Editorial: ‘Discontent is the first necessity of progress’, Thomas A. Edison
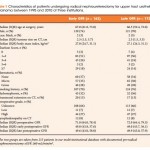
This study from Kaag et al. [1] investigates predictors of renal functional decline after radical nephroureterectomy (RNU) in patients with upper tract urothelial carcinoma (UTUC). They evaluate early (2 months) and late (6 months) predictors of renal functional decline, finding that on a multivariable model only age at surgery and preoperative renal function were independently associated with early postoperative function. This is an intuitive finding whereby we expect older patients and those with lower renal function to have a more dramatic decrease in renal function after RNU.
Age, preoperative renal function, and Charlson score were associated with late functional recovery. The latter is a counterintuitive finding, as higher Charlson score was associated with less decrease in renal function. Charlson comorbidity was not significant on univariate analyses. Why it would become significant on multivariate is unclear. Whether it is an artifact related to study methodology or is a real phenomenon will require further study.
Unquestionably, this study [1] adds to the growing discontent of our current management of UTUC. The authors cogently discuss the issues related to better risk stratification as a natural consequence of instituting a neoadjuvant chemotherapy paradigm in those with high-risk disease. Multiple retrospective studies have failed to show a benefit of adjuvant chemotherapy, whereas now we have a matched-cohort study showing significant rates of downstaging and complete remission [2], and as well significantly improved 5-year survival, with institution of a neoadjuvant paradigm [3]. One cannot view the dismal outcomes of this disease without being discontent and wishing for progress. We need to continue getting out the message to not only urologists who reflexively institute RNU in patients with a risk-unstratified upper tract filling defect, but as well many medical oncologists who can only function based on guidance from level I data, which for this disease, will be a long time coming.
Surena F. Matin
Department of Urology, MD Anderson Cancer Center, Houston, TX, USA
References
1 Kaag M, Trost L, Thompson RH et al. Pre-operative predictors of renal function decline following radical nephroureterectomy for upper tract urothelial carcinoma. BJU Int 2014; 114: 674–9
2 Matin SF, Margulis V, Kamat A et al. Incidence of downstaging and complete remission after neoadjuvant chemotherapy for high-risk upper tract transitional cell carcinoma. Cancer 2010; 116: 3127–34
3 Porten S, Siefker-Radtke AO, Xiao L et al. Neoadjuvant chemotherapy improves survival of patients with upper tract urothelial carcinoma. Cancer 2014; 120: 1794–9