What’s the Diagnosis?
Test yourself against our experts with our weekly quiz. You can type your answers here if you want to compare with our answers.
This image is taken from Abel et al. (BJUI 2014)
No such quiz/survey/poll
Test yourself against our experts with our weekly quiz. You can type your answers here if you want to compare with our answers.
This image is taken from Abel et al. (BJUI 2014)
No such quiz/survey/pollEvery Week the Editor-in-Chief selects the Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video from Dr. Franklin Emmanuel Kuehhas, discussing his paper.
If you only have time to read one article this week, it should be this one.
To compare patient-reported outcomes (PROs) of surgical correction of Peyronie’s disease (PD) with the Nesbit procedure, plaque incision and grafting, and the insertion of a malleable penile implant after surgical correction of penile curvature.
We performed a retrospective review of men who underwent surgical correction of PD between January 2010 and December 2012 at six international centres. Treatment-related PROs and satisfaction were evaluated with a non-validated questionnaire.
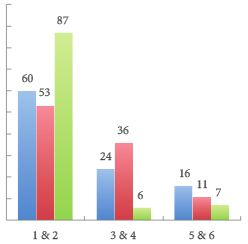
The response rate to the questionnaire was 70.9%, resulting in a study cohort of 206 patients. The Nesbit procedure, plaque incision with grafting, or implantation of a malleable penile prosthesis was performed in 50, 48, and 108 patients, respectively. Overall, 79.1% reported a subjective loss of penile length due to PD preoperatively (range 2.1–3.2 cm). Those patients treated with a malleable penile implant reported the greatest subjective penile length loss, due to PD. A subjective loss of penile length of >2.5 cm resulted in reduced preoperative sex ability. Postoperatively, 78.0%, 29.2% and 24.1% patients in the Nesbit, grafting, and implant groups reported a postoperative, subjective loss of penile length (range 0.4–1.2 cm), with 86.3%, 78.6%, and 82.1% of the patients in each group, respectively, being bothered by the loss of length.
Penile length loss due to PD affects most patients. Further penile length loss due to the surgical correction leads to bother among the affected patients, irrespective of the magnitude of the loss. The Nesbit procedure was associated with the highest losses in penile length. In patients with PD and severe erectile dysfunction, a concomitant lengthening procedure may be offered to patients to help overcome the psychological burden caused by the loss of penile length.
Peyronie’s disease (PD) is an acquired benign connective tissue disorder of the tunica albuginea of the penis that leads to the formation of fibrous inelastic plaques. As a result of pain, worsening quality of erections, penile shortening and deformity, the quality of life of both the patient and their partner may be significantly affected, and this may lead to depression, low self-esteem and relationship difficulties [1].
At present, surgery represents the ‘gold standard’ treatment when PD is stable, and should be offered to guarantee a penis straight and rigid enough to allow penetrative intercourse.
The flow chart in the 2010 guidelines on PD indicates the type of surgery that should be offered according to the preoperative quality of the erection, degree of deformity and penile length, but patient perception of preoperative penile shortening is not taken into consideration [2]. Penile shortening does play an important part, however, with regard to postoperative patient satisfaction, as confirmed by Akin-Olugbade et al. [3], whose series of patients with PD reported the lowest satisfaction rates after penile prosthesis implantation.
According to the present series by Kueronya et al. [4], in which patient-perceived pre- and postoperative penile length loss in patients with PD was evaluated, 79.1% of patients perceived a degree of length loss attributable to PD, and a subjective loss of length of >2.5 cm translated into reduced ability with regard to sexual intercourse. In particular, patients who underwent penile prosthesis implantation reported more significant perceived shortening. This is not surprising, as patients with larger plaques, more severe forms of PD and fibrosis are more likely to have erectile dysfunction and ultimately to require a penile prosthesis implantation. Among patients who did not undergo penile prosthesis implantation, those requiring Nesbit plication reported less preoperative shortening than those requiring plaque incision and grafting, as the latter group presented with more severe deformities.
Further penile length loss caused by the surgical correction leads to bother to the patients, irrespective of the magnitude of the loss. The message from the present series by Kueronya et al. is that, to achieve higher postoperative satisfaction rates in this unfortunate cohort of patients, the choice of the type of surgery should take into consideration patient’s perceived preoperative penile shortening and not be based solely on the 2010 PD guidelines algorithm, because ultimately patients wish to obtain full restoration of the shape and size of penis they had before the onset of PD [2].
As patient’s perceived penile length plays such an important role in a patient’s postoperative satisfaction and because patients undergoing penile prosthesis implantation are those who have lost more length, length restoration should be offered simultaneously with penile prosthesis implantation [5, 6].
Kueronya et al. should be congratulated for their work, which is the first series evaluating patient’s perceived penile shortening and may represent a significant step towards the restoration of an adequate sex life in patients with PD.
To compare patient-reported outcomes (PROs) of surgical correction of Peyronie’s disease (PD) with the Nesbit procedure, plaque incision and grafting, and the insertion of a malleable penile implant after surgical correction of penile curvature.
We performed a retrospective review of men who underwent surgical correction of PD between January 2010 and December 2012 at six international centres. Treatment-related PROs and satisfaction were evaluated with a non-validated questionnaire.
The response rate to the questionnaire was 70.9%, resulting in a study cohort of 206 patients. The Nesbit procedure, plaque incision with grafting, or implantation of a malleable penile prosthesis was performed in 50, 48, and 108 patients, respectively. Overall, 79.1% reported a subjective loss of penile length due to PD preoperatively (range 2.1–3.2 cm). Those patients treated with a malleable penile implant reported the greatest subjective penile length loss, due to PD. A subjective loss of penile length of >2.5 cm resulted in reduced preoperative sex ability. Postoperatively, 78.0%, 29.2% and 24.1% patients in the Nesbit, grafting, and implant groups reported a postoperative, subjective loss of penile length (range 0.4–1.2 cm), with 86.3%, 78.6%, and 82.1% of the patients in each group, respectively, being bothered by the loss of length.
Penile length loss due to PD affects most patients. Further penile length loss due to the surgical correction leads to bother among the affected patients, irrespective of the magnitude of the loss. The Nesbit procedure was associated with the highest losses in penile length. In patients with PD and severe erectile dysfunction, a concomitant lengthening procedure may be offered to patients to help overcome the psychological burden caused by the loss of penile length.
For those pop enthusiasts amongst you, “The drugs don’t work” – the year was 1997; The band: The Verve. For those more urologically minded, you will immediately be thinking of the recent publication in the Lancet reporting on the use of tamsulosin and nifedipine vs. placebo for the medical expulsive therapy (MET) of ureteric stones. Current national (BAUS) and international (EAU guidelines) recommend the use of MET, usually with an alpha blocker – and often tamsulosin, and it has certainly become common practice in most Emergency and urology departments certainly across the UK and likely worldwide.
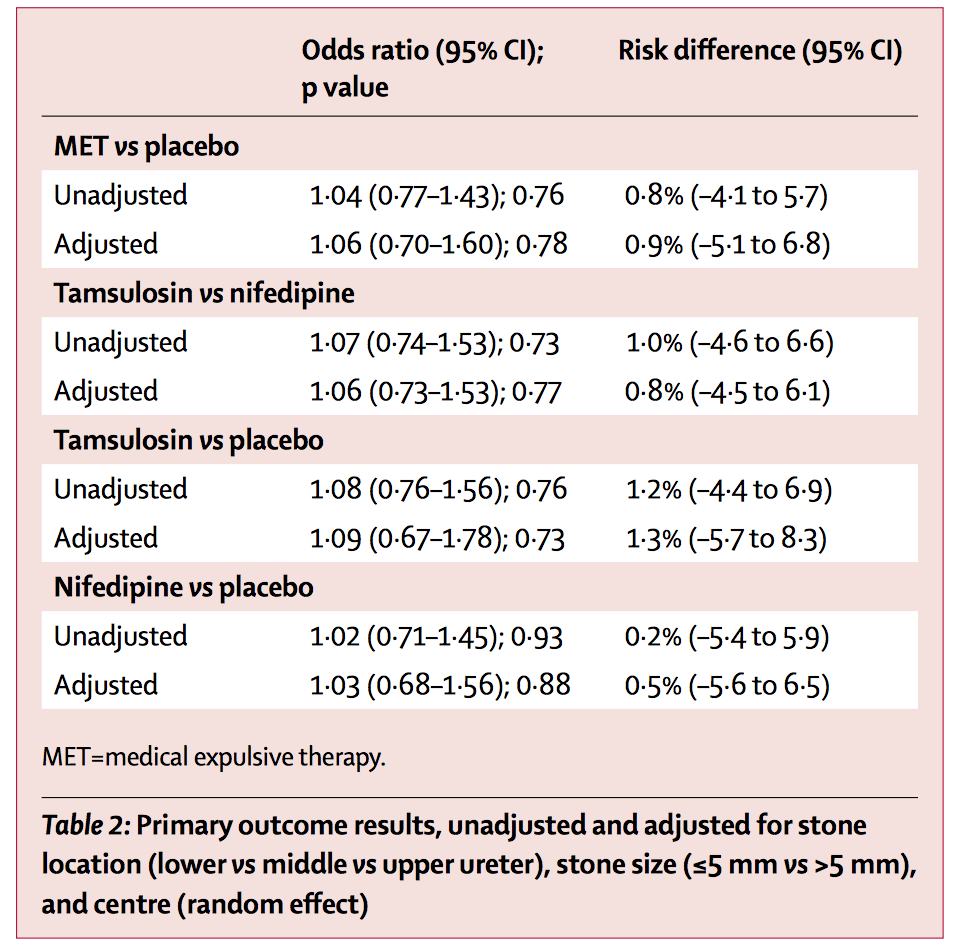
There have however always been doubts regarding the use of these with many small heterogenous studies with variable inclusion/exclusion criteria, various blinding protocols and suspicion of publication bias when only positive trials get published. Regardless, the clear outcome from the Hollingsworth meta-analysis was that both alpha blockers and calcium channel blockers are effective for helping stone passage and so they crept into routine clinical use. This trial should change all of that with headline results:
Aren’t those all the reasons we prescribe them? The first question of course is whether this trial is accurate. It certainly is a large trial with 1167 patients, randomised to the three double-blind arms in 24 centres in the UK. The trial (like many modern studies) is described as pragmatic. This has pros and cons. The advantages are that it replicates real life clinical practice allowing for variations in decision making (e.g. follow-up imaging in this paper) thus making it generally applicable. The downside of course is the lack of precision that this can introduce with stone passage possibly being only patient reported, or based on ultrasound, plain x-ray, IVU or CT. I guess we have to decide which type of trial we prefer, although it would be very difficult to mandate CT follow-up, with concerns about radiation safety, in this trial if that isn’t part of routine practice. Thus maybe this study is actually applicable to the vast amount of units around the world.
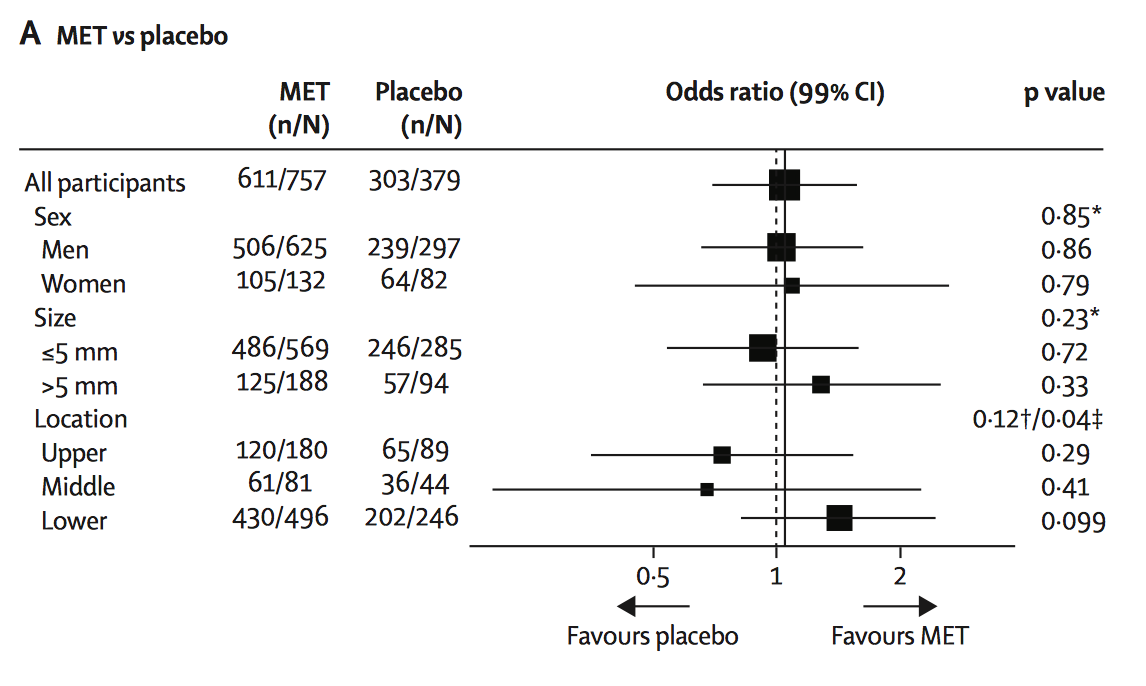
Secondly did it include the right type of patient? Well the current guidelines suggest using MET for any stone measuring up to 1cm in any part of the ureter … and that is what this trial did. And this is thus a strength given that it didn’t just focus on the distal ureter. Thus the trial population seems reasonable. One possibility is that if MET only works in the distal ureter (as almost all the studies only look at this), this could this explain the negative findings. Sub-group analysis of this based on location or stone size seems to suggest not unless it was underpowered to show a difference for this cohort of patients.
Whilst the odds ratios (see table) seem clear, the Forest plot shows the breakdown of subgroup by sex, stone size and location. Whilst not statistically significant, this does suggest a trend towards favouring MET for lower ureteric stones.
Thirdly, is it possible this trial is wrong … a type II error ? Well of course anything is possible, and the trial may be criticised for the follow-up mentioned above. However it does seem to provide easily the best evidence to date. Thus why has the use of MET been allowed to become routine practice based on a number of small trials all introducing inherent bias which is then amplified when a meta-analysis is performed. I guess it was the best evidence around at the time although it makes you wonder how many other interventions there are that we currently use that are based on smallish trials, and would they actually stand up to the rigour of a well conducted big multicentre trial?
My last question is will this change practice again? Well it should, but with no alternative (except time, fluids and NSAID’s) to offer patients with ureteric stones and given that alpha blockers are usually well-tolerated, I wonder whether people will continue to prescribe MET for the foreseeable future. But if we believe in evidence based medicine, and we do, then surely we should no longer prescribe MET for ureteric stones which after all is an off-licence indication.
Finally congratulations must go to the NIHR and the research team for answering a very important clinical question. Was the whole ‘MET’ story a placebo effect all along … or to quote another less well known song title from The Verve, was it “All in the mind”? The conclusion from this excellent study has to be yes.
Conflict of interest: Acted as PI for Guy’s and St. Thomas’ Hospital for this trial recruiting patients although have no part of study design, data analysis or publication.
Matthew Bultitude
Consultant Urologist, Guy’s and St. Thomas’ Hospital
Associate Editor, BJUI
Test yourself against our experts with our weekly quiz. You can type your answers here if you want to compare with our answers.
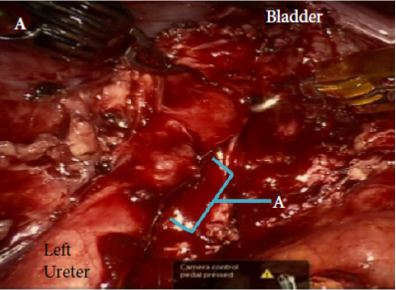
This patient (from Gellhaus et al, BJUI 2015) has suffered an injury from obstetric/gynaecological surgery.
No such quiz/survey/pollEvery Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video from Dr. Naeem Bhojani, discussing his accompanying editorial to the Article of the Week.
If you only have time to read one article this week, it should be this one.
To evaluate efficacy and safety of silodosin in a pooled analysis of individual patient data from three registrational randomised controlled trials (RCTs) comparing silodosin and placebo in patients with lower urinary tract symptoms (LUTS).
PATIENTS AND METHODS
A pooled analysis of 1494 patients from three 12-week, multicentre, double-blind, placebo-controlled phase III RCTs was performed. Efficacy and safety data were assessed across patients with different baseline characteristics. Vertigo is one of the most common health problems in adults. It is a symptom, not a disease and is usually associated with a problem in the inner ear balance mechanisms (vestibular system), in the brain, or with the nerve connections between the two organs. Vertigo can also be brought on suddenly through various actions or incidents, such as sudden changes in blood pressure or as a symptom of motion sickness while sailing, on amusement rides, airplanes or in an automobile. It can be acute and severe, lasting for days, or it may be recurrent, with attacks that last for minutes to hours. Vertigo los angeles associated with panic attacks can sometimes be caused by hyperventilating. For the best treatment for vertigo, do visit us.
Patients often describe balance problems, dizziness, light headedness, and motion sickness. They may also describe an intense or severe sensation of movement, tilting, or imbalance; the sensation is aggravated by movement and improved by remaining stationary. Patients may say that they are having continuous vertigo, when in reality, they are having repeated episodes (with each episode lasting less than a minute). Those with persistent vomiting or intractable vertigo may require admission for hydration and vestibular suppressant medication. These disorders are the ninth most common complaint that leads people to visit their physicians. It is important to not use general terms when describing balance problems. To put it another way, it is best to simply describe the sensation they feel without using general terms like dizziness or vertigo. The cause is often revealed by the patient’s history and physical examination. In migraine-associated vertigo for instance, the patient may report a history of acute-onset vertigo that lasts minutes, a few hours, many hours, or days.
RESULTS
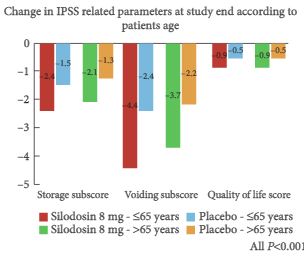
Silodosin was significantly more effective than placebo in improving all International Prostate Symptom Score (IPSS)-related parameters, and maximum urinary flow rate (Qmax) regardless of patients age (P < 0.041). Comparing the efficacy of silodosin in the different age groups, there were no differences for all the IPSS-related parameters, whereas Qmax improvement was slightly higher in patients aged <65 years (P = 0.009). Silodosin was significantly more effective than placebo in reducing all IPSS-related parameters regardless of baseline IPSS (P ≤ 0.001). Similarly, silodosin was more effective than placebo in improving IPSS-related parameters regardless of baseline Qmax (P ≤ 0.02). Silodosin was associated with significantly higher adverse event (AE) rates, compared with placebo, in all patient subgroups, with retrograde ejaculation being the most common. Prevalence of dizziness, orthostatic hypotension, and discontinuation rate was similar with silodosin and placebo in most patient subgroups.
We analysed the efficacy and safety of silodosin in several patient subgroups, showing that silodosin was more effective than placebo in improving all IPSS-related parameters in all patient subgroups, whereas AEs were similar. Notably, cardiovascular AEs were not higher in patients taking antihypertensive drugs or with mild renal function impairment. Discontinuation rates due to AEs were lower in elderly patients.
A significant proportion of aging men will have bothersome LUTS and will eventually seek help for this problem. Various medical therapies are available to help aleviate these symptoms. Amongst the various treatments, α-blockers are some of the most widely used drugs. Novara et al. [1] recently published a report on the efficacy and safety of silodosin in a pooled analysis of individual patient data from three registrational randomized controlled trials comparing silodosin and placebo in patients with LUTS. Their study contributes pertinent information to aid the clinician in determining which α-blocker is best suited for specific patients with LUTS.
In the current study, patients were subdivided into groups in order to better understand which patient would benefit most from the use of silodosin [2]. In addition, the article examines the safety of silodosin in these same distinct patient groups. With regard to efficacy, silodosin was significantly more effective than placebo in improving all IPSS-related variables and maximum urinary flow rate, regardless of the patient’s age. When comparing the efficacy of silodosin in different age groups, no difference was observed for any of the IPSS variables, whereas patients aged <65 years had a statistically significantly greater maximum urinary flow rate.
With regard to safety, silodosin was associated with a significantly higher adverse event (AE) rate compared with placebo. When comparing the safety of silodosin in patients aged <65 years and >65 years, the overall AE rate, ejaculatory dysfunction and discontinuation rate attributable to AEs were all higher in the younger age group. Interestingly, in patients with concomitant use of antihypertensive drugs, the use of silodosin was not associated with a higher risk of either dizziness or orthostatic hypotension.
In a previous study by the same authors, no clinically relevant or statistically significant differences with regard to diastolic blood pressure, systolic blood pressure or heart rate in patients taking silodosin as compared to placebo were found [3]; however, a minor statistically significant difference vs placebo was observed with tamsulosin. The present study by Novara et al. [2] further supports the belief that silodosin is a safe drug from a cardiovascular standpoint.
From a sexual standpoint, silodosin does not seem to perform as well. In the present study, patients in the silodosin group had significantly more adverse events as compared with the placebo group. Retrograde ejaculation was by far the most common side effect affecting 32.8% of patients aged <65 years vs 0.9% in the placebo group. Similarly, in a study by Chapple et al. [3], as many as 14.2% of patients in the silodosin treatment group had ejaculatory dysfunction, compared with 2.1 and 1.1% of patients in the tamsulosin and placebo treatment groups, respectively. Although the percentage of patients who discontinued treatment because of treatment-emergent AEs in the present study was small and not significantly different among all treatment groups, one might hypothesize that over a longer follow-up period, such a prevalent side effect could be responsible for a higher discontinuation rate. Consequently, it should be kept in mind that for patients desiring to maintain antegrade ejaculation, or who are bothered by treatment-onset ejaculatory dysfunction, especially younger patients, silodosin might not be the best treatment option. Furthermore, it should be recognized that some patients would potentially accept a reduction in treatment efficacy to preserve ejaculation [4].
With regard to clinical outcomes, few published papers comparing tamsulosin with silodosin are available [5, 6]. One article found no clinically significant difference between the two α-blockers [5] whereas the other, which was a post hoc analysis, found a marginal clinical benefit for silodosin over tamsulosin [4]. Unfortunately, head-to-head trials are not forthcoming, so it will not be possible to determine if one α-blocker is clinically better than the other. Furthermore, the present study, because it lacked an active control arm, did not compare silodosin with tamsulosin, which leaves something to be desired.
In conclusion, careful consideration should be given to specific patient characteristics such as age and comorbidities, along with personal preferences towards sexual function when offering patients α-blockers for treatment of LUTS.
A significant proportion of aging men will have bothersome LUTS and will eventually seek help for this problem. Various medical therapies are available to help aleviate these symptoms. Amongst the various treatments, α-blockers are some of the most widely used drugs. Novara et al. [1] recently published a report on the efficacy and safety of silodosin in a pooled analysis of individual patient data from three registrational randomized controlled trials comparing silodosin and placebo in patients with LUTS. Their study contributes pertinent information to aid the clinician in determining which α-blocker is best suited for specific patients with LUTS.
In the current study, patients were subdivided into groups in order to better understand which patient would benefit most from the use of silodosin [2]. In addition, the article examines the safety of silodosin in these same distinct patient groups. With regard to efficacy, silodosin was significantly more effective than placebo in improving all IPSS-related variables and maximum urinary flow rate, regardless of the patient’s age. When comparing the efficacy of silodosin in different age groups, no difference was observed for any of the IPSS variables, whereas patients aged <65 years had a statistically significantly greater maximum urinary flow rate.
With regard to safety, silodosin was associated with a significantly higher adverse event (AE) rate compared with placebo. When comparing the safety of silodosin in patients aged <65 years and >65 years, the overall AE rate, ejaculatory dysfunction and discontinuation rate attributable to AEs were all higher in the younger age group. Interestingly, in patients with concomitant use of antihypertensive drugs, the use of silodosin was not associated with a higher risk of either dizziness or orthostatic hypotension.
In a previous study by the same authors, no clinically relevant or statistically significant differences with regard to diastolic blood pressure, systolic blood pressure or heart rate in patients taking silodosin as compared to placebo were found [3]; however, a minor statistically significant difference vs placebo was observed with tamsulosin. The present study by Novara et al. [2] further supports the belief that silodosin is a safe drug from a cardiovascular standpoint.
From a sexual standpoint, silodosin does not seem to perform as well. In the present study, patients in the silodosin group had significantly more adverse events as compared with the placebo group. Retrograde ejaculation was by far the most common side effect affecting 32.8% of patients aged <65 years vs 0.9% in the placebo group. Similarly, in a study by Chapple et al. [3], as many as 14.2% of patients in the silodosin treatment group had ejaculatory dysfunction, compared with 2.1 and 1.1% of patients in the tamsulosin and placebo treatment groups, respectively. Although the percentage of patients who discontinued treatment because of treatment-emergent AEs in the present study was small and not significantly different among all treatment groups, one might hypothesize that over a longer follow-up period, such a prevalent side effect could be responsible for a higher discontinuation rate. Consequently, it should be kept in mind that for patients desiring to maintain antegrade ejaculation, or who are bothered by treatment-onset ejaculatory dysfunction, especially younger patients, silodosin might not be the best treatment option. Furthermore, it should be recognized that some patients would potentially accept a reduction in treatment efficacy to preserve ejaculation [4].
With regard to clinical outcomes, few published papers comparing tamsulosin with silodosin are available [5, 6]. One article found no clinically significant difference between the two α-blockers [5] whereas the other, which was a post hoc analysis, found a marginal clinical benefit for silodosin over tamsulosin [4]. Unfortunately, head-to-head trials are not forthcoming, so it will not be possible to determine if one α-blocker is clinically better than the other. Furthermore, the present study, because it lacked an active control arm, did not compare silodosin with tamsulosin, which leaves something to be desired.
In conclusion, careful consideration should be given to specific patient characteristics such as age and comorbidities, along with personal preferences towards sexual function when offering patients α-blockers for treatment of LUTS.
The urology section of the RSM left Wimpole Street and travelled up to sunny Queen Elizabeth Hospital in Birmingham on the 24th April to be educated in the ‘Management of Non-Muscle invasive and Muscle Invasive Bladder Cancer’. This meeting was organised in collaboration with Nick James and Rik Bryan at the Birmingham Warwick Uro-Oncology unit as the RSM looks to add to its regional programme of teaching days.
The meeting was well attended by both experts as well as trainees and we kicked off with John McGrath and a review of the evidence behind current haematuria investigations as well as the new NICE guidelines. Professor Charles Hutchinson from the University of Warwick then gave a detailed talk on pre-operative imaging in bladder cancer and this led to an interesting debate on the necessity of performing a full TURBT in cases of known muscle invasive disease if the patient will ultimately require a cystectomy. No consensus was reached although if definitely proceeding to cystectomy it is unlikely to be beneficial. If radiotherapy is considered then debulking is important.
Eva Comperat from the Service d’Anatomie and Cytologie Pathologiques du Pr Capron presented a fascinating histopathological perspective of bladder cancer and it was interesting to see that even amongst eminent pathologists there can be challenges in distinguishing pTa from pT1 disease with only 44% in one large study showing full agreement. The importance in reporting histological variants such as micropapillary or plasmocytoid was discussed due to the aggressive nature of these types and the need for more radical treatment. This was also re-iterated by Peter Rimington while discussing early cystectomy which should be offered to all suitable patients at high risk of progression according to EORTC tables, especially in young patients and in tumours which are multifocal, difficult to resect, have deep lamina propria or prostatic involvement and those with associated CIS.
A highlight for me was Professor John Kelly’s talk on the treatment option of hyperthermic Mitomycin C. HYMN Trial.
Data from the HYMN trial which looked at hyperthermic MMC vs. standard treatment in BCG failures was disappointing in that there was no difference in terms of disease free survival at 24 months. Outcomes were found to be worse in patients with CIS, but in patients with papillary disease, hyperthermic MMC had far more favourable results. This has led to the HIVEC I and HIVEC II trials currently recruiting in the UK and Spain looking at standard MMC vs. hyperthermic MMC in intermediate risk disease. It was also interesting to see new immunotherapy drugs currently in phase III trials which will hopefully be available in the near future.
Rik Bryan’s presentation on the evolving role of bio markers explained that the Bladder Cancer Diagnostic Programme had found that contrary to our beliefs, patients trust, and would rather accept certainty over burden and thus would rather continue with cystoscopic surveillance over bio-markers, unless the sensitivity of these bio-markers was over 99%. No such bio-marker has yet been found to be that accurate but current research into odor-readers, urinary dipsticks and DNA all look promising in terms of potential for both diagnosis and prognosis.
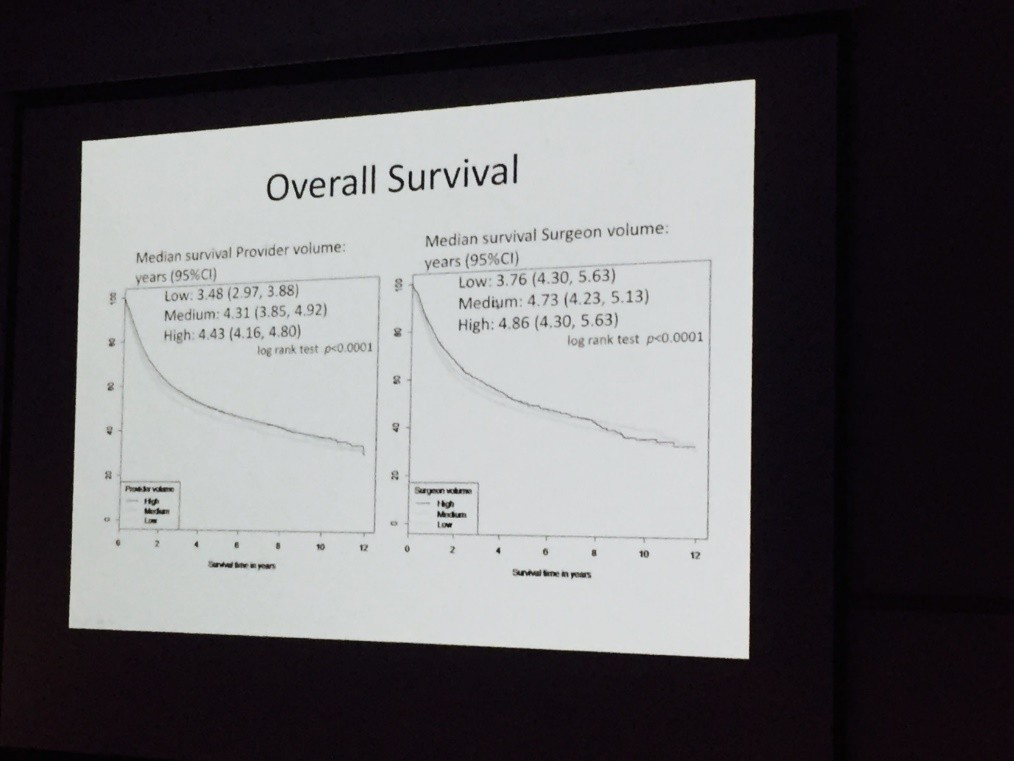
Both Nick James and Hugh Mostafid highlighted current research trials with the CALIBER RCT on chemo resection in recurrent low risk bladder cancer as well as the PHOTO trial looking at both clinical and cost effectiveness of photo-dynamic cystoscopy leading the way in terms of surgical trials currently recruiting. Nick also caused a stir on Twitter as he presented data showing a median survival advantage of more than a year between surgeons performing low or high volume of cystectomies annually. Surely we do not need more convincing evidence to centralise such surgery?
Reviewing bladder cancer from the oncologist’s perspective, Syed Hussein from the University of Liverpool explained that although there is a 6% overall survival benefit with neo-adjuvant chemotherapy there have been no RCT on MVAC vs gemcitabine/cisplatin regimes. Nick James’ talk on bladder preserving treatment added to this that synchronous chemoradiotherapy could be complementary to neo-adjuvant treatment and the addition of synchronous chemotherapy has been shown to provide a significant improvement in terms of loco regional control.
Vijay Ramani presented his series on salvage cystectomy with no significant difference in terms of complications for salvage vs. primary surgery as long as certain techniques were adopted such as division of ureters outside of the pelvis and using bowel at least 15-20cm proximal from the ileocaecal valve.
To complete the diverse and stimulating programme, Professor Peter Wiklund from the Karolinska University Hospital, Stockholm, presented a state of the art lecture on “Reconstruction rules! The robot has taken over?”. With discussion and impressive videos demonstrating intra-corporeal robotic neobladder reconstruction it was difficult not to be in awe of such an impressive series, with a 90% continence rate in males.
Overall it was fantastic to have the RSM in the West Midlands. Roger Plail has done much to reach out to those of us outside of London and I look forward to the Geoffrey Chisholm Prize Meeting and AGM on the 22nd May in Hastings. RSM President’s Day.
Rebecca Tregunna, Speciality Trainee, Burton Hospitals NHS Foundation Trust, West Midlands Deanery @RebeccaTregunna