What’s the Diagnosis?
Test yourself against our experts with our weekly quiz. You can type your answers here if you want to compare with our answers.
This image is taken from a recent BJUI paper (Bach et al, BJUI 2014).
No such quiz/survey/poll
Test yourself against our experts with our weekly quiz. You can type your answers here if you want to compare with our answers.
This image is taken from a recent BJUI paper (Bach et al, BJUI 2014).
No such quiz/survey/poll
Every Month the Editor-in-Chief selects the Article of the Month from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Month heading on the homepage will consist of additional material or media. This week we feature a video from Dr. Wouter Everaerts, discussing his paper.
If you only have time to read one article this week, it should be this one.
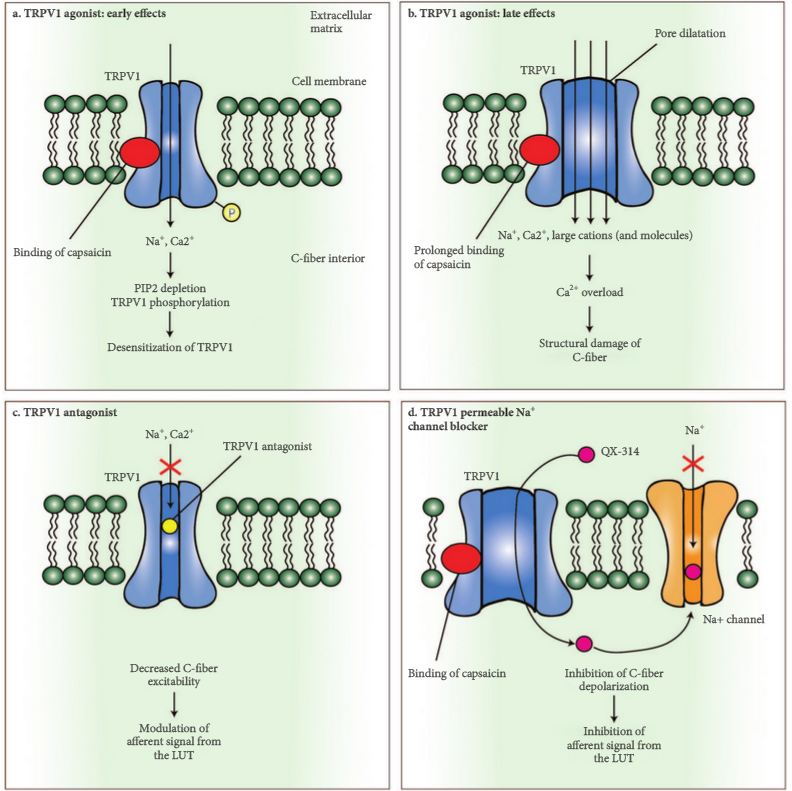
Transient receptor potential (TRP) channels belong to the most intensely pursued drug targets of the last decade. These ion channels are considered promising targets for the treatment of pain, hypersensitivity disorders and lower urinary tract symptoms (LUTS). The aim of the present review is to discuss to what extent TRP channels have adhered to their promise as new pharmacological targets in the lower urinary tract (LUT) and to outline the challenges that lie ahead.
Seventeen years have elapsed since the capsaicin receptor was first cloned by Caterina et al. [1] and the excellent review with an unusual provocative title by Deruyver et al. [2] was written. The capsaicin channel, re-named transient receptor potential (TRP) vanilloid receptor subtype 1 (TRPV1), is now commonly referred to as the founding member of the TRP family, as it currently includes 28 related channels, a number difficult to foresee in those early years [3].
TRP channels have been extensively studied in the lower urinary tract (LUT) with the aim of clarifying their role in micturition control and in the generation of LUTS. It is well accepted that TRP receptors have neuronal and non-neuronal expression [3, 4]. TRPV1 is fundamental to bladder hyperactivity and pain associated with LUT inflammation [3], while TRPV4 may participate in the generation of the normal sensation to void [5]. Another group of TRP receptors may even participate in bladder oncogenesis, which seems to be a role of TRPV2 [3]. The main substance of all this information is not a myth; rather it represents a large body of very solid scientific data.
There are certainly still many obscure areas. The distribution of TRP receptors in the bladder is certainly one of them. However, I disagree that a substantial part of available technical and financial resources have been allocated to study this matter. One should not forget that other matters, like the role of many TRP channels for bladder function, remain elusive. Broadly speaking, in my opinion, future key studies should tackle three very relevant but still unclear points. The importance of most TRP channels for bladder function is difficult to predict at the moment [3]. Just as an example, TRPA1 and TRPM8, which are sensitive to cold temperatures, are expressed in the bladder. However, the bladder, as all internal organs, is conserved at very constant physiological temperatures, making it difficult to understand the relevance of cold receptors to its function. Then, we need to find what the endogenous agonists for TRP receptors are in the LUT. Anandamide has been largely explored as an endogenous agonist for TRPV1 in the bladder [6], a fruitful observation as drugs able to manipulate endogenous levels of anandamide are currently being explored in clinical trials. The same holds true for the other members of the TRP family. TRPA1 may respond to infections due to its capacity to react to hydrogen sulphide [3]. But for the large majority of the TRP family endogenous agonists remain unknown. Finally, TRP antagonists that are simultaneously effective and safe must be generated. Most available TRPV1 antagonists, produced to date, although able to control bladder dysfunction in models of cystitis and spinal cord injury [3], cause hyperthermia and have been associated with an enlargement of ischaemic areas of the heart after coronary artery obstruction [3]. TRPV4 antagonists look very promising for controlling frequency but a compound safe for human use is still eagerly awaited [2]. Eventually the combination of antagonists for more than one of these receptors may prove effective at very low doses, so low that they do not generate serious adverse effects [7].
In conclusion, TRP receptors are a reality that still needs an enormous amount of work and dedication before becoming therapeutically useful. And that may take more time than we anticipate at the moment.
Transient receptor potential (TRP) channels belong to the most intensely pursued drug targets of the last decade. These ion channels are considered promising targets for the treatment of pain, hypersensitivity disorders and lower urinary tract symptoms (LUTS). The aim of the present review is to discuss to what extent TRP channels have adhered to their promise as new pharmacological targets in the lower urinary tract (LUT) and to outline the challenges that lie ahead.
Test yourself against our experts with our weekly quiz. You can type your answers here if you want to compare with our answers.
This image is taken from a recent BJUI paper (Huang et al BJUI 2015).
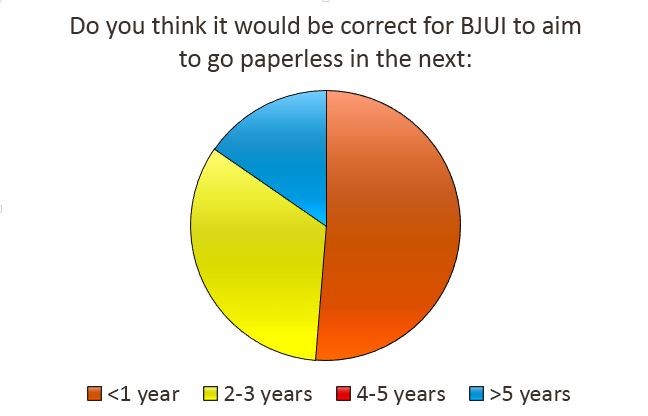
No such quiz/survey/pollThe current BCG shortage, and the effect this is having on our bladder cancer patients, is an issue that continues to weigh heavily on many urologists. With no immediate solution in sight, and limited availability, a variety of tactics are being advocated to optimally use the current supply.
The April 2015 International Urology Journal Club #urojc debate focused on the timely paper by Martínez-Piñeiro et al1. This paper reported the results of a randomised trial evaluating the outcomes of BCG induction followed by a modified three year maintenance regimen versus standard BCG induction alone in patients with high-risk non-muscle-invasive bladder cancer. The investigators concluded there was no observed decrease in recurrence and progression rates in those receiving just induction compared to induction and maintenance regimen.
This very topical debate kicked off on Sunday 12th April.
Coinciding with the USANZ Annual Scientific Meeting, this month’s debate gave both those who were live tweeting at the conference, and those learning about the benefits of social media as a new concept, the opportunity to see the #urojc debate in action.
One of the first points of discussion raised was the difference between the maintenance protocol used in the study, consisting of one BCG installation every three months for three years, and the standard SWOG schedule.
The lack of difference in outcome between the two groups raised the question as to whether this indicated that their modified maintenance protocol is less effective that the current strategies.
The theme of alternative maintenance schedules continued, with some variation in practice noted.
Some of the variability in maintenance may be due to the tolerability and side effects experienced.
Although there may be a degree of acceptance amongst patients if there is thought to be a chance of improvement in risks of disease recurrence or progression.
The reason for the variability of response to BCG therapy between patients remains unclear.
For the patient, the lack of understanding of why this is the case may be a cause of distress, especially when faced with adverse effects and toxicity.
Inevitably it was not long until the key on-going issue of the lack of available BCG was raised.
This issue continues to cause a lot of angst for both patients and their treating urologists, with no immediate solution evident. There may however be light at the end of a somewhat long tunnel with the restarting of production by Sanofi.
In the mean time, the downstream effects of the production delay continues to compromise the treatment options for bladder cancer patients.
As the availability remains largely outside of clinicians’ hands, perhaps our focus at present needs to be on other factors we can control in order to improve the outcomes for our bladder cancer patients.
This debate surrounding this paper has raised a number of key points that, in the face of the BCG shortage, are worth considering. Until the supply is re-established, the BCG we have needs to be optimally used – however perhaps the most effective maintenance schedule needs further investigation. Or perhaps, due to the variation in tolerability and effectiveness between individuals, maintenance therapy needs to remain a more fluid concept.
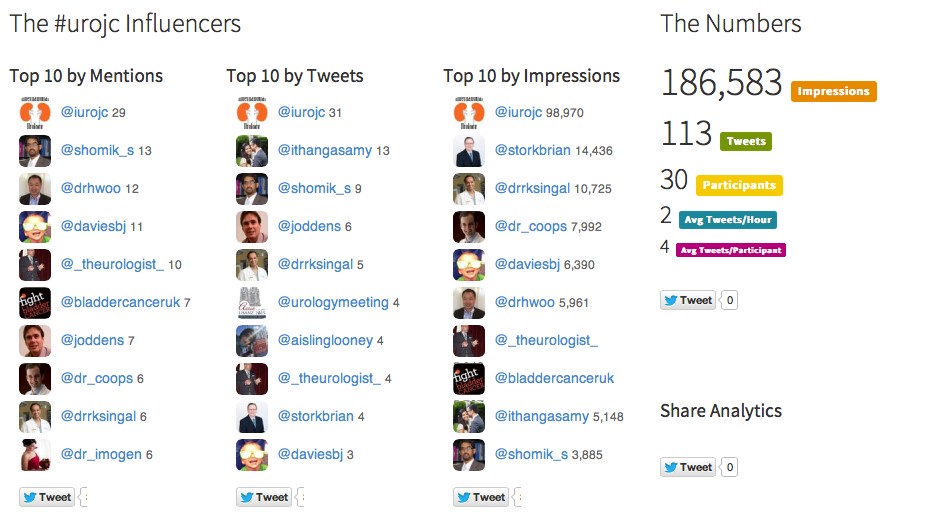
As always, the #urojc debate involved healthy international discussions. This gives the unique ability to understand the global viewpoints on the study findings, and the current BCG crisis. Analytics of the debate using the #urojc hash tag from the website www.symplur.com again demonstrated the excellent involvement from participants, with over 180,000 unique impressions.
Thanks to all of those who participated this month. We look forward to the #urojc May debate – I am sure it will be as lively as ever.
1. Martínez-Piñeiro L, Portillo JA, Fernández JM, et al. Maintenance Therapy with 3-monthly Bacillus Calmette-Guérin for 3 Years is Not Superior to Standard Induction Therapy in High-risk Non-muscle-invasive Urothelial Bladder Carcinoma: Final Results of Randomised CUETO Study 98013. European Urology March 2015 (Article In Press)
Every week the Editor-in-Chief selects the Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
To investigate whether poor preoperative cardiopulmonary reserve and comorbid state dictate high-risk status and can predict complications in patients undergoing radical cystectomy (RC).
In all, 105 consecutive patients with transitional cell carcinoma (TCC; stage T1–T3) undergoing robot-assisted (38 patients) or open (67) RC in a single UK centre underwent preoperative cardiopulmonary exercise testing (CPET). Prospective primary outcome variables were all-cause complications and postoperative length of stay (LOS). Binary logistic regression analysis identified potential predictive factor(s) and the predictive accuracy of CPET for all-cause complications was examined using receiver operator characteristic (ROC) curve analysis. Correlations analysis employed Spearman’s rank correlation and group comparison, the Mann–Whitney U-test and Fisher’s exact test. Any relationships were confirmed using the Mantel–Haenszel common odds ratio estimate, Kaplan–Meier analysis and the chi-squared test.
The anaerobic threshold (AT) was negatively (r = −206, P = 0.035), and the ventilatory equivalent for carbon dioxide (VE/VCO2) positively (r = 0.324, P = 0.001) correlated with complications and LOS. Logistic regression analysis identified low AT (<11 mL/kg/min), high VE/VC02 (≥33) and hypertension as significant factors, such that, in their presence patients were 5.55-times more likely to have complications at 90 days postoperatively [P = 0.001, 95% confidence interval (CI) 2.2–13.9]. ROC analysis showed a high significance (area under the curve 0.78, 95% CI 0.69–0.87; P < 0.001). In addition, based on CPET criteria >50% of patients presenting for RC had significant heart failure, whereas preoperatively only very few (2%) had this diagnosis. Analysis using the Mann–Whitney test showed that a VE/VCO2 ≥33 was the most significant determinant of LOS (P = 0.004). Kaplan–Meier analysis showed that patients in this group had an additional median LOS of 4 days (P = 0.008). Finally, patients with an American Society of Anesthesiologists grade of 3 (ASA 3) and those on long-term β-blocker therapy were found to be at particular risk of myocardial infarction (MI) and death after RC with odds ratios of 4.0 (95% CI 1.05–15.2; P = 0.042) and 6.3 (95% CI 1.60–24.8; P = 0.008).
Patients with poor cardiopulmonary reserve and hypertension are at higher risk of postoperative complications and have increased LOS after RC. Heart failure is known to be a significant determinant of perioperative death and is significantly under diagnosed in this patient group.
In this month’s issue of BJUI, Tolchard et al. [1] describe their experience with the use of cardiopulmonary exercise testing (CPET) in patients undergoing radical cystectomy. In particular, they assess the value of cardiopulmonary reserve in predicting complications and the length of stay in hospital after surgery.
The origin of CPET is in non-surgical specialties for the further investigation of patients with cardiac failure or unexplained breathlessness [2], but it subsequently gained utility in surgical fields, including the preoperative assessment of patients undergoing cardiac surgery [3].
In more recent times, it has been increasingly adopted within ‘high-risk’ preoperative assessment clinics for those patients undergoing a wide range of major elective, non-cardiac surgery; however, this enthusiastic uptake has often preceded more formal validation of the test’s ability to perform reliably in these new patient groups and their associated surgical procedures. The Bristol group [1] has therefore prospectively studied the role of CPET in 105 patients undergoing either robot-assisted or open radical cystectomy for TCC, using all-cause complications and length of stay as the primary outcome variables.
The researchers found that anaerobic threshold (AT), ventilatory equivalent for carbon dioxide (VE/VCO2) and hypertension were independent predictors of postoperative complications. Using the criteria chosen by Older et al. [4] of an AT ≤ 11 mL/kg/min and or VE/VECO2 ≥ 33, it was possible to define a high- and low-risk group. The high-risk group were 5.5 times more likely to experience a complication at 90 days compared with the low-risk group and, notably, all deaths and myocardial infarctions occurred in the high-risk group. As expected, they found that complications prolonged length of stay. Additionally, falling AT and or rising VE/VECO2 also correlated with increasing length of stay. Their study therefore suggests that CPET may have a role in the preoperative risk stratification of patients undergoing radical cystectomy by an open or robot-assisted approach.
The authors acknowledge that the cohort size is small and from a single institution, thereby necessitating further validation work across multiple centres, as well as subgroup analysis of differing surgical approaches. Interestingly, their study excluded patients who had received neoadjuvant chemotherapy; for many UK cancer centres, this would exclude ∼70% of patients undergoing radical cystectomy. It would clearly be important in future studies to understand how CPET metrics perform in this wider cohort, where anaemia and impaired performance status are known to be more common.
On the assumption that further studies may validate the use of CPET as a preoperative risk-stratifying tool, the pertinent question is how do we translate this research finding into patient benefit? Interventions such as preoperative patient optimization, pre-habilitation exercise regimes or the planned escalation of postoperative care may confer benefits but, as yet, we do not know if they attenuate the increased risk of complications or the prolonged inpatient stay.
As further evaluation of CPET takes place, we should remain cautious about its use as a ‘rule-out’ investigation in those patients otherwise considered eligible for radical surgical treatment. To date, there have been no formal evaluations of patients’ quality of life or end-of-life care in ‘non-operated’ cases. Poor local control of pelvic malignancy remains one of the most challenging aspects of care for uro-oncologists and, at times, it may even outweigh the impact of postoperative surgical complications. Due consideration must be given to this aspect when advising individual patients about the predicted risks and benefits of therapeutic treatment options. The decision to operate should clearly be informed by the preoperative assessment, but it is imperative that it continues to involve the patient’s wider multidisciplinary team, whose responsibility it will be to provide lifelong care.
In conclusion, CPET offers an interesting opportunity to identify those patients at greatest risk of adverse outcomes after radical cystectomy; however, the full benefits will not be realized if it is simply the ‘bearer of bad news’. The key to its success will be the identification of modifiable behaviours, by both the patient and the clinical team, that lead to improved patient-related outcomes. These outcomes should not be restricted to overall or cancer-specific survival but also measures of return to good health and prior performance status. Such longer-term outcome data may then help us to more accurately delineate the point at which the risks of a surgical treatment can be confidently predicted to outweigh the alternative of non-operative care for individual patients.
Test yourself against our experts with our weekly quiz. You can type your answers here if you want to compare with our answers.
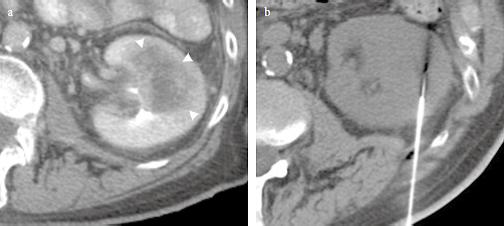
This image is taken from a recent BJUI paper (Brousil et al. 2015).
No such quiz/survey/poll