Video: Some like it safe
Preoperative JJ stent placement in ureteric and renal stone treatment: results from the Clinical Research Office of Endourological Society (CROES) ureteroscopy (URS) Global Study
Objective
To compare outcomes of ureteric and renal stone treatment with ureteroscopy (URS) in patients with or without the placement of a preoperative JJ stent.
Patients and Methods
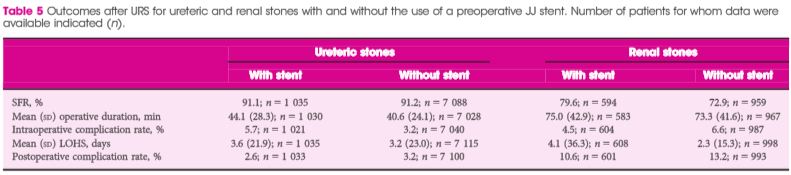
The Clinical Research Office of the Endourological Society (CROES) URS Global Study collected prospective data for 1 year on consecutive patients with ureteric or renal stones treated with URS at 114 centres around the world. Patients that had had preoperative JJ stent placement were compared with those that did not. Inverse-probability-weighted regression adjustment (IPWRA) was used to examine the effect of preoperative JJ stent placement on the stone-free rate (SFR), length of hospital stay (LOHS), operative duration, and complications (rate and severity).
Results
Of 8 189 patients with ureteric stones, there were 978 (11.9%) and 7 133 patients with and without a preoperative JJ stent, respectively. Of the 1 622 patients with renal stones, 590 (36.4%) had preoperative stenting and 1 002 did not. For renal stone treatment, preoperative stent placement increased the SFR and operative time, and there was a borderline significant decrease in intraoperative complications. For ureteric stone treatment, preoperative stent placement was associated with longer operative duration and decreased LOHS, but there was no difference in the SFR and complications. One major limitation of the study was that the reason for JJ stent placement was not identified preoperatively.
Conclusions
The placement of a preoperative JJ stent increases SFRs and decreases complications in patients with renal stones but not in those with ureteric stones.