Editorial: Cutaneous Ureterostomy: ‘Back to the Future’
An increasingly ageing and frail population undergoing cystectomy and urinary diversion has rekindled interest in urinary diversions with a lower risk of peri-operative complications, such as cutaneous ureterostomy (CU).
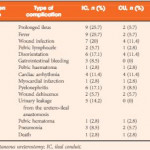
The study in this issue of BJUI by Longo et al. [1] compares complications and quality of life in elderly patients with high comorbidities (American Society of Anesthesiologists [ASA] physical status score 3–4 and Charlson Comorbidity Index [CCI] ~5) receiving either an ileal conduit (IC) or a CU with a single stoma. Although the IC group had longer surgery, greater intra-operative blood loss, a higher number of patients needing intensive care monitoring, a longer time to drain removal and a longer hospital stay, as well as a higher number of intra- and early postoperative complications, the intensive care unit length of stay and quality of life did not differ.
Complication rates are high for cystectomy and urinary diversion, especially in the frail elderly population with comorbidities [2]. Most studies are retrospective and the reported complication rates differ largely. Few centres have compared IC with CU and, probably as a result of selection biases, the results vary [3, 4]. Obvious advantages of CU are the reduced length of surgery and the lack of a bowel anastomosis, and peritoneal lesions can be minimized or omitted, thus reducing the risk of postoperative ileus (POI), a common complication after urinary diversion. These advantages were confirmed in the present study, with prolonged POI observed in 25.7% in the IC group vs 5.7% in the CU group and the duration of surgery being 226 min in the IC group vs 150 min in the CU group. Interestingly, there was no difference in major complications classified as Clavien–Dindo grades III–IV, with the exception of urinary leakage from the uretero-ileal anastomosis (14.2%).
Somewhat surprisingly, 42.8% of patients with IC required a blood transfusion compared with 17.1% with UC. The main blood loss usually takes place during cystectomy, whereas blood loss during urinary diversion is minimal [5]. The authors explain this through bleeding from the mesenteric vessels associated with isolating a bowel segment for IC, an occurrence not commonly observed in our experience or in other published reports. Overall the transfusion rate seems high, but this is highly dependent on the preoperative haemoglobin level/anaemia and the haemoglobin level set for transfusion, which differs between centres.
One of the main problems with CU is ureteric obstruction, especially of the left ureter. The rationale behind this is the more extensive mobilization of the left ureter to enable its transfer to the right side, which can result in ischaemic lesions of the distal ureter. Stenosis and kinking of the ureters when passing through the abdominal wall can also lead to obstruction. For these reasons, many patients have long-term ureteric stents. In the present study, the ureteric stents were changed every month. Foreign bodies in the urinary tract can cause problems such as upper urinary tract infections, stent encrustation and nephrolithiasis [3]. To reduce these problems, meticulous care of the CU and frequent changes of the silicone JJ stent with antibiotic prophylaxis are generally recommended. A cost assessment would be of interest to determine the long-term cost of regular stent changes compared with the management of a higher rate of peri-operative complications in patients receiving an IC. Tubeless approaches have been described, and one study reported less ureteric obstruction with deferred stent removal after surgery [6].
The Bladder Cancer Index score as a measure of quality of life did not differ between groups. Quality of life questionnaires assessing urinary diversion have inherent problems. When comparing leakage (frequency of leakage) and control (amount of leakage) in a patient with an IC or a CU, it is not surprising that there is no difference. However, the need for regular hospital visits to change the stents, which can be bothersome for patients, especially the frail and dependent elderly or those with problems travelling, because of the need to transport the necessary aides (stoma bags, pads, catheters), are rarely addressed in questionnaires.
Cutaneous ureterostomy, which is being rediscovered, belongs in the armamentarium of every surgeon performing cystectomy. However, each type of urinary diversion has its pros and cons, and careful selection is necessary to balance benefits against risks in an effort to offer the best individual option to the older and frail patient.