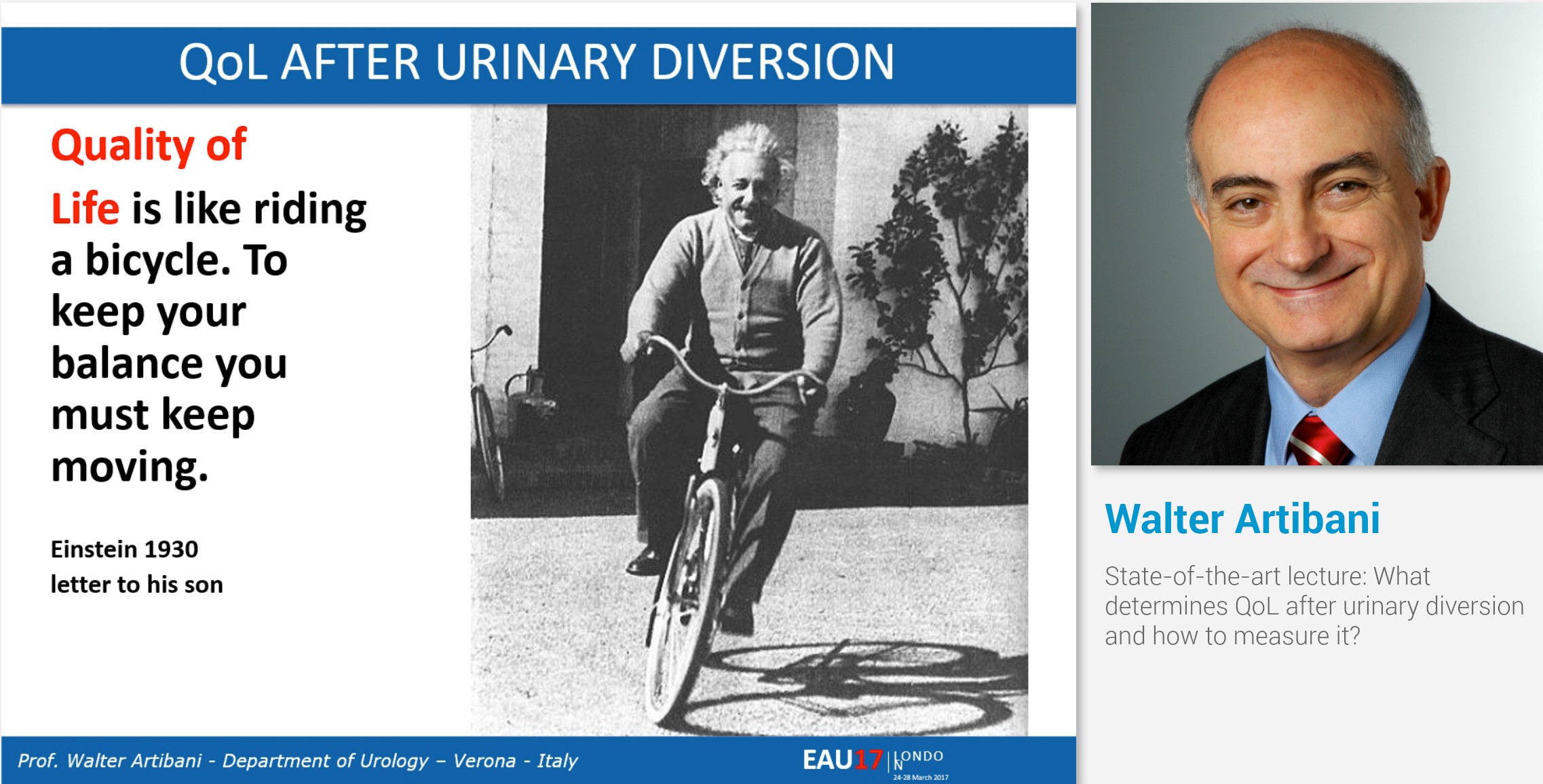
The second State-of-the-art lecture by Walter Artibani gave perspectives on “What determines Quality-of-Life after urinary diversion and how do we measure it?” Artibani pointed out that we have to do a better job in defining and researching health-related quality of life in order to compare outcomes of urinary diversions. Multidisciplinarity is a must and there is room and need for enhanced long-term personalized information and support programs.
Quality of Life after urinary diversion – Walter Artibani’s twist of Albert Einstein’s wisdom.
Besides scientific meetings, the Annual Meeting of course is the place for board meetings of the EAU bodies. The EAU Section Office Members took the opportunity to step out of the congress and enjoy London’s incredibly good weather.
EAU Section Office Members enjoying London’s sun for a group photo.
At high noon it was time for me to join the Advanced Course on Social Media – take it to the next level! An expert panel of Social media users in urology gave insights on the wide variety of Social media use in our field. Twitter queen Stacy Loeb (@LoebStacy) gave examples on the use of social media for scientific research and for dissemination of content. Matthew Cooperberg (@dr_coops) showed in his talk “reputation management” why and how urologists should take care of their digital self. Finally, Inge van Oort (@onco_uroloog) presented do’s and don’ts of Twitter use emphasizing the importance of Social Media guidelines.
Great conclusion of the advanced Social Media Course by @LoebStacy.
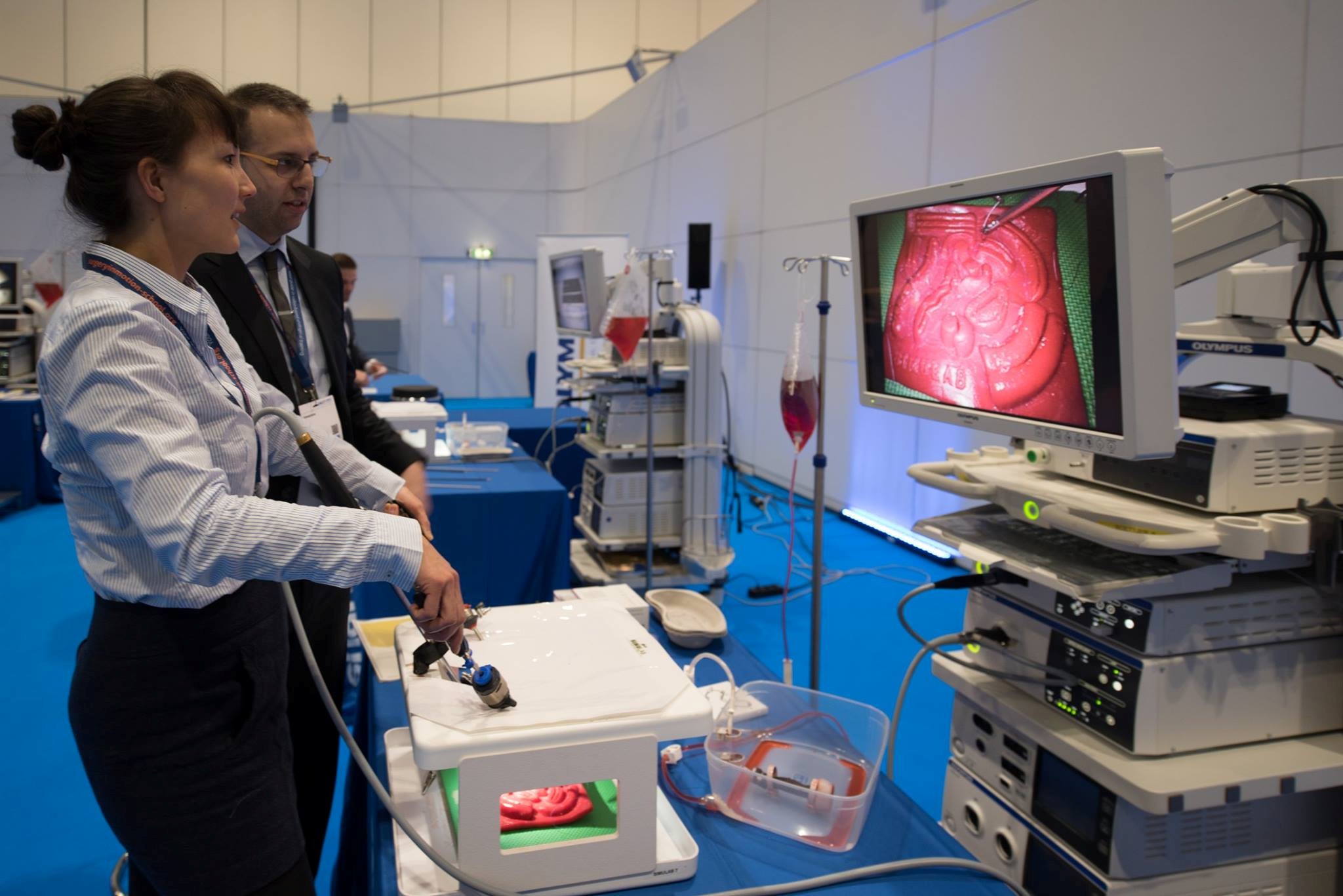
Yet, ESU Courses weren’t limited to lectures and discussions. HOT – Hands on Training was offered to delegates with 1-on-1-supervision. I was amazed by the variety of simulators and technical equipment for course participants. But why would they use red irrigation fluid? – Making the TURP simulation a more realistic experience? 
Simulation and tutoring during European School of Urology Hands-on-training courses.
On Monday morning the EAU launched a new initiative: the Young Urologist Office provided a new course format: the EAU Leadership Course. Ambitious urologists from all over the world gathered to expand on their leadership skills: What are my leadership styles? Can I flex my style? Am I effective? These were only some of the aspects covered by a team of specialized leadership coaches.
One key skill for leadership: great rhetorical skills!
Another thing I liked about the EAU congress was the professional media coverage – EAU TV offered short interviews covering highlights from abstract sessions, plenary sessions and insights from the EAU bodies. It was EAU TV that attracted my attention to Amanda Chung’s study “Is your career hurting you? – The ergonomic consequences of surgery in 701 urologists worldwide”. Against common presumption, Chung et al. didn’t find a dose-response relationship between volume of surgeries performed and back pain. A protective effect against back pain was found for exercise, instead increasing weight and BMI were associated with higher pain – thanks for these insights! I definitely aim for a lifestyle change after hearing these findings!
EAU TV enriches the conference experience.
There were a lot of things to learn during the congress. During the congress first-ever e-Poster Abstract Session on New technologies: Urology and multimedia, I learned from session chair and BJUI’s editor-in-chief Prokar Dasgupta that the highest cited paper on Altmetrics in 2015 was on a new antibiotic that kills pathogens without detectable resistance. Maybe this is why the EAU heavily announced it’s thematic session on infections in urology: “Killer bacteria and viruses in urology”. One must-read I got from this session was an update on the management of sepsis and septic shock.
Highlights from the EAU Infectious diseases session “Killer bacteria and viruses in urology”.
As usual the EAU congress featured lots of live and semi-live surgeries. For some of them the Copenhagen Room wasn’t quite enough to accommodate all delegates interested.
Live and semi live surgery as usual attracting lots of EAU delegates.
The EAU congress truly offered a cocktail of everything: the latest science presented in plenary & poster sessions, education, updates on guideline knowledge and of course lots of networking in form of meeting, greeting and tweeting.
Finally, my EAU17 journey ended on Monday night after lots of congress input, short nights and a great time meeting urology friends from around the world. Thanks a lot to all organisers and contributors for your hard work and great performance! See you in Copenhagen!
Hendrik Borgmann, Urologist, University Hospital Mainz
@HendrikBorgmann
≠WeAreNotAfraid. Perhaps the standout memory of EAU – London 2017. The 32nd Annual EAU Congress in London was marked with a message of defiance from colleagues and delegates from London, Great Britain, Europe and Worldwide. These were messages of solidarity, which rang through in person and on social media after an attack at Westminster. It was quite simple. London, Europe and the World will continue regardless of these tragic events and our urological fraternity beautifully demonstrated this as days following, a record-breaking attendance of 12000 delegates from over 123 countries descended to the Excel Centre in London, UK.
EAU-2017 had surpassed many a milestone. A record breaking 5000 abstracts were submitted for poster and video presentations from over 81 countries. 1200 presentations were displayed across 300 poster and video sessions. This year showcased an expansion of the number of plenary sessions from 4 to 7 allowing for a greater choice for all delegates. The quality, breadth and expertise behind the EBUS educational courses must be commended. Finally, as always, live surgery, which has year on year, proved to be popular was broadcast from Guy’s Hospital, London. They showcased the crème de la crème of surgical talent from live procedures with over 30 surgeons involved in operating, moderating, acting as patient advocates and in organisation. I, as I am sure all delegates extend our gratitude to the patients involved during the live surgical broadcast.
The camaraderie was clear to see. One could not take more than ten steps without running into a colleague or friend. It was a perfect opportunity to catch up, network and build relationships. Perhaps it was Prof. Sir Bruce Keogh (NHS England’s Medical Director and Commissioner of the Commission for Health Improvement (CHI)) who described it best in his opening address: ‘meetings like this are vitally important since it is at these occasions that knowledge and professional links are developed, and at these events ideas take seed and take hold: the important ideas that will later lead to significant work and progress in medicine.”
In addition, the opening ceremony showcased some the serious talent in urology. Awards for Prof. Paul Abrams, Prof. Per-Anders Abrahamsson, Prof. Christian Gratzke, Dr. Riccardo Autorino and Mr. Richard Turner-Warwick demonstrated their commitment, hard work and dedication to the specialty.
Day 1 began with multiple subspecialty meetings and meetings between affiliated sections. These themed discussions were stimulating and really addressed the trials and tribulations as well as successes in the delivery of urology worldwide. Day 1 also showcased a fantastic session organised by the prostate cancer prevention group. They examined the role of active surveillance in low risk prostate cancer with specific reference to data from ProtecT, ESRPC and the PLCO trials. Prof. Hamdy gave a comprehensive overview of the ProtecT study and reminded the audience that the risk of death from prostate cancer remains low (1% over ten years), and that surgery and radiotherapy although reduce cancer progression can result in bothersome side effects. The increasing role of urine based biomarkers; microRNA, imaging and genetic testing were all discussed when redefining the cohort of patients suitable for active surveillance.
The night ended with drinks at the Healtap, a bar outside Guy’s hospital, London. This was a throwback to the past for many. Old friends and colleagues, past fellows and current urologists all gathered to reminisce about past UK experiences. Following this, a late night serious session of serious recording and video production ensued with Declan Murphy and Alastair Lamb. For those open surgical protagonists who wonder ‘what have the robots ever done for us?’ I encourage you to watch:
The opening plenary session of Day 2: ‘Sleepless nights: Would you do the same again?’ chaired by Mr. Tim O’Brien critically re-evaluates some of the management decisions for kidney cancer from a medico-legal perspective. This session was fascinating and almost akin to a TV drama. A medico-legal lawyer (Mr. Leigh) vociferously cross-examining key members of faculty and an audience watching them sweat over what would have been initially perceived an acceptable clinical decision. A key message: allow your patients to take on decisions and not shoulder the entire burden yourself and the phrase; ‘your skills are for your patient, your notes are for yourselves’ continues to resonate.
Another EAU annual conference goes by with yet more casualties from a verbal punch up. The second session showcased a debate on robotic salvage prostatectomy between Declan Murphy and Axel Heidenreich. Perhaps the blood spilt from this joust reminded the audience that despite the rising bank of evidence favouring salvage prostatectomy, there will always remains debate when a salvage procedure is associated with increased morbidity and risk for the patient.
The ‘twitosphere’ was heavily active. The beauty of this as always is that if you were to miss sessions, lectures or abstracts, the ability to follow them on twitter in real time adds another dimension to conference attendance.
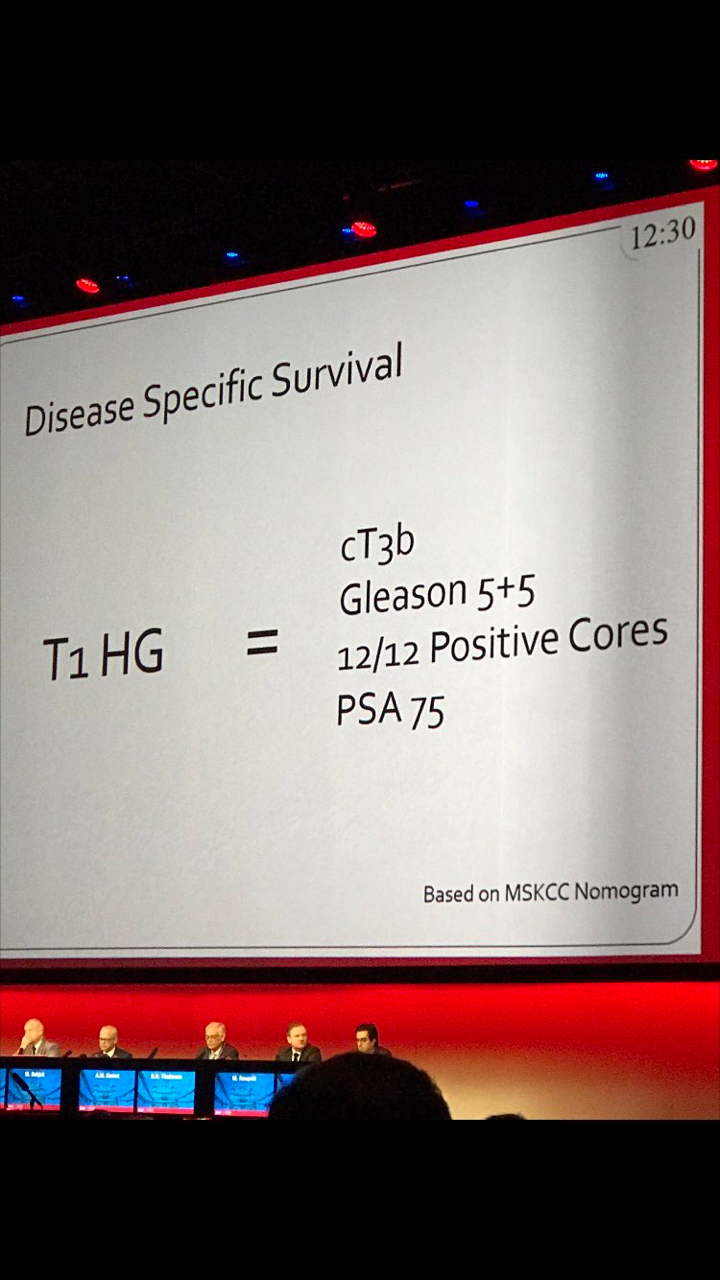
The most re-tweeted slide was presented by Dr. Ashish Kamat, a simple yes incredibly powerful slide demonstrating the equivalence in disease specific survival between high grade T1 urothelial carcinoma of the bladder and advanced prostate cancer reminded us all of the need to be vigilant and aggressive with high grade non muscle invasive disease of the bladder.
Day 2 brought out some of the best in abstracts, EBUS courses and updates in clinical trials. The latest developments in urological research include: the PROstate MRI Imaging Study (PROMIS) trial results reviewed by Hashim Ahmed and futher evidence and discussion from the Prostate Testing for Cancer and Treatment (ProtecT) trial by Freddie Hamdy. Prof. Jim Catto gave an eloquent talk examining the role of the enhanced recovery programme in radical cystectomy.
What a fantastic start to the meeting! As you shall see, the remainder of the meeting did not disappoint. Dr. Hendrick Borgmann will reveal all in the update of day 3 and 4.
Mr. Rajesh Nair
Fellow in Robotics and Uro-Oncology
The Royal Melbourne Hospital & Peter MacCallum Hospital, Melbourne, Australia
Twitter: @nairajesh
TRoMbone is launched! The UK feasibility randomised trial Testing radical prostatectomy in men with prostate cancer and oligoMetastases to the bone has opened at Oxford University Hospitals (PI Freddie Hamdy), University College London Hospitals (PI John Kelly) and Royal Surrey County Hospital (PI Chris Eden). Men <75 with newly-diagnosed prostate cancer and 1-3 skeletal lesions on any standard-of-care imaging (CT, bone scan, MRI, or PET) who are fit for surgery and deemed to be technically operable are eligible. Emerging but lower-quality data suggests a role for treatment of the primary tumour in men with oligo-metastatic prostate cancer and this UK study will investigate this question with level 1 evidence.
Participants will be randomly allocated to standard-of-care treatment (hormones +/- chemotherapy) versus standard-of-care treatment plus surgery to remove the prostate and draining lymph nodes (radical prostatectomy plus extended pelvic lymphadenectomy). A qualitative recruitment investigation to optimise accrual will be conducted by the University of Bristol (Caroline Wilson) and biologic samples will be collected, processed and stored in a repository at the Institute of Cancer Research (Gerhardt Attard).
We will assess technical feasibility, safety and complications of surgery in oligo-metastatic prostate cancer, and examine ways to improve recruitment in this pilot study. TRoMbone is managed by the Surgical Intervention Trials Unit at the University of Oxford and funded by the Prostate Cancer Foundation and The Urology Foundation.
We need to recruit 50 men over a 12-month period, and are seeking referrals from other centres to increase accrual. Centres that demonstrate ability to refer eligible patients will be able to take part in the main trial if we can demonstrate feasibility in this phase and get funding for the larger study.
So please look out for these patients and send them to me at UCLH, Freddie in Oxford, or Chris in Guildford. One of the three of us will do the surgery if they get randomised to it, but of course you’re welcome to come with the patients. If you have any queries please contact me, the study CI (P. Sooriakumaran (PS); prasanna.sooriakumaran@nds.ox.ac.uk) or the study co-ordinator (Neelam Hassanali; trombone@nds.ox.ac.uk). You can start them on androgen deprivation and ‘stop the clock’ before you refer them to us. The extra burden of participating in this study is minimal. They will require one visit for consent, and one follow-up visit at 3 months after randomisation. The surgical group will also have two other visits for their surgery and catheter removal. The rest of the follow-up can be done back at your referring centre or with us, whatever you and the patient prefer. If it’s your standard policy to give them chemotherapy or metastasis-directed therapy with SBRT then you can still do that as part of the study.
With your help we can demonstrate that this study is feasible in the UK and we can lead the way in the surgical management of oligo-metastatic prostate cancer.
P. Sooriakumaran [social type=”facebook” opacity=”dark’ label=’PLACE_LINK_HERE[/social]
BMedSci(Hons) BMBS(Hons) PhD PGCMedLaw ADCClinInv FRCS(Urol) FEBU USLME
Consultant Urological Surgeon, UCL Hospitals NHS Foundation Trust & Honorary Clinical Senior Researcher, University of Oxford
The BJUI supports clinical trials. Plain, simple, and with some new strategies.
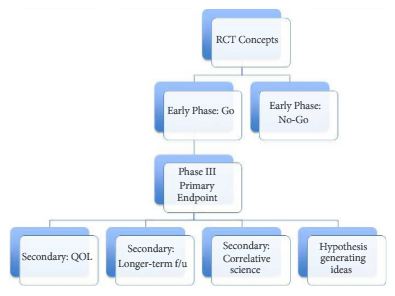
Randomised clinical trials (RCTs) are the highest level of evidence-based medicine. We know this to be true, but we also know that RCTs are a challenge to fund, accrue patients, execute, and follow to endpoints. From a statistician’s point of view, RCTs provide unbiased estimates of the effects of different treatments. From a clinician’s point of view, RCTs provide the grandest of experiments in nature – a true test of option A vs option B. We are thrilled when one option beats the other. We can be satisfied if the options are equivalent, at least knowing the matter is settled and move on to the next question. Either way, the story lines can be rich with ongoing debate, drama, and analysis: were the cohorts truly equivalent? Was the study population generalisable? Were the treatments contemporary? Were there unintended harms/toxicities?
Allow us to illustrate some examples of what we propose to our readers. In 2003, Thompson et al. [1] published the famous Prostate Cancer Prevention Trial in the New England Journal of Medicine: ‘The influence of finasteride on the development of prostate cancer’. This landmark study has been cited 2541 times, according to Google Scholar. Looking further at impact, one can go to the www.swog.org site and query the protocol ‘SWOG-9217’ and see that over 150 publications have been produced using this dataset (16 in 2016!). Several publications pre-dated the primary endpoint paper and discussed trial design, the dilemma of chemoprevention, and updates to trial progress. Post primary endpoint, publications have looked at multiple strategies – costs, the high-grade findings, longer-term follow-up, biopsy findings from the placebo arm, etc. Just last year, the UK made its mark on the prostate cancer world with the landmark Prostate Testing for Cancer and Treatment (ProtecT) study [2]. Again, we see the primary endpoint paper in the New England Journal of Medicine, but secondary endpoint papers, such as the quality-of-life outcomes are in the BJUI [3], and a mortality outcome analysis for trial screen failures in European Urology [4].
The BJUI can support clinical trial efforts through multiple pathways. Certainly, we would love to receive a primary endpoint paper from an important RCT in urology. We can also have impact by featuring important secondary endpoint papers, trial design papers (preferably ones that read like a good review article, with the trial proposed as the ‘answer’ to the dilemma), as well as smaller/early phase I–II trials that are stand-alone pieces of key knowledge. Figure 1 shows a possible flow chart of a RCT with each box representing possible publication points. In addition to content in the BJUI, our webpage Blogs section has a ‘rapid response team’ to start immediate dialogue on important RCTs published in other journals. For example with the recent Yaxley et al. [5] trial in the Lancet, our blogs section, led by Declan Murphy, had over 10 000 views and over 50 follow-up comments. So clearly, our readers care about RCTs.
Figure 1. A possible flow chart of a randomised clinical trial (RCT) with each box representing possible publication points. QOL, quality of life; f/u, follow-up.
Finally, the BJUI can help with RCTs in two more ways. For the reader, we will highlight RCT-related papers in their native sections (i.e. oncology, functional, education) with a special ‘Trials’ headline, and will invite experts to comment on the significance of the study. For reviewers and authors, we will be critical on RCT design, such that flaws are identified, and papers not given inflated significance. It is frustrating to receive papers that lack adequate reporting on what researchers did, RCT-related papers submitted to the BJUI frequently fail to adhere to the 2010 Consolidated Standards of Reporting Trials (CONSORT) guidance for reporting RCTs, which potentially leads to major revisions, if not outright rejection. The CONSORT requirements are on our author submission guidelines, but ideally these are read and adhered to in advance, as many are not possible to correct after the fact. Recently, we have also added that all RCTs must be registered (i.e. clinicaltrials.gov or similar) before the first patient is enrolled.
*MD Anderson Cancer Center, Houston, TX, USA and †University of Aberdeen, Aberdeen, UK
Davis, J. W. and MacLennan, G. (2017), The BJUI‘s clinical trials initiative. BJU International, 119: 503. doi: 10.1111/bju.13837
The Article of the Month authors in this issue are from Norfolk and Norwich University Hospital, Norwich, UK.
©istock.com/chris2766
Click here for this issue’s Table of Contents
Canberra, our nation’s capital and the host city for the 2017 USANZ ASM, is a gem in its own right, but one which was created to satiate two feuding states locked in a bitter rivalry. In 1908, Canberra embodied the very meaning of compromise and collaboration, a technique which has garnered much success for our Country over the ensuing 100 odd years. Arguably the first official Australian collaborative effort, this way of thinking has become an almost uniquely Australian attribute and a strength imbued in our national pride.
Canberra from up high, a breathtaking backdrop for a fantastic USANZ ASM.
Given this year’s mantra of: “Capitalising on our strengths” It is perhaps fitting then, that the 70th anniversary of the Urological Society of Australia and New Zealand (USANZ) Annual Scientific Meeting (ASM) including the Australia and New Zealand Urological Nurses Society (ANZUNS) 22nd ASM, should be held in such a location. In addition to providing some wonderful tourist opportunities for guests including the War Memorial, the National Gallery and Parliament House.
Convenors A/Prof Nathan Lawrentschuk and Kath Schubach went to great efforts to successfully welcome both national and international guests and Scientific Program Directors A/Prof Shomik Sengupta and Carla D’Amico ensured a star-studded academic program addressing contemporary updates in Urological evidence based practice, which were aptly discussed both inside and outside the confines of the National Convention Centre.
Senior YURO members standing outside Parliament House (from left to right): Dr. Daniel Christidis, Dr. Tatenda Nzenza, Dr. Todd Manning, Dr. Shannon McGrath
The representation by International faculty was exceptional, with countless urological household names from world leading centres across the globe both involved in the academic program and socially. Urological goliaths including Prof. Christopher Chapple, Prof. Prokar Dasgupta and Prof. Laurence Klotz weighed in on various topical issues providing an intercontinental perspective that complimented the equally impressive national line-up of speakers.
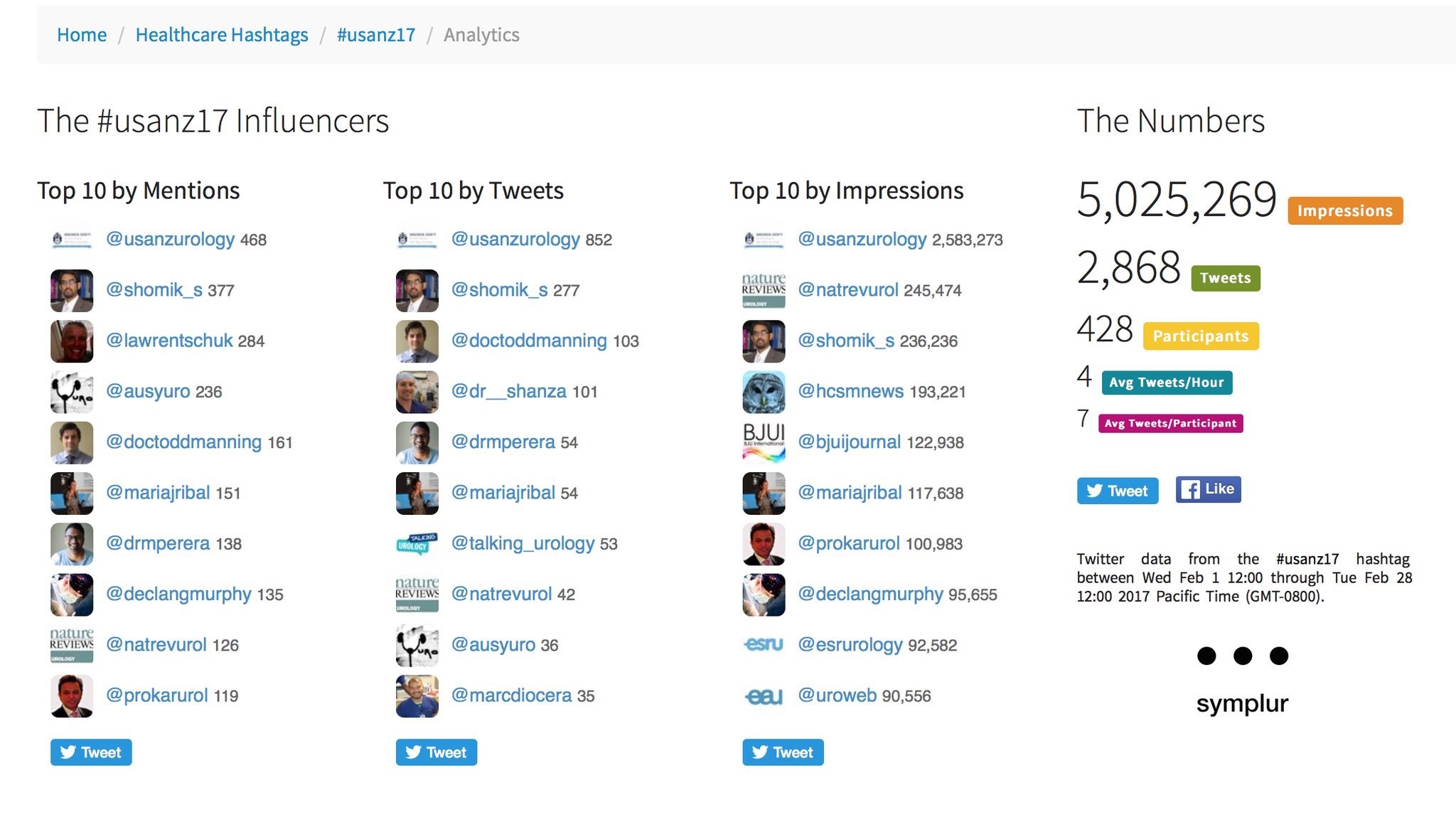
As with previous years, use of social media was rife, with those not able to attend kept in the loop via #Usanz17 and a steady stream from the ever focused twitterati. The ASM provided more than 5 million impressions and over 2800 individual tweets from more than 400 participants. The usual suspects were eminent as always, along with a few newcomers who provided impact in their own right. The official USANZ 2017 App also kept participants up to date via timely notifications and was user friendly.
Guests were spoilt for choice in the convention centre during well timed breaks, which was perpetually abuzz with attendees networking. In the background the ‘Talking Urology’ team headed by Mr Joseph Ischia and A/Prof Nathan Lawrentschuk provided a steady stream of captivating interviews with guests, regarding a myriad of urological topics. Simultaneously, numerous academics gave brief summaries of research posters during allocated presentation sessions. Exhibitors provided a captivating backdrop for these activities including many hands-on simulators and challenges for those keen to test their dextrous mettle. All the while guests relished a variety of delectable culinary options.
Guests networking at the Gala Dinner, whilst being entertained by opera classics in the Great Hall foyer of Parliament House
The meeting’s common themes were strong and pertinent to contemporary urology. They centred around collaborative research efforts such as the ANZUP trials group and the Young Urology Researchers Organisation (YURO), technology especially PSMA PET and social media and social justice including women in urology and operating with respect. Discussions were directed by chairpersons during purposefully allocated Q&A times at the conclusion of each session, a new and well received addition to this years meeting. This was generously embraced by both senior and junior academics and led to intriguing symposiums and at times heated debate.
The first official day of proceedings provided a smorgasbord of morning and afternoon workshops ranging from technical skills courses to the medico-legal implications of E-Health and technology. This was followed by an allocated networking session for Urology trainees with International faculty.
Officially opening the conference in the Royal Theatre of the convention centre, A/Prof Lawrentschuk introduced this year’s Harry Harris orator; Elizabeth Cosson, AM CSC. Her speech entitled “leading with grit and grace” eloquently detailed her journey in the armed forces and highlighted the difficulties of the unmistakably imbalanced workplace for women in the military. Her talk clearly underlined her role in not only forging a highly successful career for herself but also for those women following in her footsteps. Her inspiring dialogue was synchronous with contemporary issues surrounding Urological practice, especially concerning equality for women but more resolutely, appropriate equity both in training and established practice.
With the tone well established for an exceptional meeting, guests enjoyed a variety of canapés and drinks in the exhibition hall, unwinding with social discussion.
YURO President, Dr Todd Manning talks to young researchers with help from Prof. Henry Woo and A/Prof. Lawrentschuk during the YURO annual meeting
Plenary sessions aplenty began the second day of proceedings with International academic giants including Prof. Klotz, Prof. Chapple, Prof. Traxer and Prof Nitti mixed in with National heavy hitters such as Prof Frank Gardiner, Mr Daniel Moon and outgoing USANZ president Prof. Mark Frydenberg.
Afternoon sessions included subspecialty discussions and some stellar Podium Poster presentations, with an especially impressive mix of senior and junior researchers regarding countless and diverse urological topics.
Heralding the beginning of another exceptional day, the ‘Women in Urology’ breakfast symposium chaired by Dr Anita Clark along side distinguished panellists including Dr Caroline Dowling and Dr Eva Fong was a conference stand out for many.
Following this, more plenary sessions filled the remainder of the pre-lunch program, leading into the highly anticipated Keith Kirkland and Villis Marshall presentations by Urology SET trainees. The presentations did not disappoint. As in previous years, research of unyielding professional and academic quality was offered by the group of future urologists, who as is tradition weathered the gauntlet of probing and tough questions from the floor. All presentations were captivating in their own right. 2017 Villis Marshall winner Dr Marlon Perera presented ground-breaking research regarding the reno-protective role of zinc in contrast nephropathy. Dr Amila Siriwardana was deservedly awarded the Keith Kirkland award for his multicentre retrospective review on Robot assisted salvage node dissection to treat recurrences detected by PSMA PET.
Following these presentations, the YURO annual meeting once again heralded a complement of enthusiastic, innovative and clever minds from all Australian states, eager to pursue research opportunities through collaborative means. Joined this year by Prof. Henry Woo, the group was fortunate to receive his valuable insight and feedback regarding past success and future direction. The group solidified upcoming positions of leadership and highlighted new directions in educational, research and mentorship avenues for younger members.
The Gala Dinner is a stand out affair during each ASM and this year was no exception. Guests were provided with the unique opportunity to see Australia’s Parliament House from the inside. The night began with surprise operatic renditions of many well known classics in the spacious foyer of the Great Hall and culminated with a climactic performance of Nesson Dorma. Guests then enjoyed a delectable 3 course meal in identical fashion to a rare collection of political royalty including; Barack Obama, Prince William and the Duke and Duchess of Cambridge.
Twitter metrics tabulated from the conference via the #Usanz17 (courtesy of Symplur LLC)
The final day of proceedings saw once again provided an array of interesting and thought provoking topics. The clear highlight of the morning was the metaphorical prize fight between Mr Joseph Ischia and Dr Shankar Siva debating the roles of surgery and radiotherapy in Oligometastatic disease. Although these two went toe to toe over many rounds, the inevitable conclusion was understandably a draw. Although on PowerPoint slide pictures alone, Dr Siva’s extensive use of Star Wars based analogies won my vote.
Insight and introduction to the 71st USANZ ASM was then delivered and as a Melbournian my bias was admittedly hard to hide. Attendees received a taste of the excitement to come, with what is assured to be another blockbuster cast of national and international urologists led boldly by Convenor Mr Daniel Moon and Scientific Program Director Prof. Declan Murphy. I for one, eagerly anticipate the return of the ASM to out Nation’s culinary and cultural capitol and I’m sure guests in 2018 will be captivated by the world most liveable city!
It can be said with certainty that this years USANZ 70th ASM presented a scientific program as strong as ever within a fascinating and historical backdrop and complimented by a lively social atmosphere. This consensus of a highly successful meeting, I’m sure was shared by all.
I look forward to seeing you all next year and hope you are eagerly anticipating the ‘flat whites’.
Dr. Todd G Manning, Department of Surgery, Austin Health, Melbourne, and Young Urology Researchers Organisation (YURO), Australia. Twitter: @DocToddManning
The twitter-based international urology journal club @iurojc #urojc is back with a splash after a brief hiatus. For the March 2017 #urojc, a lively discussion takes the theme of pelvic node dissection (PLND) on radical prostatectomy (RP) reviewing a timely article by Nicola Fossati et al. The paper was made available open access courtesy of European Urology @EUplatinum.
Benefits and Harms of Different Extents of LND During Radical Prostatectomy for #ProstateCancer: A https://t.co/PxRbbUyQOM
— European Urology (@EUplatinum) February 13, 2017
A systematic review of the literature was performed including all comparative studies of both randomized and non randomized studies, with at least one experimental and one control arm. This summarised 66 studies including more than 250.000 patients with particular focus on different extents of pelvic lymphadenectomy as proposed by the European Association of Urology. Outcome measures studied included oncological features of biochemical recurrence, development of metastases, cancer-specific survival, and overall survival. Adverse events were covered under secondary outcomes, both intra- and postoperatively observed. Finally, quality of PLND was addressed in terms of total number of nodes and total number of positive nodes. Risk of bias was assessed for all studies judging on basis of specific confounders.
The journal club ran for 48 hours from Sunday 5th march. The central question addressed is balance of benefits and drawbacks of lymph node dissection. The corresponding author of the manuscript, Steven Joniau from the University Hospitals of Leuven, Belgium highlighted the role of lymph nodes in prostate cancer recurrence.
#urojc Remember: PCa recurrence often first in regional LN. So, why not remove at RP? @iurojc @ChapinMD @LoebStacy @EveraertsW @dr_coops pic.twitter.com/5GRKhjOJfl
— steven joniau (@joniau) March 6, 2017
However despite this idea, the benefit of PLND is heavily scrutinized from the start. Long term data from a single centre suggested limited benefit.
How do we reconcile what appears to be lack of therapeutic benefit & morbidity for ePLND and current guidelines? #urojc
— Urology JC #urojc (@iurojc) March 5, 2017
Depends on how much time you spend on it
JH population was "unique". Therapeutic benefit depends on the cohort being studied.
— Badar M. Mian, MD (@BadarMian1) March 5, 2017
If PSA bcf so high with N1 disease, has PLND really made a diff? How is management changed if N1 disease confirmed pathologically? #urojc
— Urology JC #urojc (@iurojc) March 6, 2017
However PLND has since earlier times been employed as a diagnostic tool, where an optimal template (presacral in addition to extended LND) may be optimal for staging and removal of lymph nodes.
Does need for accurate staging trump (NOT about that man
) therapeutic benefit for standard PLND versus ePLND?#urojc pic.twitter.com/6N3bjAoRS2
— Urology JC #urojc (@iurojc) March 5, 2017
Try to encourage in our MDT as node info is often can often fine tune further management after RP #urojc https://t.co/4fZQ2eEVkv
— Nick Brook (@nickbrookMD) March 5, 2017
#urojc But knowlegde gained by PLND may guide decisions regarding adj treatment (which may influence survival)
— steven joniau (@joniau) March 6, 2017
Prospective study shows 'less-than-eLND' insuficient for staging. eLND 94% accurate staging, but misses 24% pos LN compared to seLND pic.twitter.com/f1Fm26SPcp
— steven joniau (@joniau) March 6, 2017
Despite the current state of evidence, PLND is frequently mentioned in the various guidelines available for prostate cancer. However the exact situations when to employ them is questioned by some participants.
How do we reconcile what appears to be lack of therapeutic benefit & morbidity for ePLND and current guidelines? #urojc
— Urology JC #urojc (@iurojc) March 5, 2017
@iurojc @nickbrookMD #EAUGuidelines mention Briganti, MSKCC or Roach nomograms, NCCN doesn't recommend a particular nomogram #urojc pic.twitter.com/QAdE4PBsHa
— Stacy Loeb, MD (@LoebStacy) March 6, 2017
#urojc @joniau @ChapinMD @LoebStacy @dr_coops Makes sense for high risk tumours, but the EAU 5% guideline for PLND is overkill
— Wouter Everaerts (@EveraertsW) March 6, 2017
The various therapeutic options for lymph node metastases also coloured the discussion.
if we can figure out whether postop RT necessary in all N1, ePLND may help avoid unnecessary treatment in some. #urojc
— Brian F. Chapin (@ChapinMD) March 6, 2017
The discussion further continued to the important issue of morbidity, and the associated question of performing an extended PLND (ePLND).
Are we understating morbidity of ePLND? Do we leave these patient on a knifes edge for future lymphodema? (Eg future RT, infection)#urojc
— Urology JC #urojc (@iurojc) March 6, 2017
@joniau lymphoedema is major concern for QoL, especially after eLND+ adj RT,
Needs multiD management #urojc— Wouter Everaerts (@EveraertsW) March 6, 2017
the baby shouldn't be in the bath. PLND so clearly needs to be tested in a prospective trial. As for ePLND…
— Tim O'Brien (@tsoburol) March 6, 2017
What's your justification for doing an ePLND? Is it because of guideline recommendations?#urojc
— Urology JC #urojc (@iurojc) March 5, 2017
#urojc ePLND = mmmPLND, more morbidity,minutes,money. less BCR, doubt it.
— Alan Hay (@alanhaymd) March 5, 2017
@iurojc ePLND does nearly double my time for RALRP. Sometimes even longer then the prostatectomy. #urojc
— Brian F. Chapin (@ChapinMD) March 6, 2017
.@DrHWoo I don't follow–Some N+ men essntlly cured by only RP/PLND. I think it's therapeutic.
But I don't believe ePLND= improvemnt #urojc pic.twitter.com/EwSp4Im5VO— David Y.T. Chen (@dytcmd) March 6, 2017
Try to encourage in our MDT as node info is often can often fine tune further management after RP #urojc https://t.co/4fZQ2eEVkv
— Nick Brook (@nickbrookMD) March 5, 2017
#urojc But knowlegde gained by PLND may guide decisions regarding adj treatment (which may influence survival)
— steven joniau (@joniau) March 6, 2017
Prospective study shows 'less-than-eLND' insuficient for staging. eLND 94% accurate staging, but misses 24% pos LN compared to seLND pic.twitter.com/f1Fm26SPcp
— steven joniau (@joniau) March 6, 2017
Despite the current state of evidence, PLND is frequently mentioned in the various guidelines available for prostate cancer. However the exact situations when to employ them is questioned by some participants.
How do we reconcile what appears to be lack of therapeutic benefit & morbidity for ePLND and current guidelines? #urojc
— Urology JC #urojc (@iurojc) March 5, 2017
@iurojc NCCN guidelines recommend PLND for nomogram probability >=2% vs 5% threshold in #eauguidelines #urojc pic.twitter.com/7HYVSYUSJv
— Stacy Loeb, MD (@LoebStacy) March 6, 2017
@iurojc @nickbrookMD #EAUGuidelines mention Briganti, MSKCC or Roach nomograms, NCCN doesn't recommend a particular nomogram #urojc pic.twitter.com/QAdE4PBsHa
— Stacy Loeb, MD (@LoebStacy) March 6, 2017
#urojc @joniau @ChapinMD @LoebStacy @dr_coops Makes sense for high risk tumours, but the EAU 5% guideline for PLND is overkill
— Wouter Everaerts (@EveraertsW) March 6, 2017
The
if we can figure out whether postop RT necessary in all N1, ePLND may help avoid unnecessary treatment in some. #urojc
— Brian F. Chapin (@ChapinMD) March 6, 2017
The discussion further continued to the important issue of morbidity, and the associated question of performing an extended PLND (ePLND).
Are we understating morbidity of ePLND? Do we leave these patient on a knifes edge for future lymphodema? (Eg future RT, infection)#urojc
— Urology JC #urojc (@iurojc) March 6, 2017
@joniau lymphoedema is major concern for QoL, especially after eLND+ adj RT,
Needs multiD management #urojc— Wouter Everaerts (@EveraertsW) March 6, 2017
the baby shouldn't be in the bath. PLND so clearly needs to be tested in a prospective trial. As for ePLND…
— Tim O'Brien (@tsoburol) March 6, 2017
What's your justification for doing an ePLND? Is it because of guideline recommendations?#urojc
— Urology JC #urojc (@iurojc) March 5, 2017
#urojc ePLND = mmmPLND, more morbidity,minutes,money. less BCR, doubt it.
— Alan Hay (@alanhaymd) March 5, 2017
@iurojc ePLND does nearly double my time for RALRP. Sometimes even longer then the prostatectomy. #urojc
— Brian F. Chapin (@ChapinMD) March 6, 2017
.@DrHWoo I don't follow–Some N+ men essntlly cured by only RP/PLND. I think it's therapeutic.
But I don't believe ePLND= improvemnt #urojc pic.twitter.com/EwSp4Im5VO— David Y.T. Chen (@dytcmd) March 6, 2017
if we can figure out whether postop RT necessary in all N1, ePLND may help avoid unnecessary treatment in some. #urojc
— Brian F. Chapin (@ChapinMD) March 6, 2017
The increasing use of PSMA PET/CT provided other spread pattern data to be considered. And finally temporal changes in PSA testing is observed to affect the need for LND.
How might Ga68 PSMA PET/CT change the dynamic? Early data shows a lot of disease above the diaphragm. #urojc https://t.co/zyX9czHuwH
— Urology JC #urojc (@iurojc) March 6, 2017
Although, with PSMA PET/CT we're finding crazy spread patterns (e.g. Isolated supraclav nodal met) #urojc
— Matt Cooperberg (@dr_coops) March 6, 2017
I dunno… in 2017 I think it's a very rare pt who needs the RP and doesn't need the LND! #urojc @iurojc
— Matt Cooperberg (@dr_coops) March 6, 2017
#urojc @dr_coops @LoebStacy @iurojc the pt who "doesn't need PLND" probably often doesn't need RP either. Especially in PSA era
— David Y.T. Chen (@dytcmd) March 6, 2017
From the poll which ran during the discussion, about half responders would perform extended PLND for staging, while the rest were divided almost equally between therapeutic benefit and adherence to guideline recommendations.
Why do you do ePLND?#urojc
— Urology JC #urojc (@iurojc) March 5, 2017
Probably all participants of the discussion agrees for the need of a proper randomised study addressing role of PLND.
But "therapeutic benefits of PLND during radical prostatectomy remain unproven"@ChapinMD @LoebStacy @EveraertsW @dr_coops#urojc
— Henry Woo (@DrHWoo) March 6, 2017
At the end of a busy 48 hours, the discussion had been joined by top experts in the field of prostate cancer, generated more than 200 tweets and reached more than 700 thousand impressions the world over.
Special thanks to @EUplatinum for allowing open access for this month's paper. Special thanks to author @joniau for participating #urojc
— Urology JC #urojc (@iurojc) March 7, 2017
Yodi Soebadi (@yodisoebadi) is an Indonesian urologist, trained at Universitas Airlangga, currently pursuing doctoral research at KU Leuven in Belgium.