Editorial: Equivalent outcomes for monopolar and bipolar TURP; but are we overlooking the potential for improvement in sexual function after surgery?
Both BPH and sexual function (SF) have a major impact on quality of life in older men. Sexual dysfunction is a complex process encompassing both erectile and ejaculatory dysfunction, as well as reduced libido and difficulty achieving orgasm. Whilst retrograde ejaculation is an almost inevitable consequence of TURP, the evidence that TURP causes erectile dysfunction is conflicting. This is probably attributable, at least in part, to a lack of high-quality historical data. Studies now show that LUTS is a risk factor for sexual dysfunction, and we are becoming increasingly aware of the relationship that exists between LUTS, depression and sexual dysfunction.
Given the favourable safety profile of bipolar TURP (b-TURP), it is perhaps a surprise that this latest study from Mamoukalis et al. has failed to demonstrate any difference in outcomes with regard to the deterioration in SF after surgery. The authors should be praised for their attempts to examine in fine detail (using the International Index of Erectile Function [IIEF]-15 in this case) any potential differences between b-TURP and monopolar TURP (m-TURP).
The design of the bipolar system is such that tissue is removed at a lower temperature and therefore the likelihood of damage to surrounding tissues and nerves is reduced. Several randomized trials have compared b-TURP with m-TURP, but only a small number have looked specifically at sexual variables in a randomized setting. This multicentre study by Mamoukalis et al. randomized 279 men to one of the two resection techniques, looking specifically at overall SF quantified by the IIEF-15. No differences were detected in any aspect of SF; erectile function (EF) improved in 26.4% of patients in the m-TURP group compared with 19.6% in the b-TURP group, and remained stable in 60.9 and 60.8% of patients, respectively. A deterioration in EF was apparent in 12.7% of the m-TURP group compared with 19.6% of the b-TURP group (P = 0.323). These results mirror those of a similar randomized study by Akman et al. comparing a quasi-bipolar system with m-TURP. They demonstrated equivalence for all measured variables except for operating time and a 1.4% incidence of TUR syndrome in the m-TURP group. In their study, the EF domain of the IIEF-15 was measured before and after surgery. EF worsened in 17% of men, improved in 28.2% and was unchanged in 54.8%. A comparative evaluation of EF was performed in a sub-group of 188 sexually active non-catheterized men of whom 18.2% developed de novo erectile dysfunction.
The explanation for the equivalent outcomes is unclear and further investigation is required. Does the failure of bipolar TURP to demonstrate a benefit with regard to SF leave the door open for the competing minimally invasive laser technologies? The overall impact of the holmium laser compared with that of TURP appears to be equivalent, with a mean of 7.5 and 7.7% of patients reporting decreased erectile function, and 7.1 and 6.2% of patients reporting increased function after each surgery. From the data available thus far, it would also appear that photoselective vaporization of the prostate similarly has no overall deleterious impact on SF when compared with TURP in a randomized trial. Further randomized data are pending and are of course of great importance if we are to understand better how the procedures we perform for symptomatic BPH affect our patients. As technological advances are made the hope is that the ‘damaging’ effects of BPH surgery on overall SF (particularly EF) will reduce further, but it may indeed be that we are searching for small margins when our attention might be better focused on maximizing the likelihood of a positive outcome, facilitated by considering the preoperative status (general health as well as urinary and sexual function), aided by the use of validated questionnaires. A better appreciation and understanding of the factors that may increase the risk of ED after surgery (age, diabetes, metabolic syndrome, obesity, cardiovascular disease and psychological factors) will enable us to manage expectations more effectively. A shorter hospital stay with minimal postoperative discomfort and an early return to normal activities, coupled with good symptomatic improvement in the longer term can only serve to be of benefit with regard to improving SF outcomes.
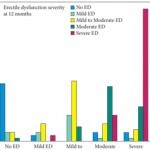
One recent study reporting both the short-, medium- and long-term effects of TURP on SF highlighted the high incidence of LUTS before treatment with 57% overall reporting ED before surgery. Those with severe LUTS were much more likely to have significant sexual dysfunction before surgery. This study also demonstrated a 15% improvement in pre-existing ED which was related to the improvement in LUTS after TURP.
On reflection, therefore, it would seem reasonable to conclude from the evidence presented that, although retrograde ejaculation frequently occurs after outflow surgery, erectile function is as likely to improve as it is to deteriorate. By focusing on the specific patient characteristics for each individual case before surgery it is possible we can improve the proportion of patients achieving a favourable outcome. When counselling patients before surgery regarding SF we should therefore remember to include the potential benefits as well as the risks. Furthermore, for those patients particularly anxious about the possibility of worsening SF, a ‘lesser’ surgical procedure, which might not achieve a transurethral resection-like cavity should perhaps be considered as a compromise. However, a surgical alternative which is not equivalent to TURP may indeed reduce the likelihood of improving erectile function, given the interrelationship that appears to exist between LUTS and SF.
Richard Hindley
Department of Urology, Hampshire Hospitals NHS Foundation Trust, Basingstoke, Hampshire, UK.