Editorial: Renal functional recovery after radical nephrectomy
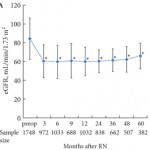
In their publication ‘Trends in renal function after radical nephrectomy: a multicentre analysis’, Chung et al. [1] suggest that after radical nephrectomy (RN), renal functional recovery in patients who have RCC occurs even in states of baseline renal functional compromise (pre-existing stage III chronic kidney disease, CKD). These findings bolster other recent reports, which suggest that surgically induced CKD may not be associated with the same degree of renal functional decline as CKD that may be caused by medical factors [2, 3]. While the incidence of de novo stage III CKD (36.1%) and delta estimated GFR between preoperative and postoperative values are lower than reported by most other groups, which may be attributable to national and demographic trends that are different from North American and European trends [2-4], the findings are nonetheless important and show that in the short-to-intermediate term (median follow up of 33 months) continued renal functional stabilisation and recovery occurs after RN. Also, performing a RN in a patient does not sentence him or her to invariable or inevitable renal functional decline in the short-to-intermediate term. Furthermore, they establish, in the short-to-intermediate term at least, a reasonable timeline of renal functional recovery for patient counselling and physician expectations in the postoperative follow-up period. Interestingly, and perhaps more disturbingly, the authors noted minimal and no functional recovery in the elderly and diabetic groups, underlying the importance for consideration of nephron-sparing approaches in these higher risk subgroups, even in the setting of normal renal function, and particularly with a lower risk lesion, e.g. a clinical T1a renal mass [5]. What we are missing from this analysis are longer term data, and a more thorough analysis of the incidence and impact of potential metabolic and cardiovascular sequelae during this period [4, 6], and a comparative analysis that examines the timeline of renal functional recovery after partial nephrectomy. Because of these reasons, the reader should be cautioned not to over-interpret these findings, and to conclude that because RN is associated with renal functional recovery, performing a RN may not pose increased long-term risk compared with a nephron-sparing method, particularly in a patient with pre-existing medical drivers towards CKD (diabetes, obesity, hyperlipidaemia, etc.). These findings are nonetheless important and provocative, and should spur further investigation and may provide an important adjunct in the counselling of patients about the functional impact of RN.
Ithaar H. Derweesh
Department of Urology, University of California San Diego Health System, La Jolla, CA, USA
References
- Chung JS, Son NH, Byun SS et al. Trends in renal function after radical nephrectomy: a multicentre analysis. BJU Int 2014; 113:408–415
- Van Poppel H, Da Pozzo L, Albrecht W et al. A prospective, randomised EORTC intergroup phase 3 study comparing the oncologic outcome of elective nephron-sparing surgery and radical nephrectomy for low-stage renal cell carcinoma. Eur Urol 2011; 59:543–552
- Lane BR, Campbell SC, Demirjian S, Fergany AF. Surgically induced chronic kidney disease may be associated with a lower risk of progression and mortality than medical chronic kidney disease. J Urol 2013; 189: 1649–1655
- Sun M, Bianchi M, Hansen J et al. Chronic kidney disease after nephrectomy in patients with small renal masses: a retrospective observational analysis. Eur Urol 2012; 62: 696–703
- Campbell SC, Novick AC, Belldegrun A et al. Guideline for management of the clinical T1 renal mass. J Urol 2009; 182:1271–1279
- Woldrich J, Mehrazin R, Bazzi WM et al. Comparison of rates and risk factors for development of anaemia and erythropoiesis-stimulating agent utilization after radical or partial nephrectomy. BJU Int 2012; 109: 1019–1025