Editorial: The metabolic syndrome and the prostate
The metabolic syndrome has been known for ~80 years 1 and is important to both urologists and their patients because of a two‐fold increase in the relative risk of atherosclerotic cardiovascular disease‐related events and a five‐fold increase for developing Type 2 diabetes as compared to people without the syndrome. Abdominal obesity is well known to be an important underlying risk factor for precipitating the syndrome and obesity is also known to markedly increase the risk for developing BPH and its symptoms 2. There are other associations that may be relevant here including an association between a lack of physical activity and the severity of LUTS 3, and a close correlation between the degree of prostatic and systemic inflammation and the degree of LUTS 4. Systemic inflammation is implicated in the metabolic syndrome with pro‐inflammatory cytokines due to the adipose tissue load, such as C‐reactive protein, tumour necrosis factor α and interleukin 6, being involved in causing the insulin resistance, which is a diagnostic feature of this condition 5.
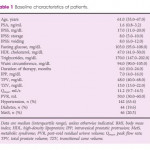
The current study connects the metabolic syndrome with an anatomical feature of benign prostatic enlargement (BPE), namely intravesical prostatic protrusion (IPP) 6. Each of the diagnostic features of metabolic syndrome was examined separately such as reduced high‐density lipoprotein (HDL)‐cholesterol and raised triglycerides. Hypertriglyceridaemia is due to an overproduction of very‐low‐density lipoprotein (VLDL) by the liver and a reduction of lipoprotein lipase in peripheral tissues, and reflects the insulin resistant condition responsible for the metabolic syndrome 5. In this study, high triglyceride levels were an independent predictor of a total prostatic volume (TPV) of >40 mL. The other major lipoprotein abnormality in metabolic syndrome is a reduction in HDL‐cholesterol levels, which is due to both a decrease in the cholesterol content of this lipoprotein and an increase in its clearance from the circulation. In this study by Russo et al. 6, HDL levels were negatively associated with IPP and both total and transition zone volumes, and they postulate that these associations may be mediated by the effect of dyslipidaemia on prostate cells and prostatic inflammation.
Hypertension is another diagnostic feature that the authors address. There is increased renal sodium reabsorption, increased activity of the sympathetic nervous system, and vasoconstriction related to an increase in fatty acids in this syndrome. Hypertension, defined as systolic ≥135 mmHg, diastolic ≥85 mmHg or on current treatment, was positively associated with IPP and also associated with a TPV of ≥40 mL and a transitional zone volume of ≥20 mL in this study 6. Waist circumference and fasting glucose were not as strongly related to the features of BPH but ultimately are key drivers of the metabolic syndrome and management of these features is a cornerstone of the management of the whole condition.
Lifestyle and dietary interventions can address many of the aspects of this insulin‐resistant state with medical management of the metabolic features being used to supplement these. The same interventions are also successful in decreasing LUTS 3, which should not be surprising given the above. The longstanding aphorism that ‘heart healthy is prostate healthy’ appears to not only apply to the treatment of prostate cancer but also to that of BPH and urologists remain in an important position to identify men at significant risk.
- 1 Alberti KG, Zimmet P, Shaw J, IDF Epidemiology Task Force Consensus Group. The metabolic syndrome–a new worldwide definition. Lancet 2005; 366: 1059–62
- 2 Parsons JK, Sarma AV, McVary K, Wei JT. Obesity and benign prostatic hyperplasia: clinical connections, emerging etiological paradigms and future directions. J Urol 2013; 189 (Suppl.): S102–6.
- 3 Fowke JH, Phillips S, Koyama T et al. Association between physical activity, lower urinary tract symptoms (LUTS) and prostate volume. BJU Int 2013; 111: 122–8
- 4 Burris MB, Cathro HP, Kowalik CG et al. Lower urinary tract symptom improvement after radical prostatectomy correlates with degree of prostatic inflammation. Urology 2014; 83: 186–90
- 5 Eckel RH, Grundy SM, Zimmet PZ. The metabolic syndrome. Lancet 2005; 365: 1415–28
- 6 Russo GI, Regis F, Spatafora P et al. Association between metabolic syndrome and intravesical prostatic protrusion in patients with benign prostatic enlargement and lower urinary tract symptoms (MIPS Study). BJU Int 2018; 121: 799–804.