
Editorial: The evolution of robotic cystectomy
A decade has passed since the publication of the first series of robot-assisted radical cystectomies in the BJUI by Menon et al. [1]. New technologies are fascinating, and many surgeons who aspire to leave a mark in history take the lead in pioneering new procedures. Others follow without waiting for any evidence to justify the adoption of new procedures. In this race, the opinion of the most important stakeholder, the patient, gets ignored.
Although their study has many methodological flaws, Guru et al. [2] have made the effort to collect data on patients’ health-related quality of life (HRQL) after robot-assisted radical cystectomy for bladder cancer. Radical cystectomy is a morbid procedure with a serious impact on patients’ HRQL, no matter how it is performed. Loosing an organ which is responsible for the storage and evacuation of urine several times a day and replacing it with alternatives of continent or incontinent diversion has a serious impact on quality of life, as is evident from this study.
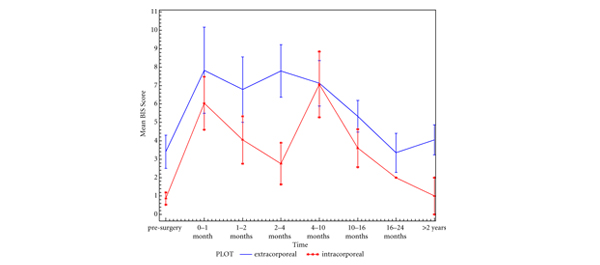
Robotic cystectomy is still evolving. With more experience, a few experts have ventured to perform intracorporeal reconstruction of the urinary diversion. While we await the long-term functional outcomes of this switch over in surgical approach, Guru et al. report the short-term HQRL outcomes in a series of 43 patients undergoing robot-assisted radical cystectomy and intracorporeal urinary diversion at their institution. Most patients (n = 38) had ileal conduit urinary diversion. The authors went on to compare the postoperative outcomes of this cohort with another group of 70 patients who only completed the questionnaire after having undergone robot-assisted radical cystectomy and extracorporeal urinary diversion.
It is interesting to note that there was no significant difference in HRQL between those undergoing extracorporeal and those undergoing intracorporeal reconstruction. These outcomes reinforce the need to gather robust scientific evidence from properly conducted multi-centre, multinational randomized trials before the introduction of new procedures, instead of evaluation with retrospective studies. The urological community has embraced new technologies and patients have benefited a great deal from these innovative approaches; however, it is incumbent upon us to develop a culture of independent, unbiased data collection on outcomes. In this regard we must make the HQRL one of the most important quality indicators in assessment of the new procedures. Such an approach will enable us to justify the extra cost which society has to bear for our innovative trends in the management of old problems [3].
Muhammad Shamim Khan
Guy’s and St Thomas’s Hospital and King’s College London, London, UK
References
- Menon M, Hemal AK, Tewari A et al. Nerve-sparing robot-assisted radical cystoprostatectomy and urinary diversion. BJU Int 2003; 92: 232–236
- Poch MA, Stegemann AP, Rehman S et al. Short-term patient reported health-related quality of life (HRQL) outcomes after robot-assisted radical cystectomy (RARC). BJU Int 2014; 113: 260–265
- Wang TT, Ahmed KA, Khan MS et al. Quality-of-care framework in urological cancers: where do we stand? BJU Int 2011; 109: 1436–1443

