
Editorial: Better late than early for long-term survival in patients with recurrence after renal carcinoma
In this paper, Brookman-May et al. [1] used a large multi-institutional database of over 13 000 patients from 23 centres in both Europe and the USA to examine the prognostic indicators of cancer-specific survival (CSS) in patients who had recurrence after primary surgery for RCC. Their analysis was based on a subset of 1712 patients who had recurrence during a median follow-up period of 50 months. All patients had undergone either radical nephrectomy or nephron-sparing surgery, with no evidence of metastasis at the time of surgery.
The authors have previously shown, in a related study based on a subset of 5000 patients from the same database, that lymphovascular invasion, Fuhrman grade 3–4, and pT stage > pT1 at the time of diagnosis were significantly associated with the development of late recurrence (defined as after >5 years) [2]. In this paper, the primary objective was to look at the effect of time to tumour recurrence (TTR) on CSS. In addition, clinical and histopathological comparisons were made between patients with early (<5 years) and late recurrence (>5 years).
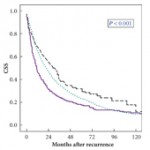
Patients often want to know whether if they are recurrence-free after a period of time, their subsequent risk of dying from recurrence is reduced; this paper goes some way towards answering this question and showing that those with later recurrence had improved survival times. Specifically, the authors found that TTR was an independent predictor of CSS; i.e. if patients recurred early they had a worse CSS than those recurring late. This is similar to results from another group who reported that recurrent disease, particularly before 12 months, was associated with a poorer prognosis [3]. In the first 4 years of follow-up, a shorter TTR independently predicted lower CSS after recurrence [1]. When divided into those with early recurrence, Group A (N = 1402), and those with late recurrence, Group B (N = 310), patients in Group A were more likely to be male, of advanced age, have a greater tumour diameter and stage, have Fuhrman grade 3–4, with lymphovascular invasion and positive lymph node disease, than those in Group B. Patients in Group A had a 3-year CSS of 30% compared with those in Group B whose CSS was better at 41%. Age and gender were also independent predictors of CSS.
These results can help to guide the aftercare management of patients after primary surgery. Currently, primary surgery is the only recommended option for patients with localized RCC, although results from several phase III clinical trials looking at the role of adjuvant therapy, such as the SORCE, PROTECT and S-TRAC trials, are still awaited [4]. Furthermore, it is not known which group of patients are suitable for adjuvant chemotherapy, which is reflected in the subtly differing eligibility criteria for recruitment to the various trials [4]. The authors of the present study pointed out that a method of risk stratification may be useful to allow equal representation of early and late recurrence patients in treatment arms for clinical trials. Potentially, understanding the predictors of early recurrence may help to identify patients for whom adjuvant therapy may be beneficial.
Only 12% of patients with localized RCC in the present cohort developed recurrence after surgery [1]. This rate is lower than that found in the literature, where 20–30% recurrence rates of localized RCC have been reported [2, 5, 6]. Brookman-May et al. speculate that this lower rate is attributable to both an increase in early detection as well as improved surgical management in recent years. Furthermore, they acknowledge that the database is heterogeneous and that the study therefore has all the inherent limitations of a retrospective study.
The present paper clearly shows that the earlier the recurrence after surgery the lower the survival rate, but a clear strategy for the surveillance of localized RCC after primary surgery is currently lacking. Most follow-up protocols exercise a blanket ‘one for all’ policy with follow-up spaced at regular intervals to ensure patients who recur are detected early. Such a policy may not be intensive enough to detect early recurrence in some patients and may be excessive for the majority of patients where the risk of recurrence is low. Risk stratification of patients, by understanding the predictors of CSS after surgery, may help to tailor surveillance protocols to the individual and identify those for whom adjuvant therapy may be beneficial.
Kathie Wong and Ben Challacombe
The Urology Centre, Guy’s Hospital, Guy’s and St Thomas’ NHS Foundation Trust, London, UK
References
- Brookman-May S, May M, Shariat S et al. Time to recurrence is a significant predictor of cancer-specific survival after recurrence in patients with recurrent renal cell carcinoma – results from a comprehensive multi centre database (CORONA/SATURN Project). BJU Int 2013; 112: 909–916
- Brookman-May S, May M, Shariat SF et al. Features associated with recurrence beyond 5 years after nephrectomy and nephron-sparing surgery for renal cell carcinoma: development and internal validation of a risk model (PRELANE score) to predict late recurrence based on a large multicenter database (CORONA/SATURN Project). Eur Urol 2012; 64: 472–477
- Rodriguez-Covarrubias F, Gomez-Alvarado MO, Sotomayor M et al. Time to recurrence after nephrectomy as a predictor of cancer-specific survival in localized clear-cell renal cell carcinoma. Urol Int 2011; 86: 47–52
- Kim SP, Crispen PL, Thompson RH et al. Assessment of the pathologic inclusion criteria from contemporary adjuvant clinical trials for predicting disease progression after nephrectomy for renal cell carcinoma. Cancer 2012; 118: 4412–4420
- Hollingsworth JM, Miller DC, Daignault S, Hollenbeck BK. Five-year survival after surgical treatment for kidney cancer: a population-based competing risk analysis. Cancer 2007; 109: 1763–1768
- Breda A, Konijeti R, Lam JS. Patterns of recurrence and surveillance strategies for renal cell carcinoma following surgical resection. Expert Rev Anticancer Ther 2007; 7: 847–862
We need more collaborative, multi-institutional datasets such as the one presented here. Is there an ideal nomogram to predict who to followup and how??